When food or liquid enters the laryngeal vestibule but, unlike with aspiration, does not descend below the level of the vocal cords themselves. Laryngeal penetration alone would be an indication of mild swallowing dysfunction, but it would not by itself create a risk of pneumonia, as aspiration might.
Laryngeal penetration (1 of 1)
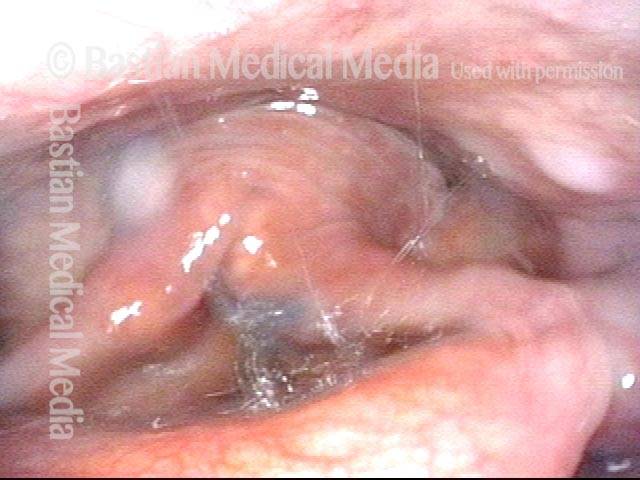
After the patient swallowed several boluses of blue-stained applesauce, there were traces visible on the laryngeal surface of the epiglottis, indicative of penetration into the earliest part of the airway. By itself, soiling of the laryngeal vestibule to this minor degree does not threaten the person’s ability to eat by mouth.
All It Takes Is A Drip to Make You Cough
Coughing (1 of 4)
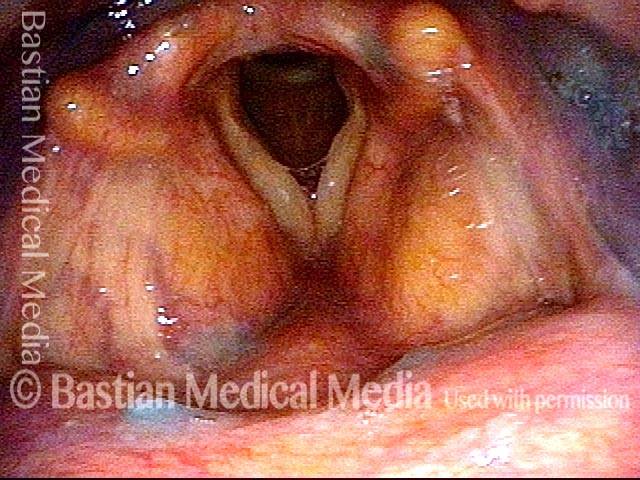
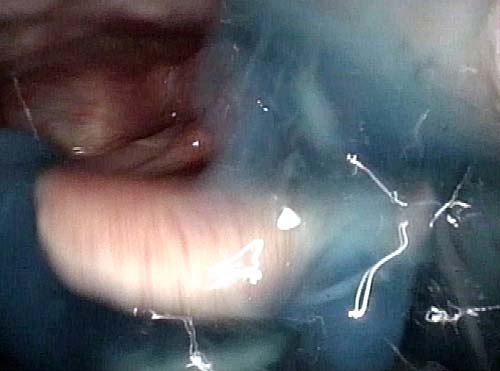
This patient is annoyed by occasional coughing when she sips liquids. She has had no pneumonias, weight loss, or increased time required to eat/drink. Here, the patient has just taken a sip of blue water and holds it in her mouth.

Coughing (2 of 4)
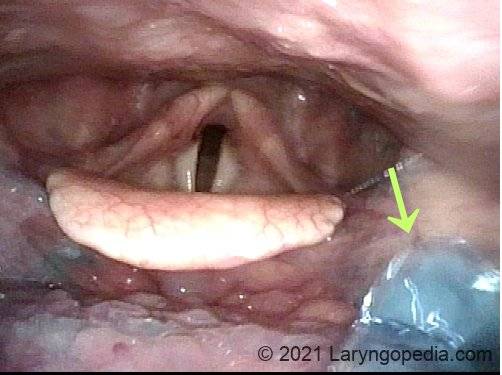
Just before swallowing, a tiny drip of blue water “gets away” and begins to trickle down into her throat. Vocal cords remain unsuspectingly open.
Coughing (3 of 4)
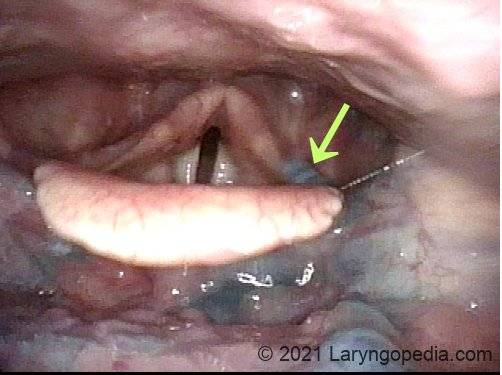
The drip (arrow) has now reached the left aryepiglottic fold, which is the “side of the boat” that keeps liquid out of the airway. The drip looks smaller than in photo 2 because it is farther away. She does not cough.
Coughing (4 of 4)
During a different swallow, if a much larger amount of water were to drip prematurely down into her throat, a part of it would enter the laryngeal entrance and provoke coughing. If coughed back up, there would be little risk of pneumonia.
VESS Demonstrating Presbyphagia, Chin Tuck Maneuver, Hypopharyngeal Pooling, Laryngeal Penetration and Effective Cough
VESS (1 of 5)
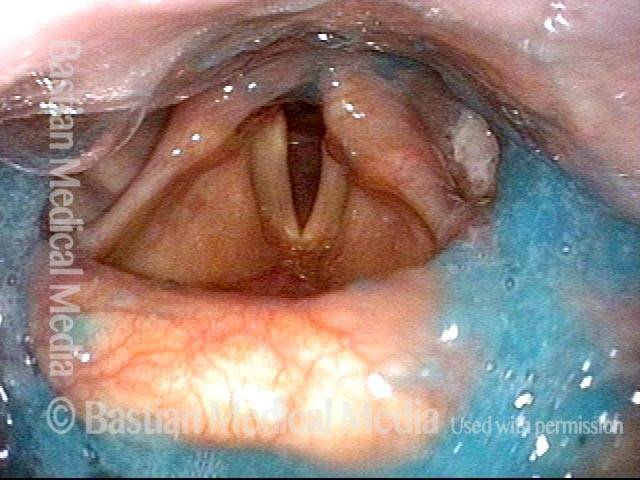
The patient swallowed a bolus of blue-stained applesauce to verify basic (though abnormal) capability. This photo follows 4 additional boluses delivered in a rapid, pressured fashion, intentionally seeking the patient’s “limits.” Note pooled blue applesauce, but without soiling of the laryngeal vestibule.
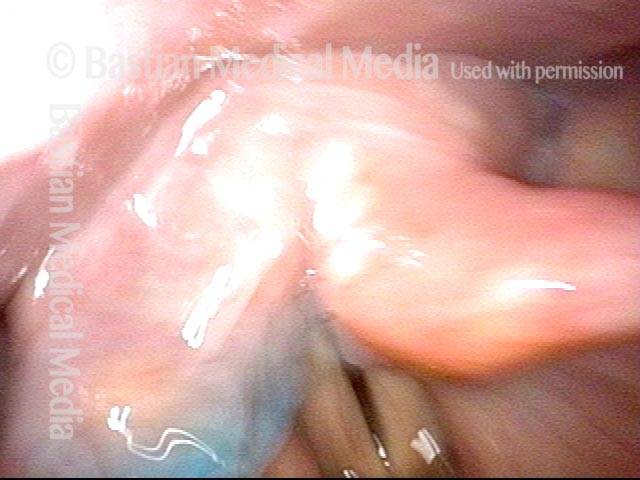
Chin tuck maneuver (2 of 5)
Moments later, the patient was asked to swallow again, but with chin tucked down towards chest. Note how effective this maneuver was in clearing away the residual material seen in the prior photo.

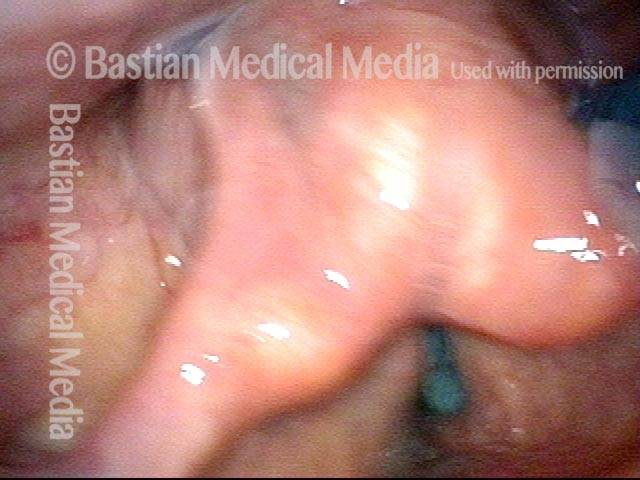
Aspiration (3 of 5)
Due to its lower viscosity, blue-stained water flows more quickly than applesauce, and enters the laryngeal vestibule. Fortunately, the patient is closing the vocal cords simultaneously, so that aspiration does not occur.
Laryngeal penetration (4 of 5)
Just after the swallow is completed, one can see a trace of blue-stained water just above the not-yet-opened cords. This is technically penetration, and not aspiration.
Air is blasted out of vestibule (5 of 5)
Using “stored” pulmonary air, this trace of penetrated water is “blasted” up and out of the laryngeal vestibule, and is never aspirated.”