Photos of SNC
A collection of photo essays demonstrating SNC in various patients.Bruising from Sensory Neuropathic Cough
Closer view of bruise (2 of 2)
Closer view of bruise, with small collection of white mucus in the middle.
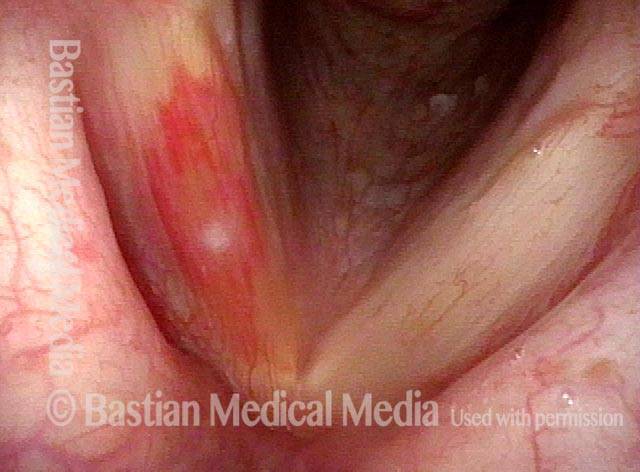
Bruise caused by violent coughing (1 of 2)
A person with violent sensory neuropathic coughing may injure the vocal cords, as illustrated by this bruise, right vocal cord (left of photo).
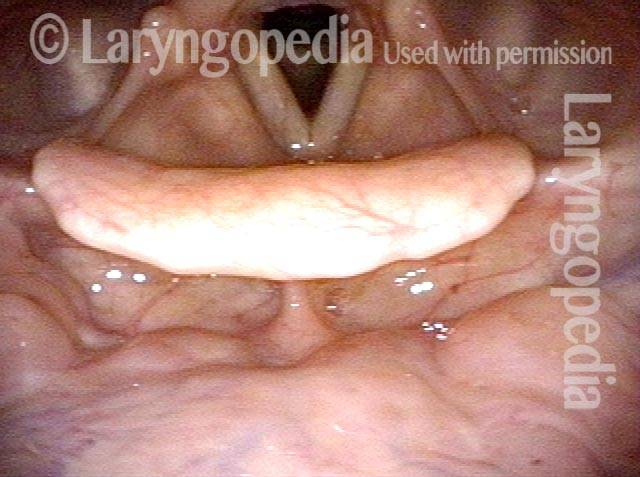
Example 2
Bruise from coughing (1 of 3)
This man had an episode of aggressive coughing a week earlier. Note the bruising over the vocal processes, which receive the major collisional force during coughing.

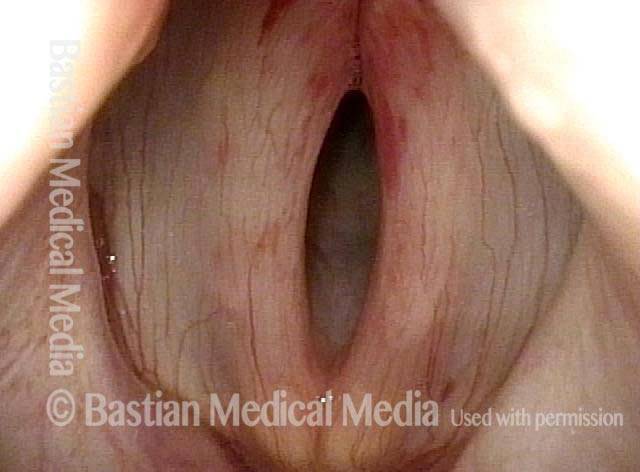
Pre-phonatory instant (2 of 3)
The vocal processes are approaching the point of touching (contact would occur gently with onset of talking and more aggressively with coughing).

Phonation (3 of 3)
Vocal cords are now in full contact. Note the unrelated moderately-severe vocal cord bowing.
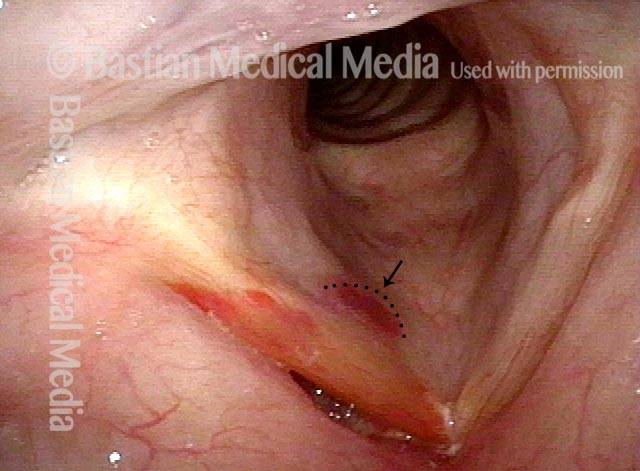
Example 3
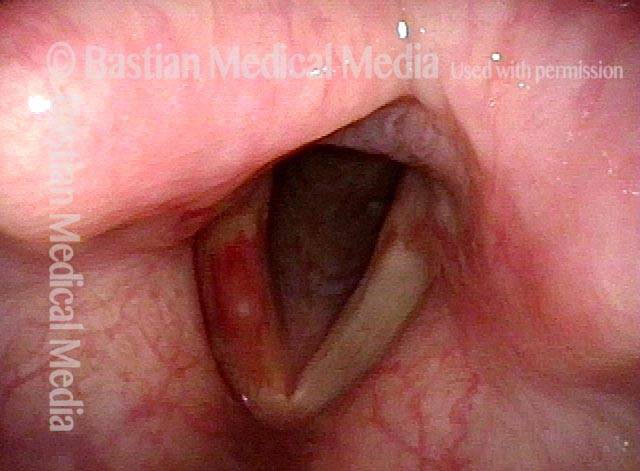
Bruising from SNC (1 of 1)
This individual occasionally coughs to the point of hoarseness. Particularly noteworthy is the subglottic bruise (arrow, dotted line) caused by profound Valsalva-retching kind of coughing. The rest of the right cord (left of photo) is also bruised.
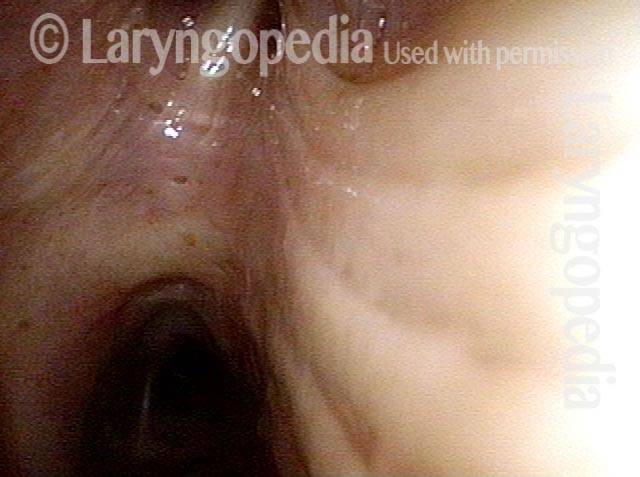
Hemoptysis
SNC patient (1 of 6)
A very worried patient with sensory neuropathic cough has scheduled a return appointment. On arrival she states that she cannot rest due to a trace of hemoptysis a week earlier. What begins as a simple upper aerodigestive tract examination represented by this view of her normal nasopharynx is easily expanded…

Panoramic view (2 of 6)
Detailed inspection of base of tongue, hypopharynx, and laryngeal vestibule, represented by this panoramic view, also show no abnormality. And the examination can continue…
Lidocaine (3 of 6)
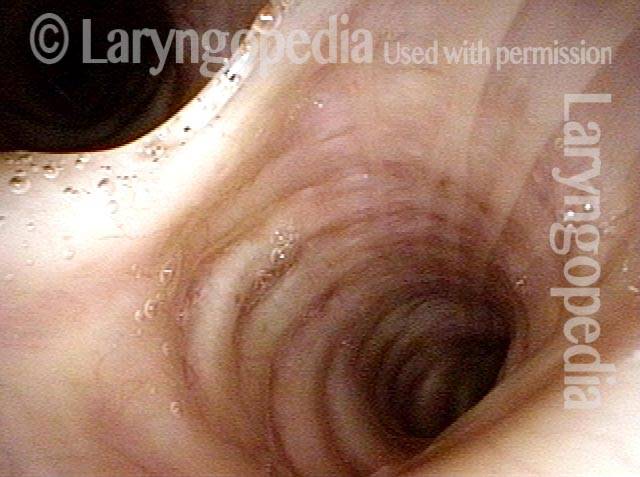
Simple instillation of lidocaine into the trachea allows this view into the upper trachea.

Carina (4 of 6)
And this view, with the carina in clear view.

Right mainstem bronchus (5 of 6)
Deep inside right mainstem bronchus and…
Left mainstem bronchus (6 of 6)
…into left mainstem bronchus also reveal no lesions and no “trail of blood.” Simple watchful waiting for more hemoptysis is acceptable to the patient. CXR is optional in the near-term.