Videofluoroscopic swallowing study (VFSS) is an x-ray-based method of evaluating a person’s swallowing ability. VFSS is also sometimes called the modified barium swallow, or the “cookie swallow.”
In a radiology suite under fluoroscopy (which creates moving rather than still x-ray images), the patient is asked to swallow barium in thin liquid and paste consistencies, and then in paste on a cookie or cracker. The barium bolus is followed radiographically through the mouth, throat, and into the esophagus. Both lateral and anterior–posterior views are recorded and, depending on the facility, a simple screening sequence of the subsequent movement down the esophagus is also recorded.
Cricopharyngeal Dysfunction, before and after Myotomy
Cricopharyngeal dysfunction: before myotomy (1 of 2)

Cricopharyngeal dysfunction: after myotomy, resolved (2 of 2)

Example 2
Cricopharyngeal dysfunction: before myotomy (1 of 2)

Cricopharyngeal dysfunction: after myotomy, resolved (1 of 2)

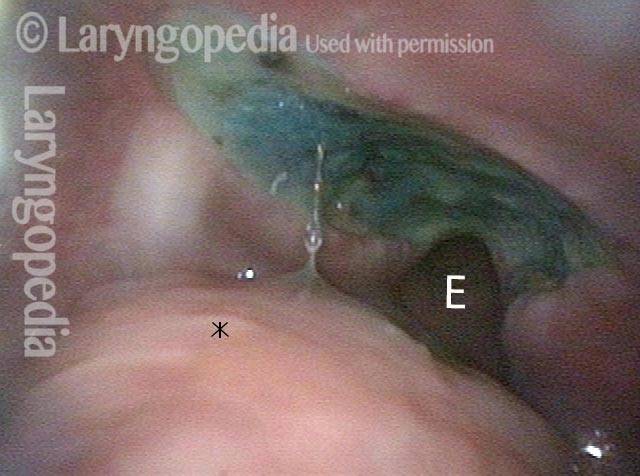
R-CPD, Aerophagia and Burping
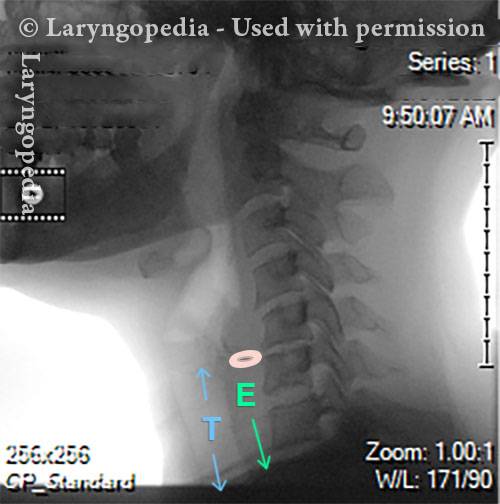
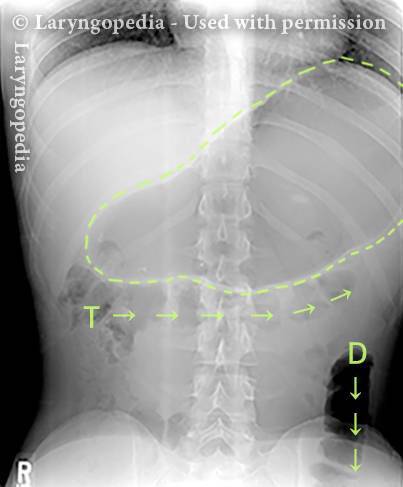
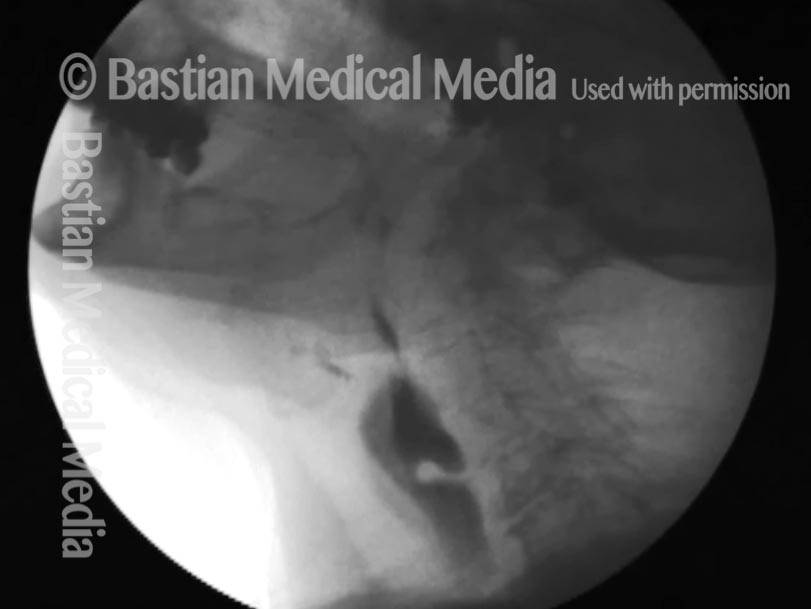
This lateral x-ray of the neck is part of a swallow study, and illustrates how air can accumulate and need to be burped up. The focus of this photo essay is the esophagus, or “foodway,” that connects the lower part of the throat to the stomach. The esophagus is a muscular tube that remains mostly collapsed—closed—except when food, liquid, or saliva traverses it. Read more about esophageal findings of R-CPD.
X-Ray of Larynx (1 of 6)
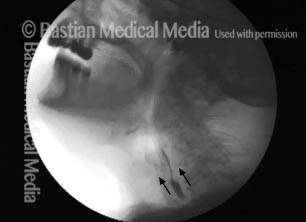
Barium swallow (2 of 6)

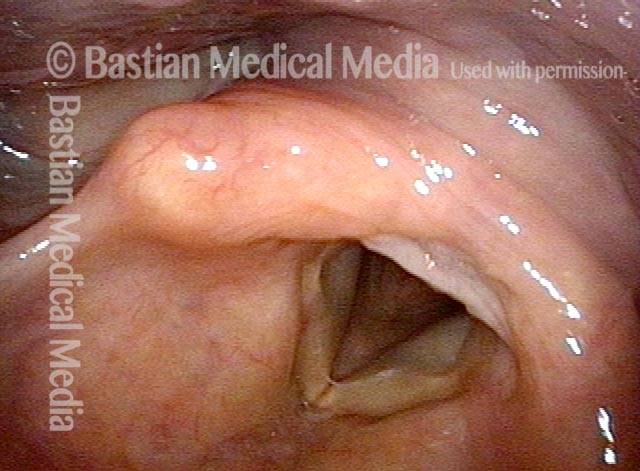
Collapsed esophagus (3 of 6)

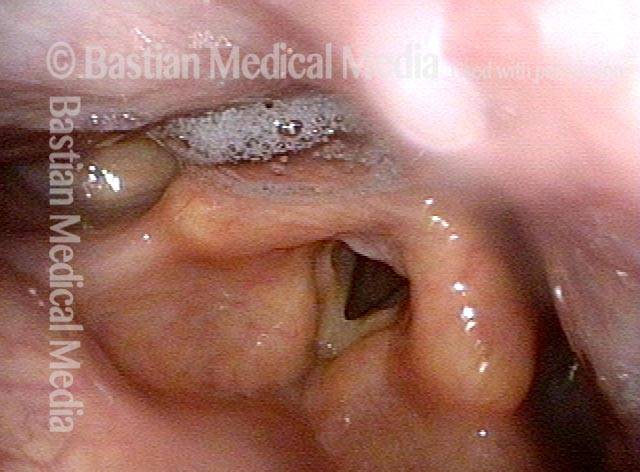
Air is swallowed (4 of 6)
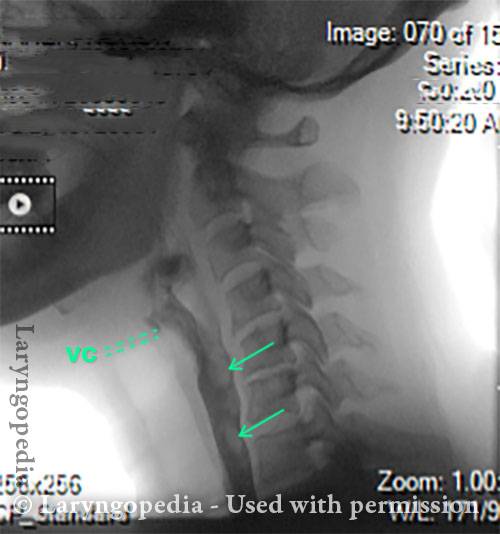
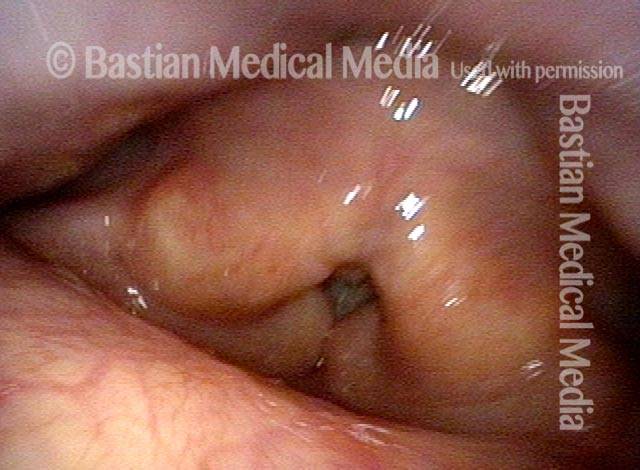
UES refuses to open for a burp (5 of 6)

Abdominal Distention from R-CPD (6 of 6)
Post-swallow Hypopharyngeal Reflux (Zenker’s Diverticulum): VESS vs. VFSS
VESS (1 of 7)

Reflux (2 of 7)

Post-swallow (3 of 7)
Reflux of cracker (4 of 7)

VFSS (5 of 7)

X-Ray (6 of 7)

Continued reflux (7 of 7)

Great View of Fresh Cricopharyngeus Myotomy Surgical Wound
CPM dysfunction (1 of 4)
VFSS six years later (2 of 4)

Five days post-op (3 of 4)
Cervical esopagus (4 of 4)
98 Year-old before and after Myotomy
Immediately after swallowing (1 of 10)
Zenker’s (2 of 10)
Dysphagia (3 of 10)
Residue from Zenker’s (4 of 10)

X-ray showing Zenker’s (5 of 10)
Moments later (6 of 10)
After myotomy (7 of 10)
No residue (8 of 10)

Zenker’s gone (9 of 10)

No barium in hypopharynx (10 of 10)