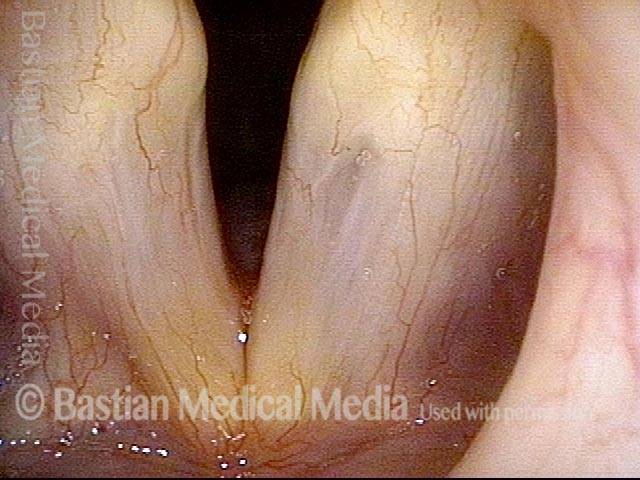
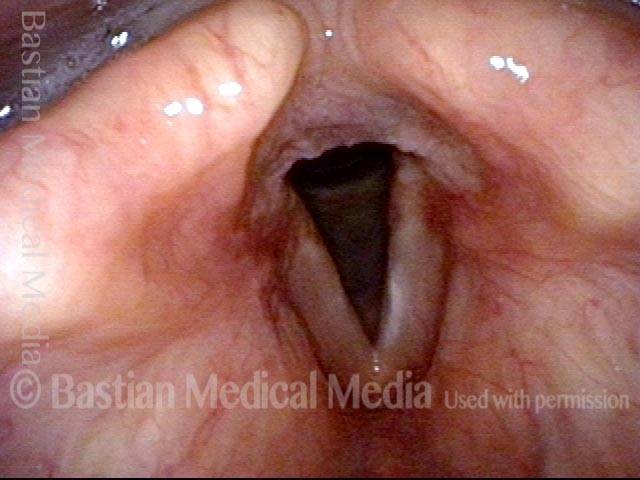
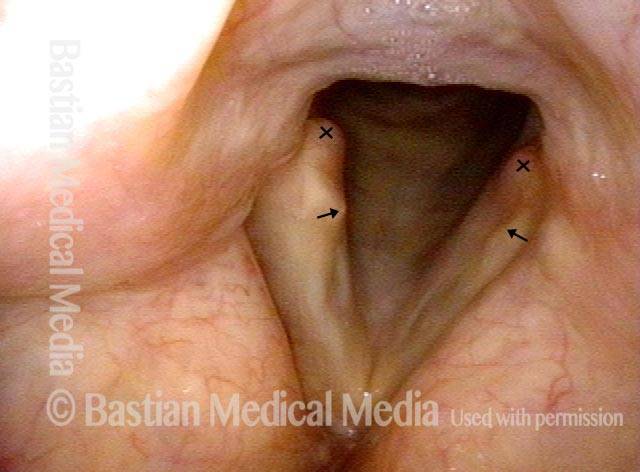
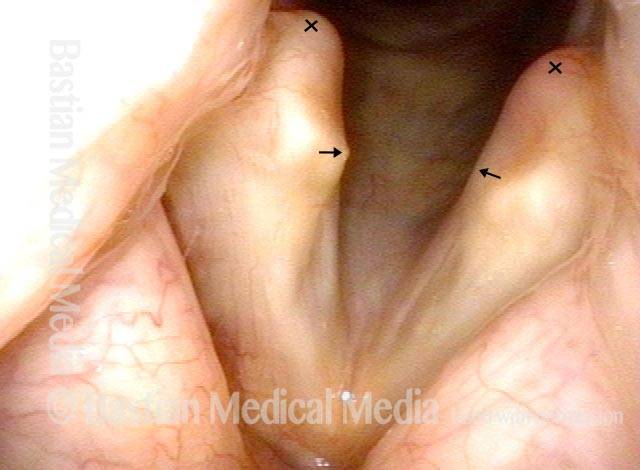
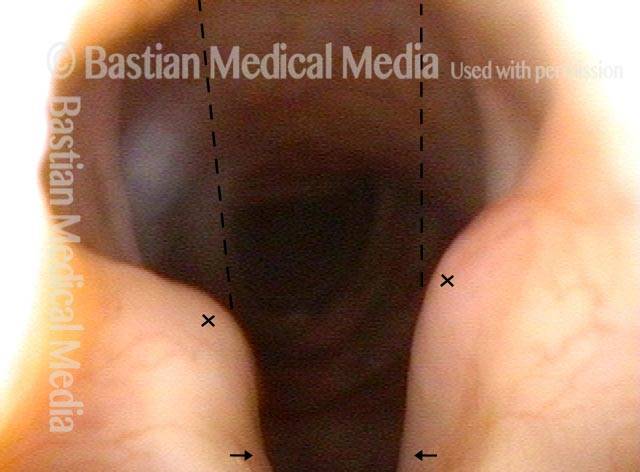
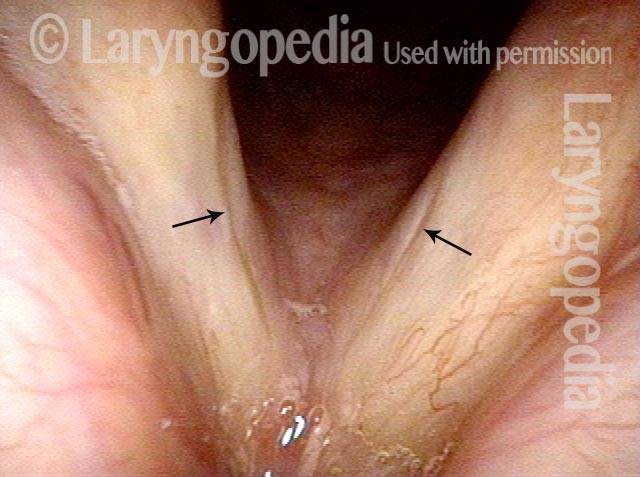
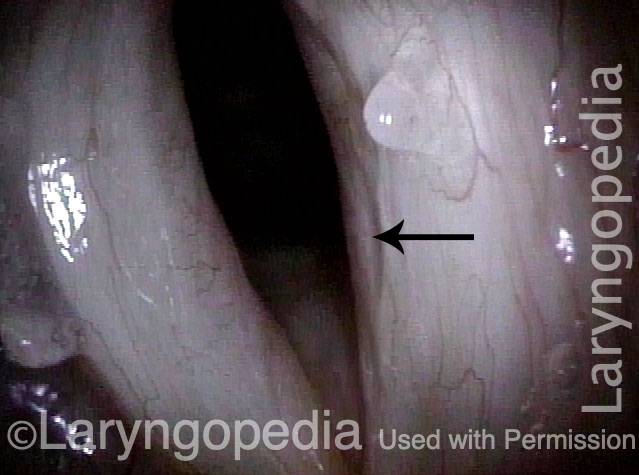
Glottic furrow is a disorder in which a furrow or groove is seen on the vocal cord, running parallel to, and at or just below, the cord’s free margin. It normally represents a defect in the underlying vocal ligament. Often, the deepest part of the furrow is lined with epithelium that is attached directly to thinned vocal ligament. Pseudobowing (due to mucosal and ligament abnormality more than atrophic muscle) is also a common feature.
Glottic furrow vs. glottic sulcus
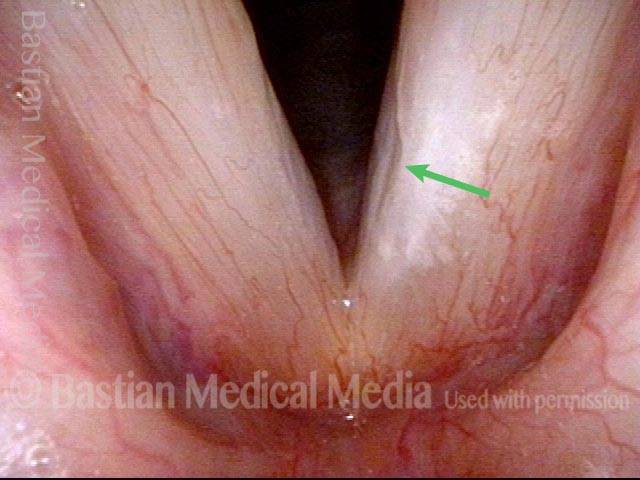
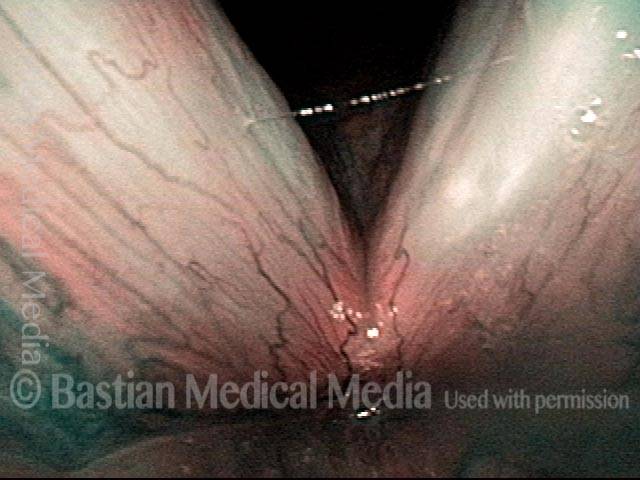
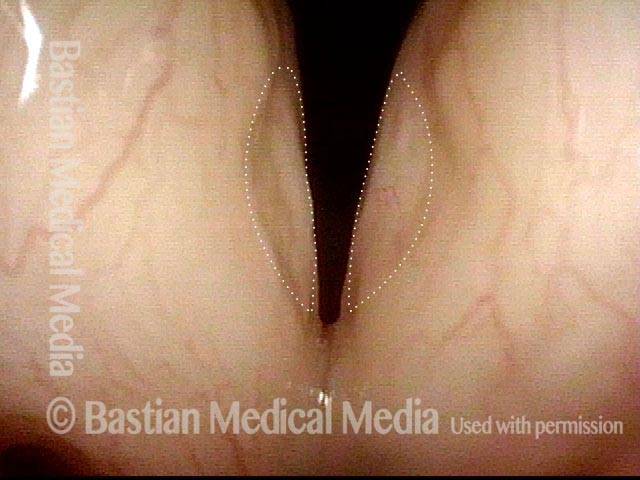
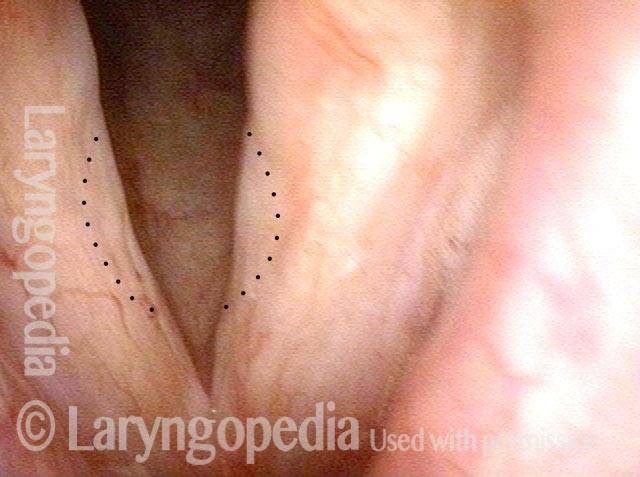
A furrow is to be distinguished from a sulcus, which is more a defect within the mucosal layer only, and is thought to represent the empty sac of what was formerly a cyst. A furrow is typically shallow, and its lips are apart; a sulcus is usually deeper, and its lips are in contact and therefore harder to see. A furrow normally adheres to the vocal ligament, and the apex or deep surface of a sulcus often does as well. However, in the case of a sulcus, the vocal ligament itself is normal. Also, in the case of a furrow, the mucosal layer—often only an epithelial layer, in fact—will tend to adhere more broadly to the ligament, due to loss of the Reinke’s space layer of the mucosa.
Glottic sulcus and glottic furrow (1 of 4)
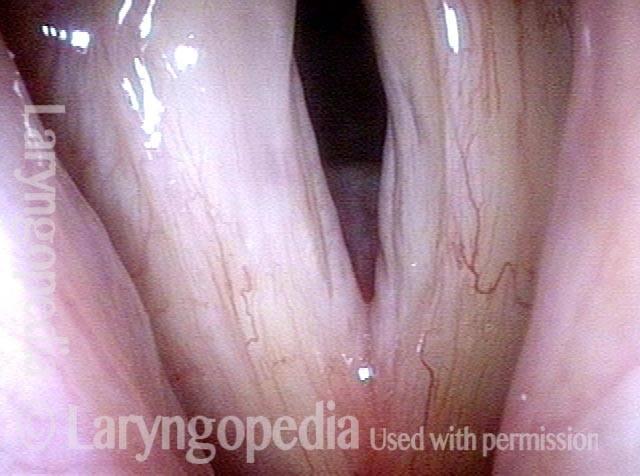
Glottic sulcus and glottic furrow (2 of 4)

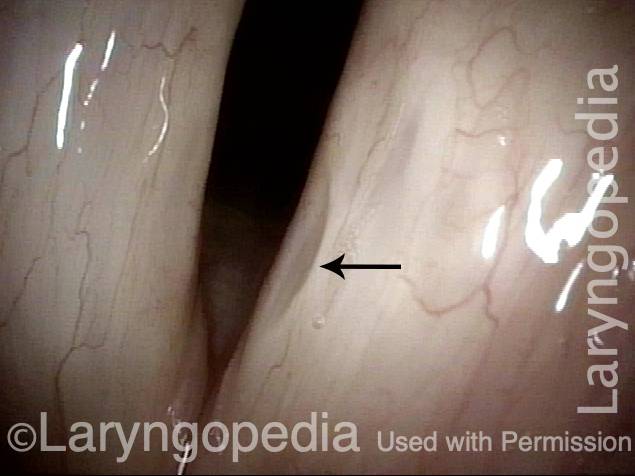
Glottic sulcus and glottic furrow (3 of 4)

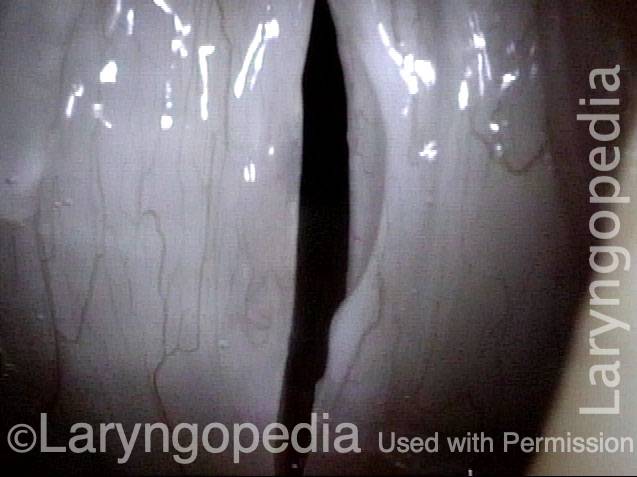
Glottic sulcus and glottic furrow (4 of 4)
Glottic Furrow
Glottic furrow (1 of 4)

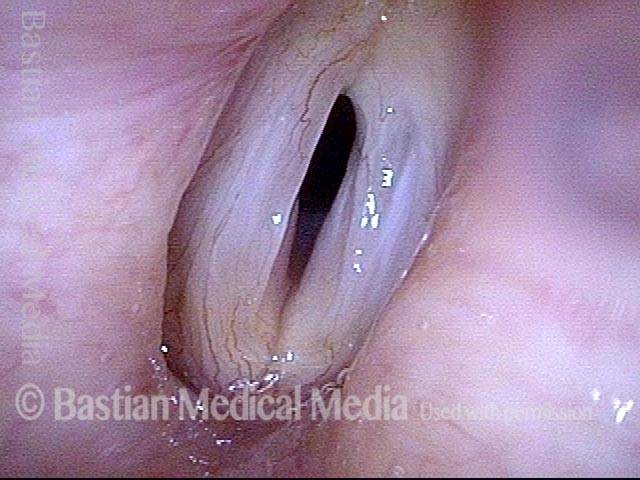
Glottic furrow (2 of 4)
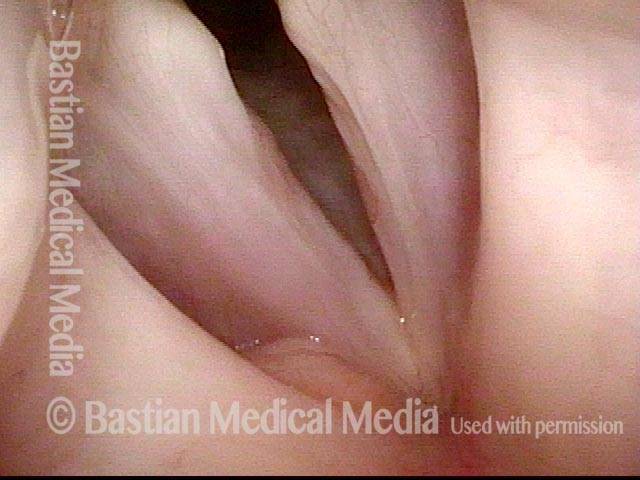
Glottic furrow (3 of 4)
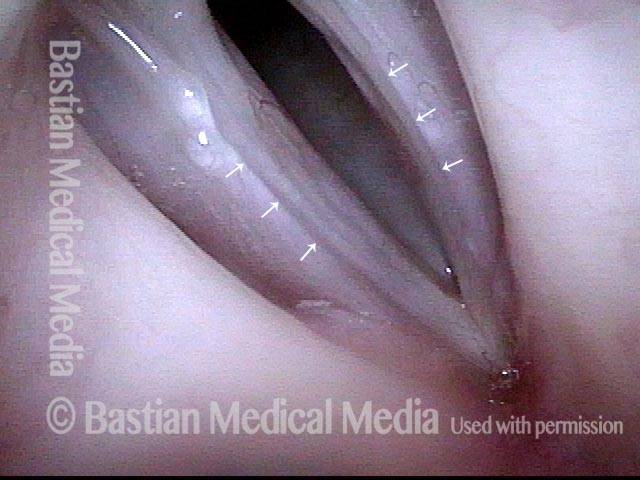
Glottic furrow (4 of 4)

Glottic Furrow / Leukoplakia / Acid Reflux
Glottic furrow / Leukoplakia / Acid reflux (1 of 4)
Leukoplakia (2 of 4)
Glottic furrows (3 of 4)
Gap during closed phase (4 of 4)

Glottic Furrow, Showing Adherent Furrow Muscoa
Glottic furrow, showing adherent furrow muscoa (1 of 4)

bilateral glottic furrows (2 of 4)
medial oscillatory position (3 of 4)
Mucosal Wave (4 of 4)

Glottic Furrow—A Thinning of Reinke’s Space
Glottic furrow (1 of 4)
Strobe light (2 of 4)
High pitch (3 of 4)

Thinning of Reinke's space (4 of 4)
Double Whammy: Intubation Injury + Glottic Furrows
Intubation injury + glottic furrows (1 of 4)
Bilateral glottic furrows (2 of 4)
Intubation injury (3 of 4)
Phonatory position (4 of 4)

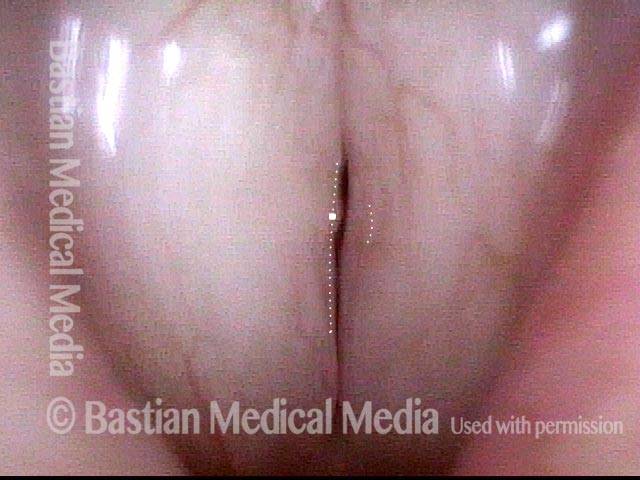
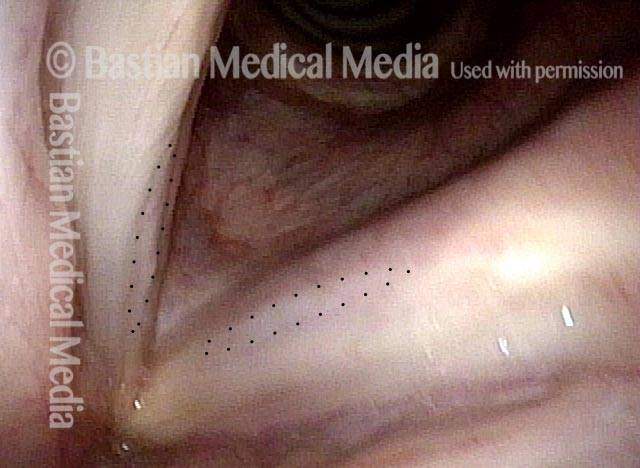
Furrow Causing Chronically Husky Voice After Years of Extensive and Often Intense Voice Use
Huskiness (1 of 4)

Pre-phonatory view (2 of 4)
Depressed area (3 of 4)

High pitch (4 of 4)

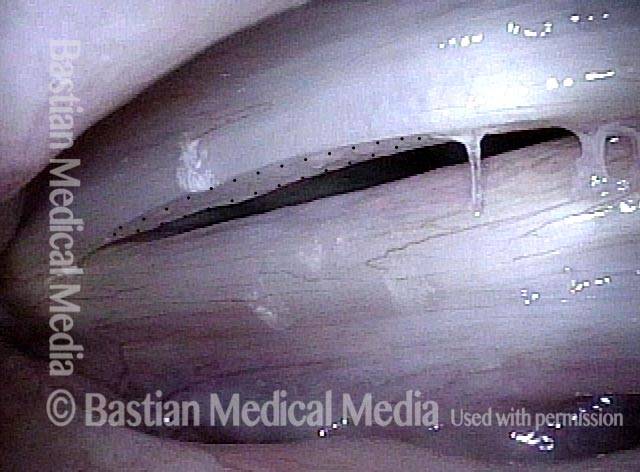
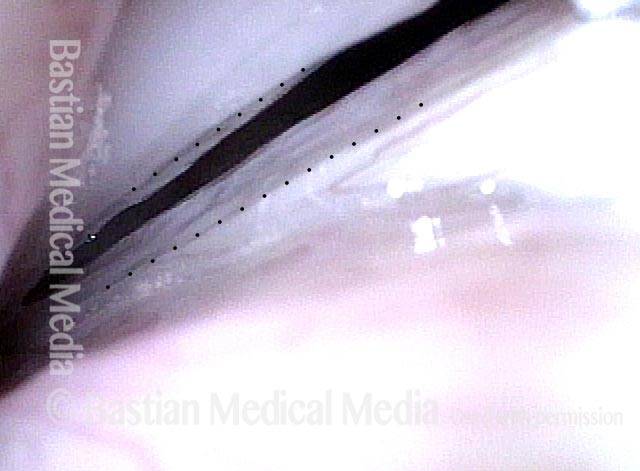
Glottic Furrow—Not Just Bowing and not Glottic Sulcus
Bowing vocal cords with furrows (1 of 4)
Closed phase (2 of 4)

Open phase (3 of 4)
Lower pitch reveals furrow (4 of 4)

Glottic Furrow—Not Sulcus
A rough and fuzzy voice (1 of 6)
Furrow (2 of 6)

asymmetrical vibration (3 of 6)
Closed phase ( 4 of 6)

vibration points amplify (5 of 6)
Furrow (6 of 6)
