The term muscular tension dysphonia (MTD) was coined by Morrison and Rammage at the University of British Columbia. This is a syndrome consisting of some or all of the following:
1) Excess tension, sometimes to the point of discomfort/ pain in the paralaryngeal and suprahyoid muscles;
2) An open posterior glottic chink during phonation;
3) High larynx position in the neck;
4) Inappropriate contraction of pharyngeal constrictors with phonation;
5) Often but not always, vibratory mucosal injury.
The vocal cord mucosal changes associated with MTD are usually fleshy vocal nodules. This syndrome is seen most often in young women.
Inappropriate Pharynx Contraction Is A Component of (MTD)
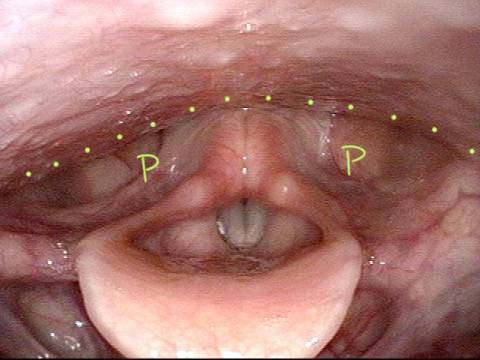
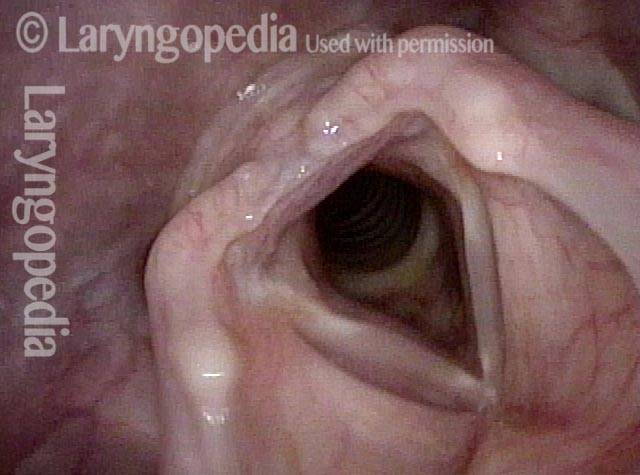
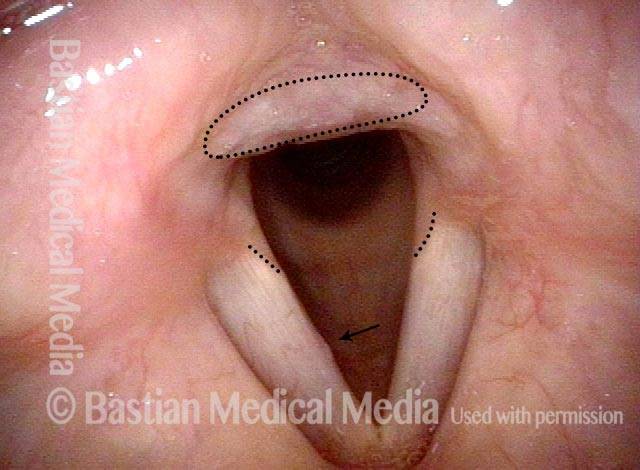
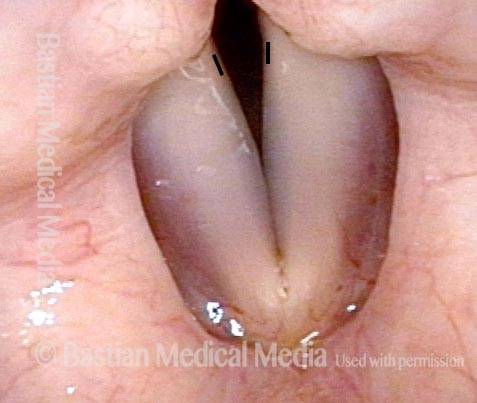
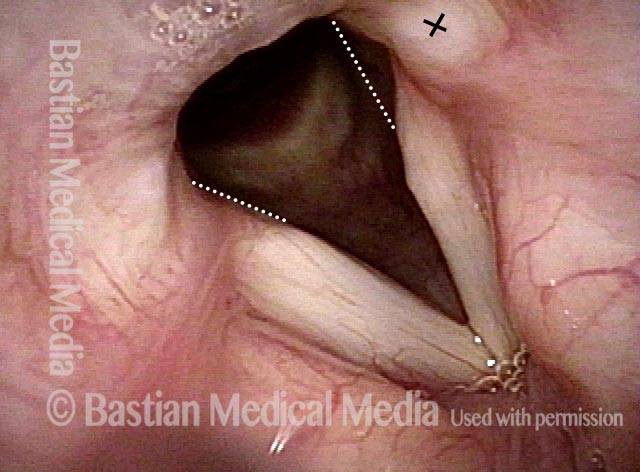
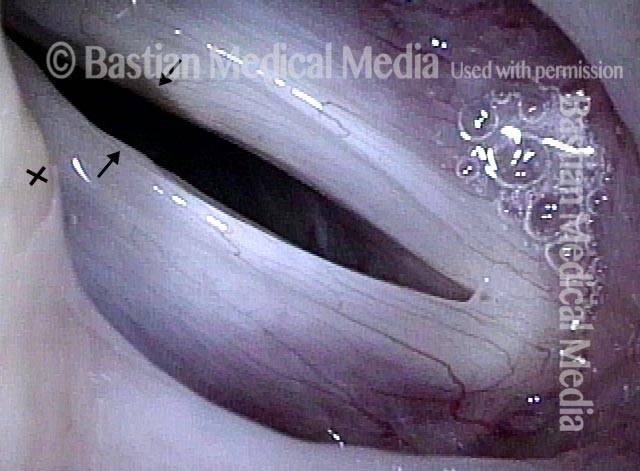
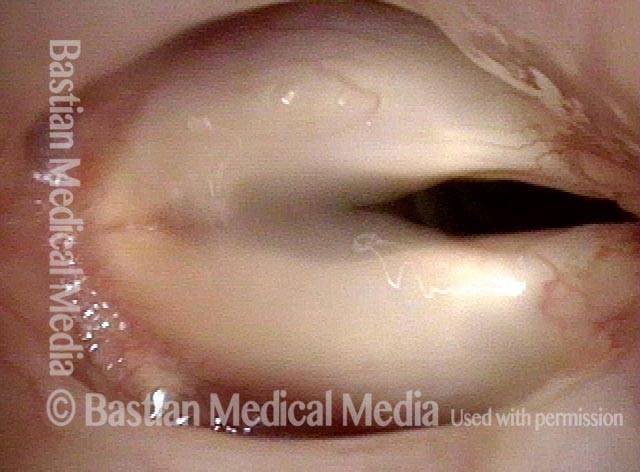
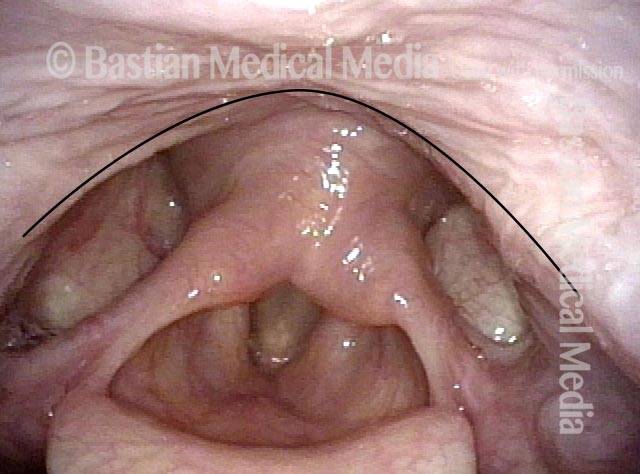
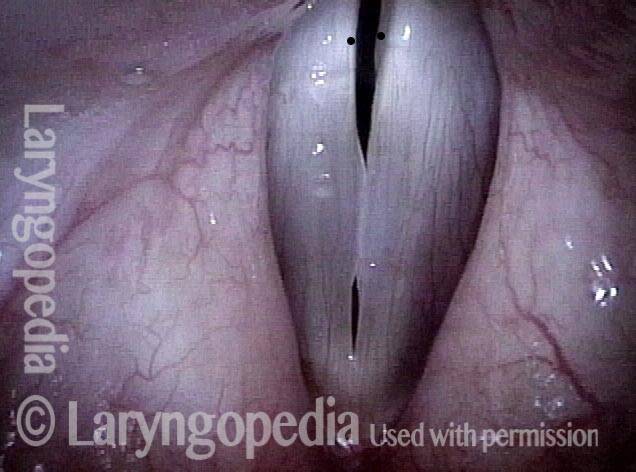
Rest Position of Pharynx (1 of 6)
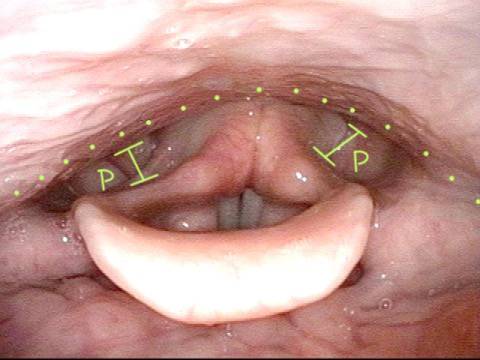
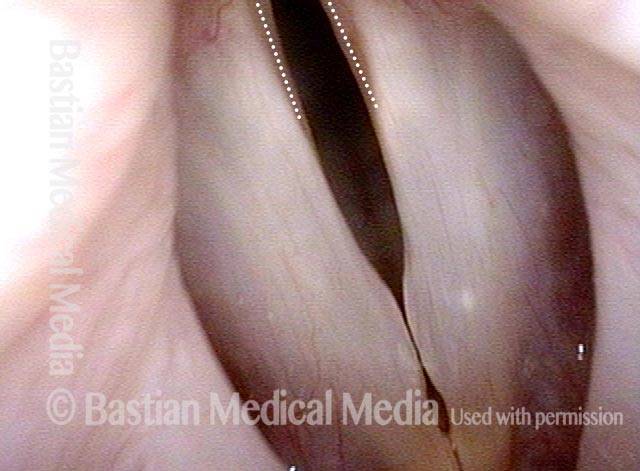
This talented teenaged classical singer is bothered by a sense of effort, fatigue, and discomfort when attempting her high soprano notes. Quiet breathing (seen here) establishes the rest position of pharynx (dotted lines), with wide open pyriform sinuses (P). A thin sheet of muscle is just beneath the mucosa.
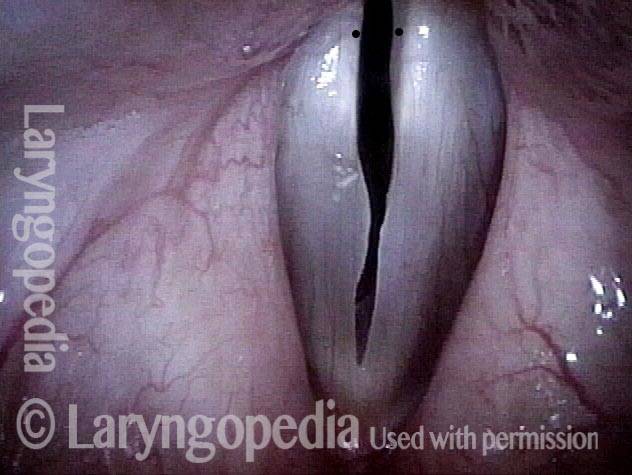
Inactive Pharynx Musculature (2 of 6)
Pharynx muscle should be inactive (not contracted) until a singer reaches the top few notes of his or her range. This singer is producing voice at B3 (247 Hz), a low note for this singer. The pharynx musculature remains inactive, like in photo 1.
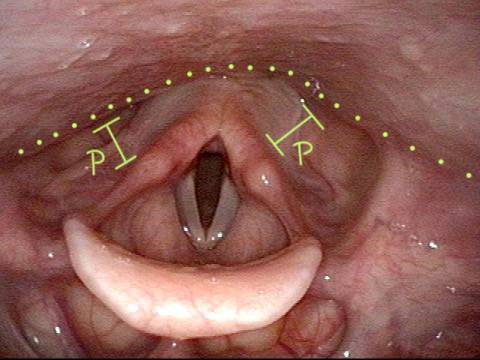
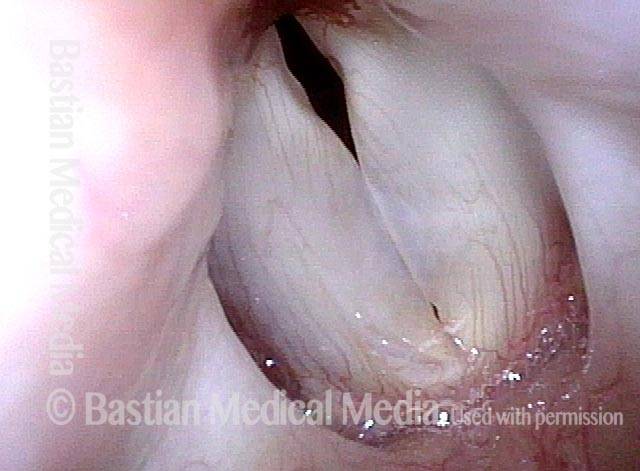
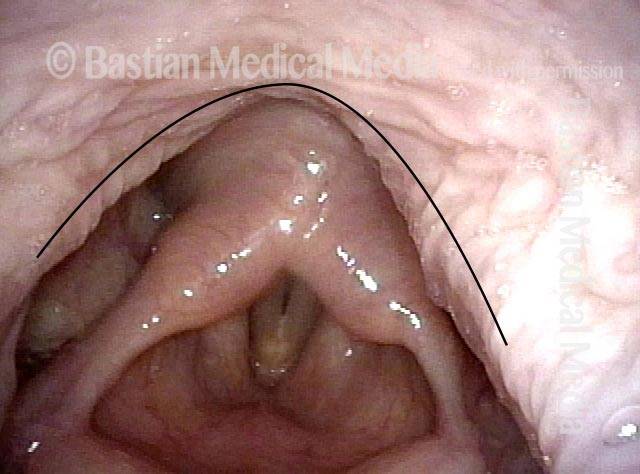
Contracted Pharynx (3 of 6)
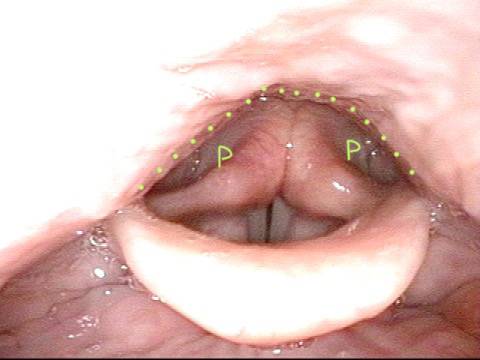
At B4 (495 Hz), which is only middle voice, the pharynx begins to contract, inappropriately. Note the smaller diameter of pyriform sinuses (see lines), and the more curved pharyngeal wall contour (dotted lines).
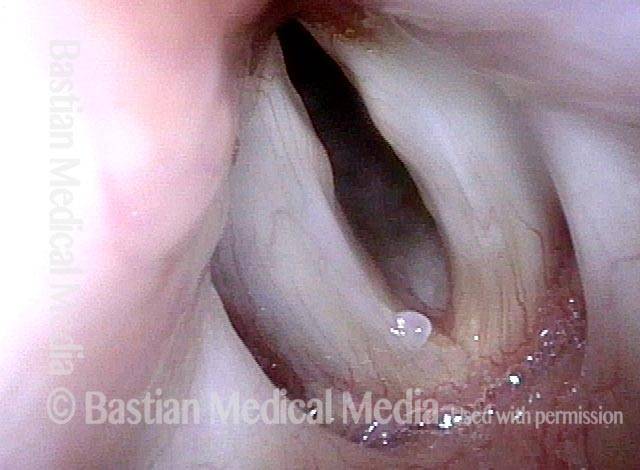
Contracted Pharynx (4 of 6)
At E-flat 5, still far from upper range, the pharynx is contracting a lot, and again inappropriately. This degree of contraction should not be seen until much higher in her range. If she sings continually at this pitch and higher, she will experience paralaryngeal discomfort and effort, and sometimes a “reaching up” vocal quality.
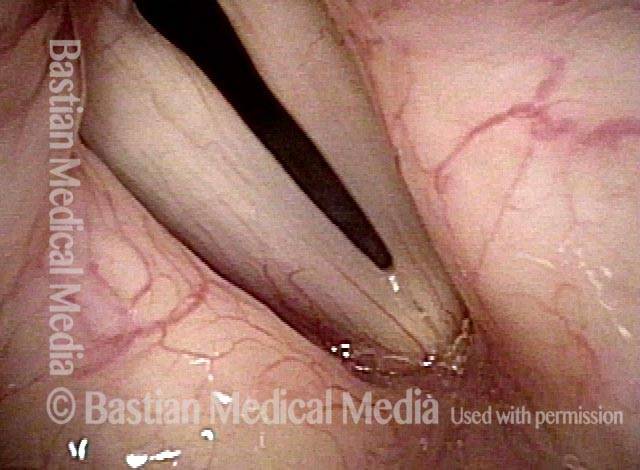
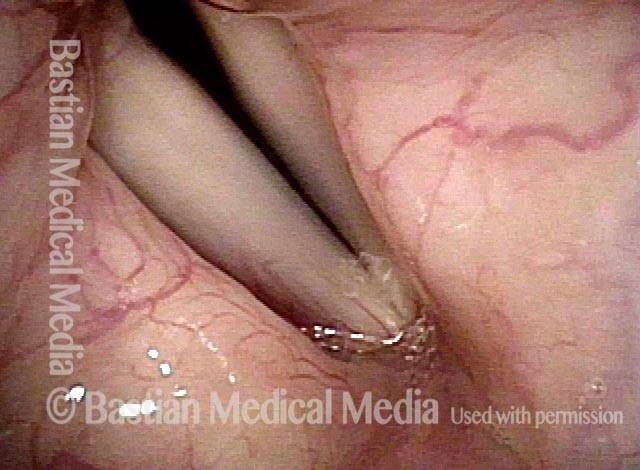
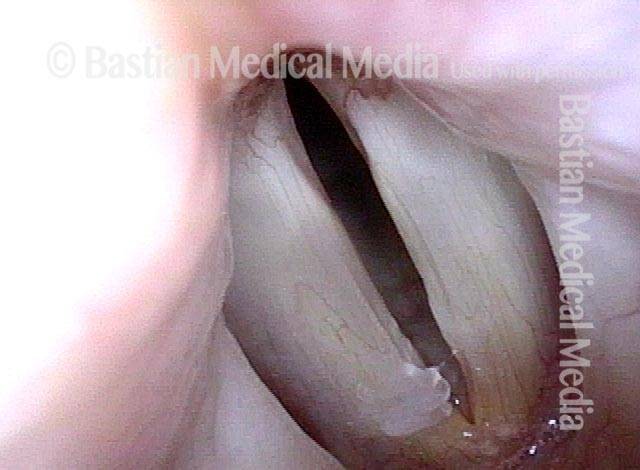
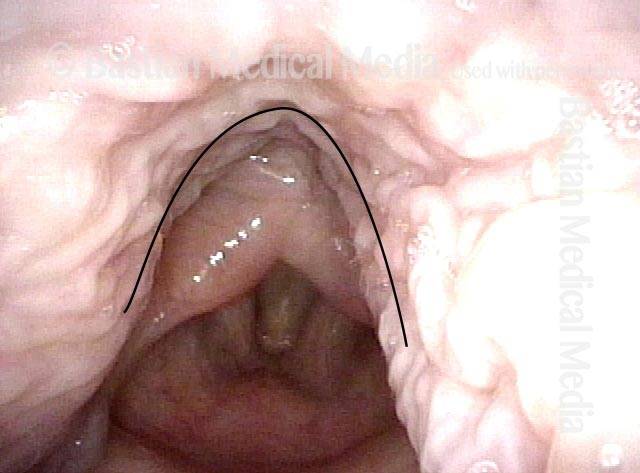
Greater Contraction of Pharynx (5 of 6)
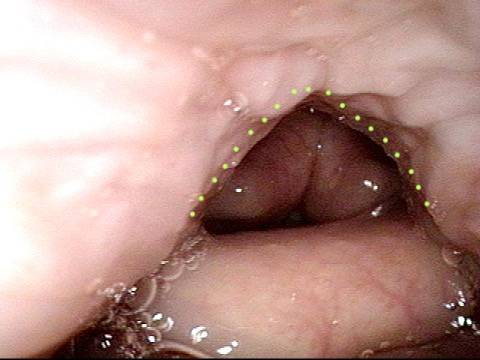
Now at “only” F#5 (740 Hz), the contraction of the pharynx is maximal and pyriform sinuses closed. For a soprano, this degree of contraction is ideally not seen before reaching C6 (1046 Hz) or higher! As the pharynx is not designed for sustained contraction, upper voice singing will be impossibly uncomfortable for her.
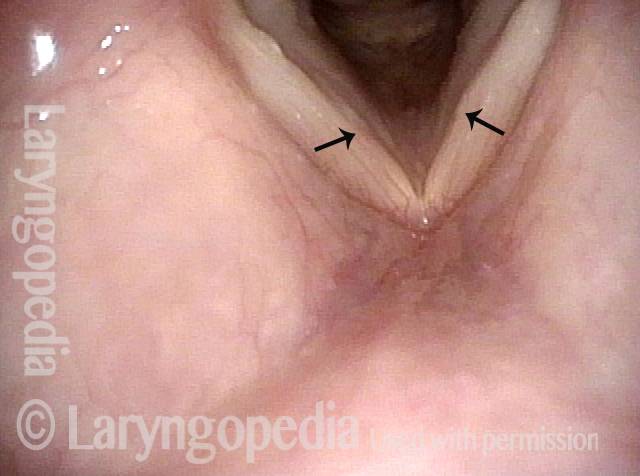
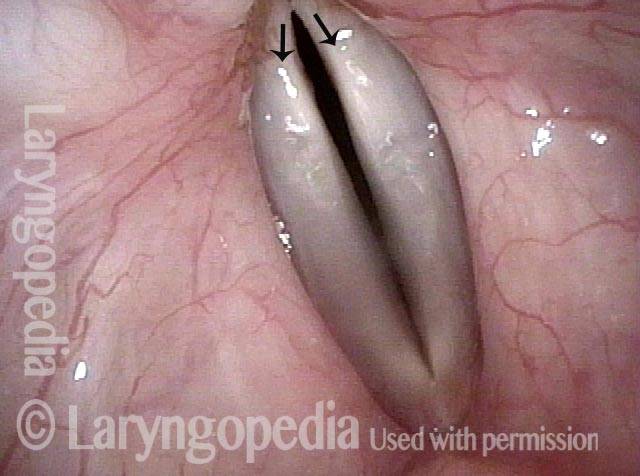
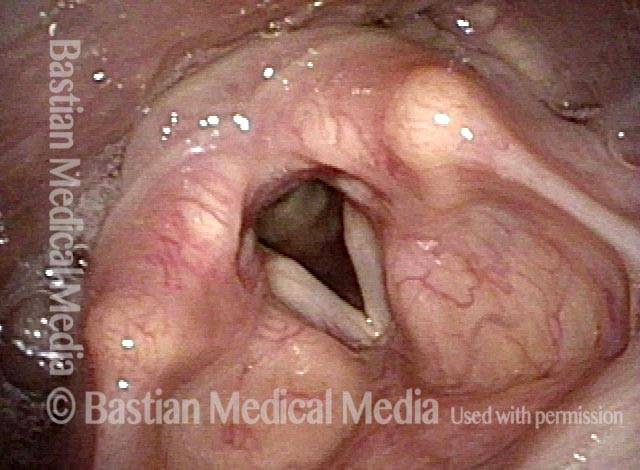
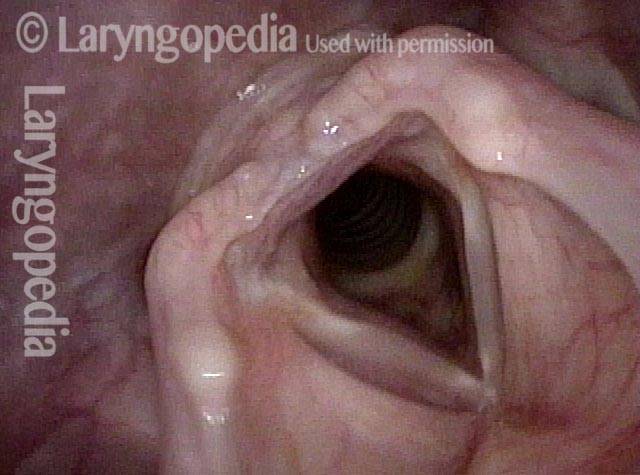
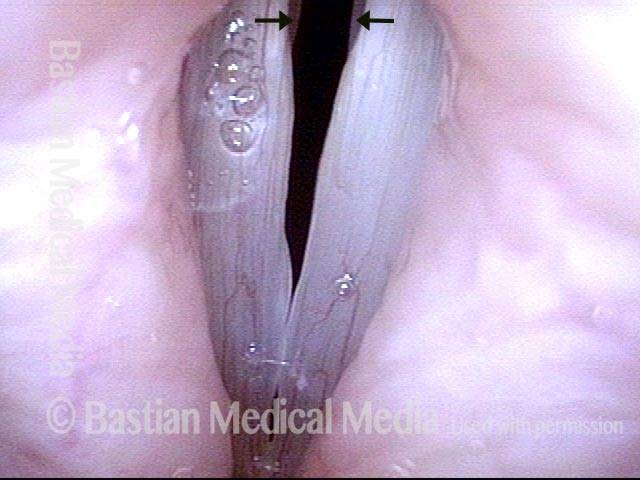
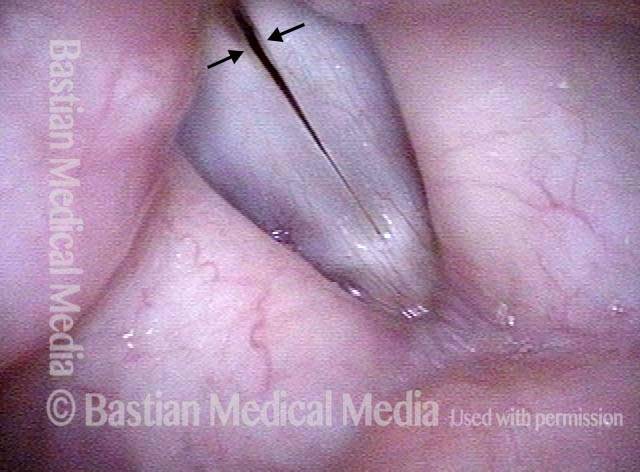
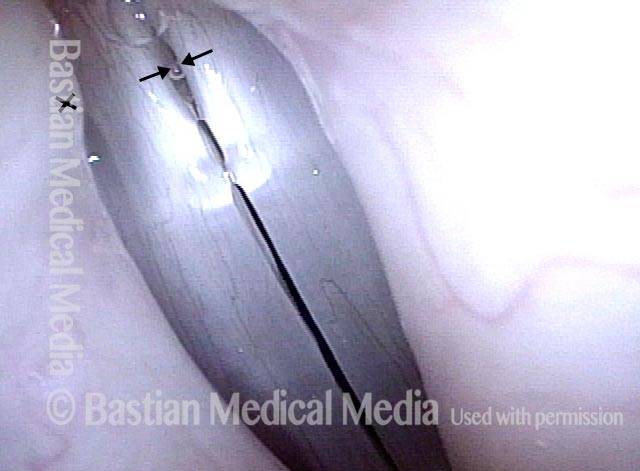
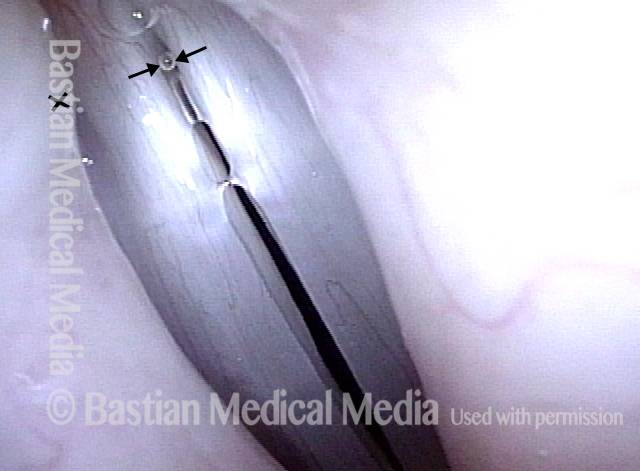
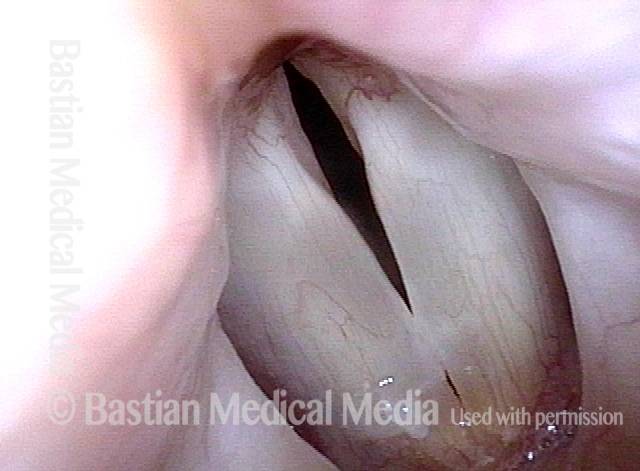
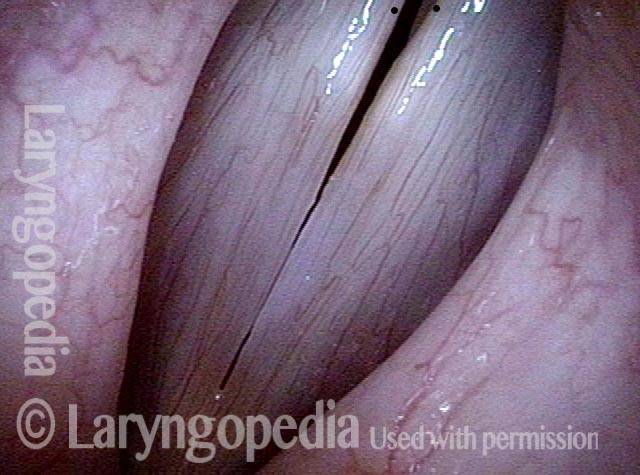
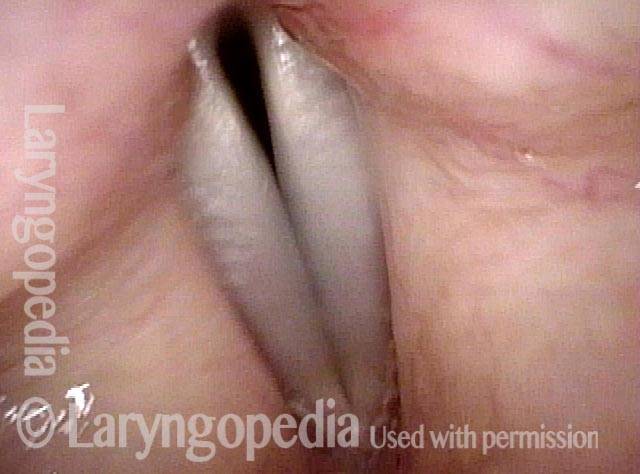
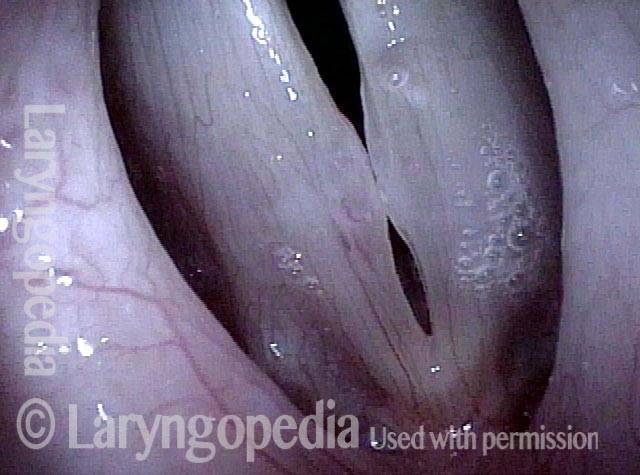
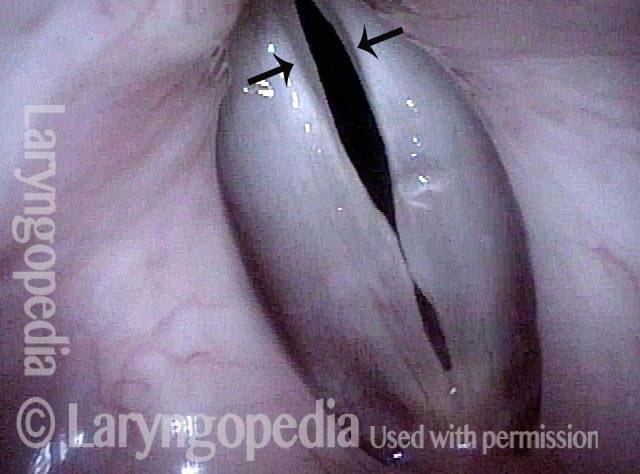
Phonating Larynx (6 of 6)
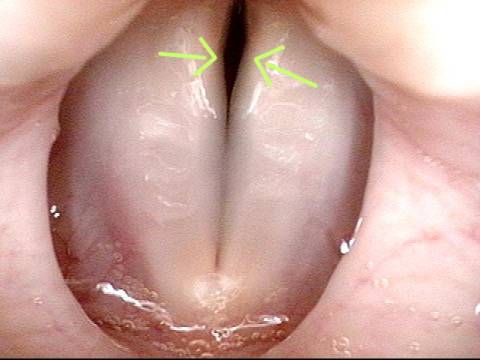
Close-range visualization of the phonating larynx (note the vibratory blur) shows a characteristic posterior commissure gap (arrows). This finding is also characteristic of MTD.
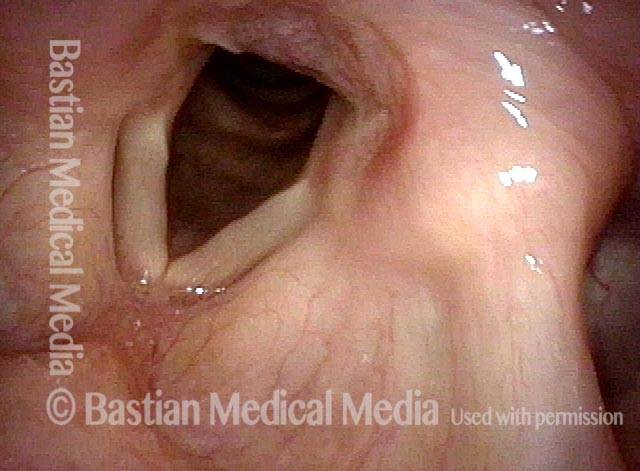
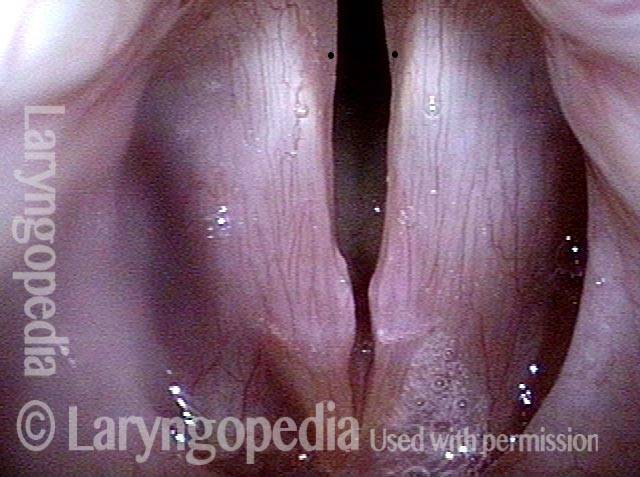
Use Different Views for MTD Than for Frequently-Associated Nodules
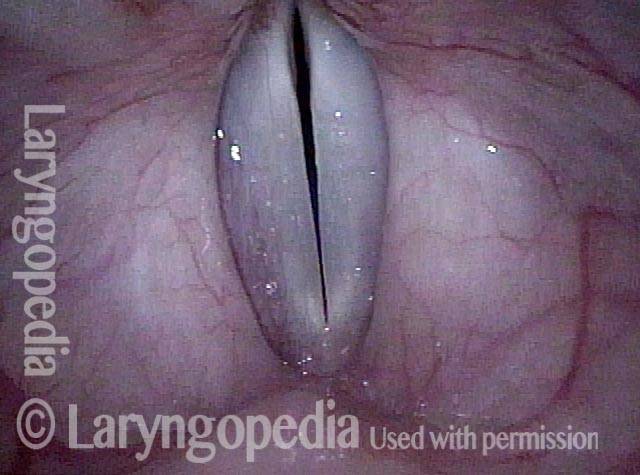
Convex vs. straight (1 of 4)
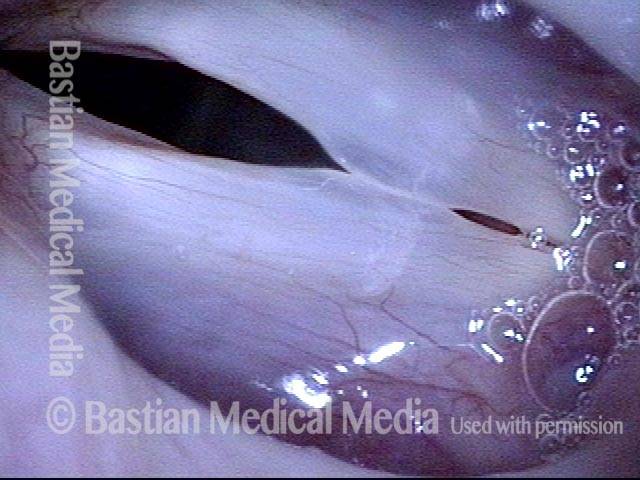
Only one of the two reasons this person has for vocal symptoms can be seen in this abducted (breathing position) photo: the margins of the vocal colds are convex rather than straight due to vibratory injury.

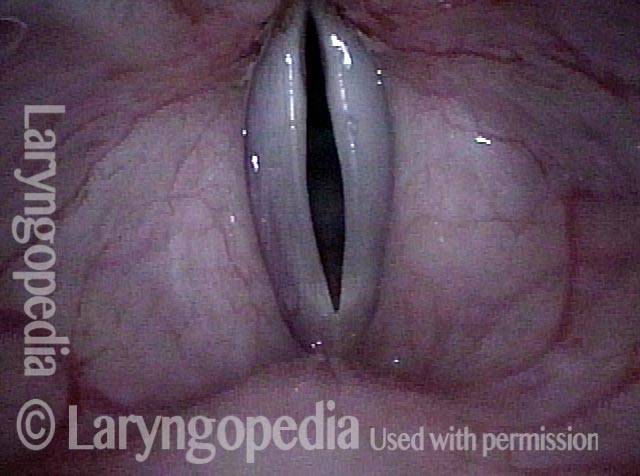
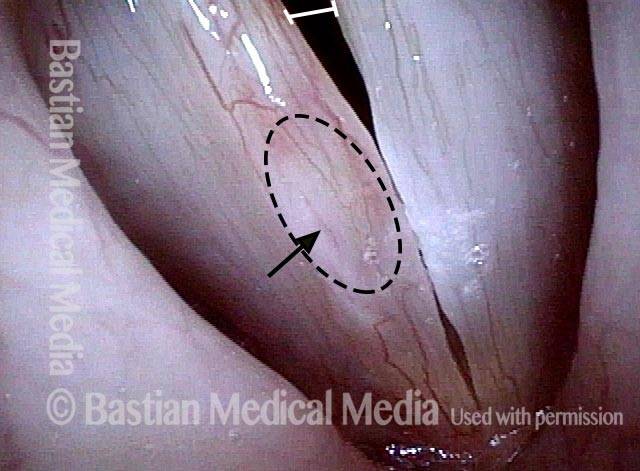
Swellings + MTD (2 of 4)
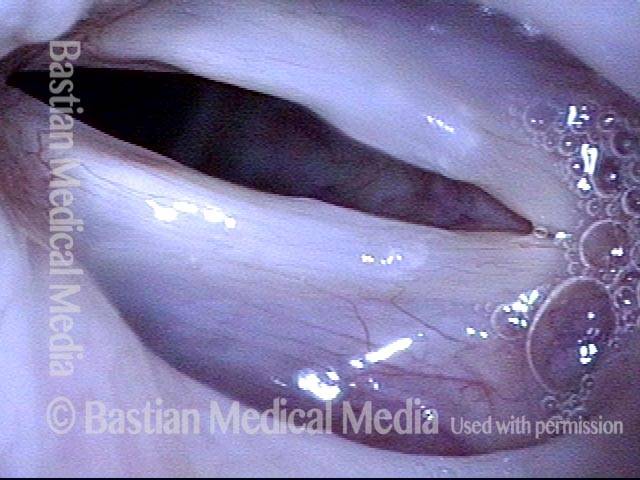
The adducted (voicing) position continues to show the margin swellings in the lower 1/3 of the photo, but adds the diagnosis of MTD, with separated “grey” vocal processes (dotted lines) within the posterior third of the vocal cords. 1 marks the center of view; 2 the midpoint of the nodules.

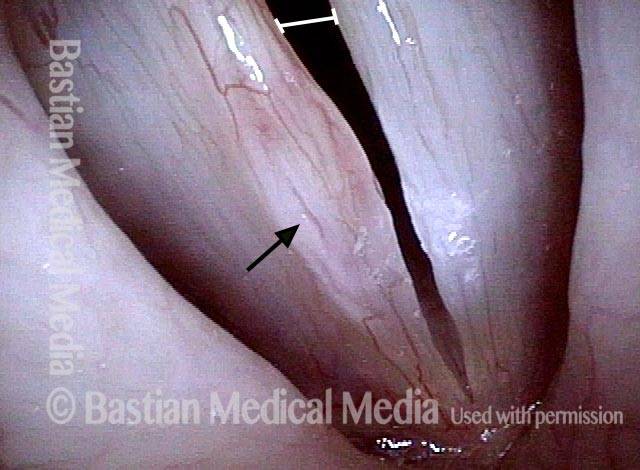
Strobe lighting (3 of 4)
A slightly magnified view under strobe light. Note the MTD again (persistently separated vocal processes), and the swellings.

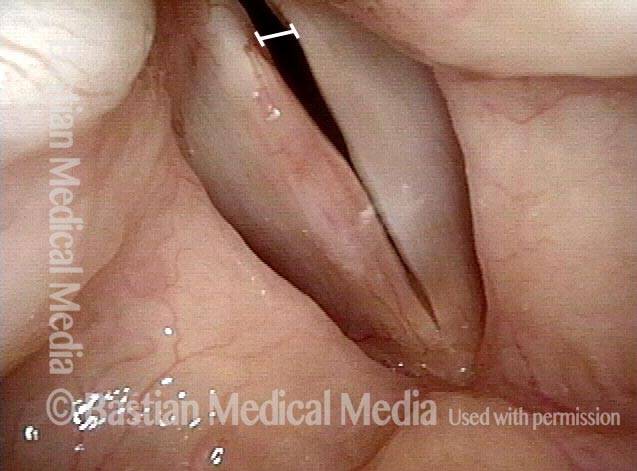
Use different views (4 of 4)
Now the view is a little more magnified, and centered on the nodules, at 2. The nodules are much better seen, but the crucial information for diagnosing MTD (vocal process posture) is lost in this view. This series illustrates that often both views are needed, as views like photo 2 and 3 are not ideal for the nodules.

MTD Posturing Abnormality Transiently Corrected With Creaky Voice
Breathing position (1 of 6)
Young soprano with short phrase length, paralaryngeal discomfort, and effortfulness in singing high range—all symptoms seen with MTD. In this distant view, no abnormalities are seen during breathing.
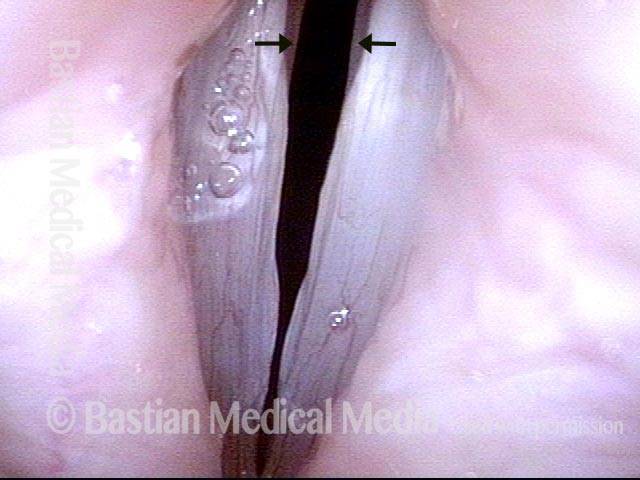
MTD posturing (2 of 6)
Under standard light, the MTD vocal cord posturing is seen at B-flat 4 (466Hz). Note the slight lateral turning of the vocal processes (arrows) and wide dark space/ blur between the cords.
“Closed” phase (3 of 6)
G4 (392 Hz) under strobe light. Even at this middle voice pitch, closed phase is not truly closed, especially at the vocal processes.
Open phase (4 of 6)
At the same pitch, this open phase view also helps to explain breathiness and short phrase length.
Creaky voice, closed phase (5 of 6)
The patient is asked to produce the voice with creaky quality just to prove that the vocal processes are physically able to adduct. Compare this closed phase view with photo 3.

Creaky voice, open phase (6 of 6)
Open phase, still in creaky voice at G4. Compare with photo 4. Creaky voice is one temporary diagnostic antidote to MTD, not a complete “treatment.”

Muscular Tension Dysphonia
Example 2
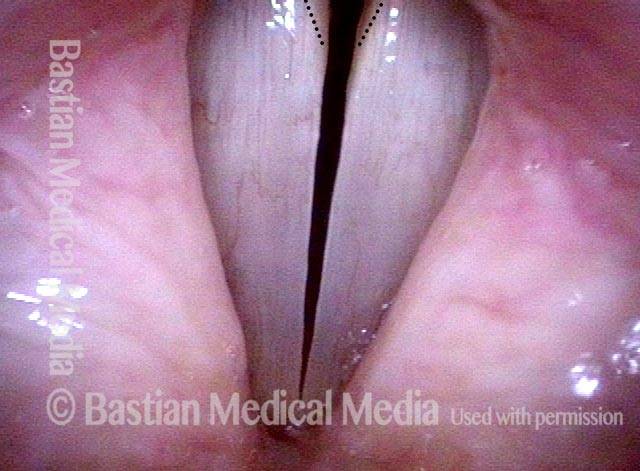
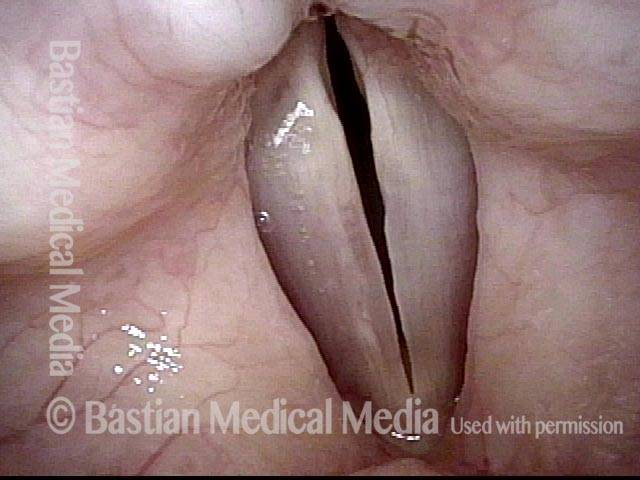
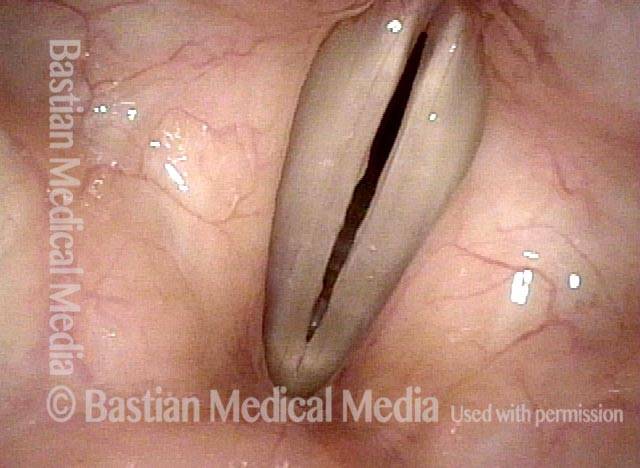
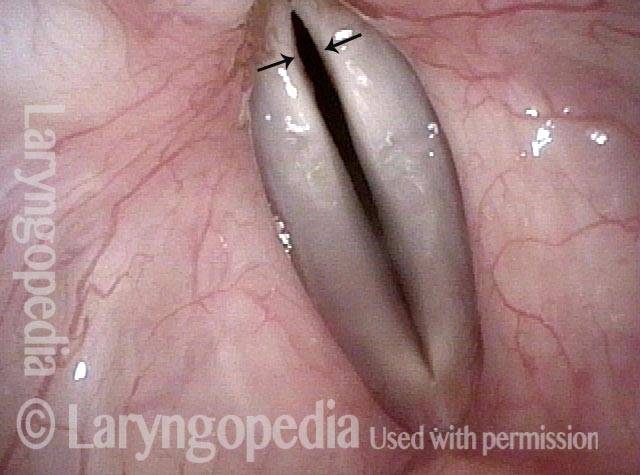
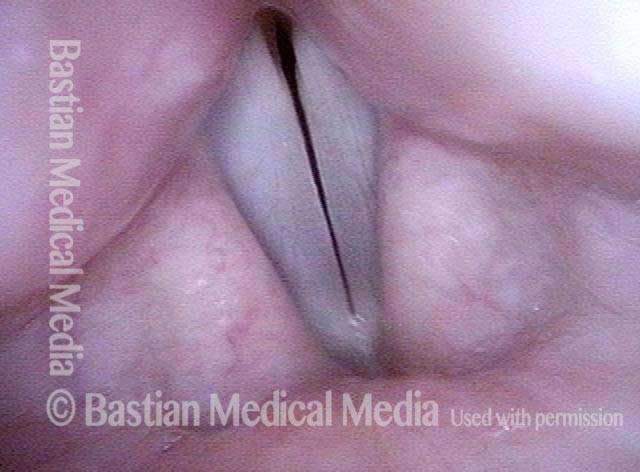
Muscular tension dysphonia (1 of 3)
This extensive voice user experiences upper voice limitations, extreme breathiness (air-wasting during phonation), and neck discomfort. When making voice, the cords are significantly separated posteriorly such that the major part of air is wasted. The white dotted lines should be fully together, with only a thin dark line between the cords.
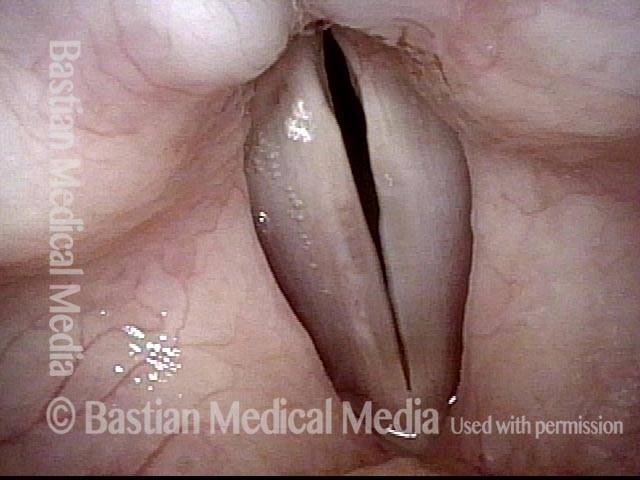
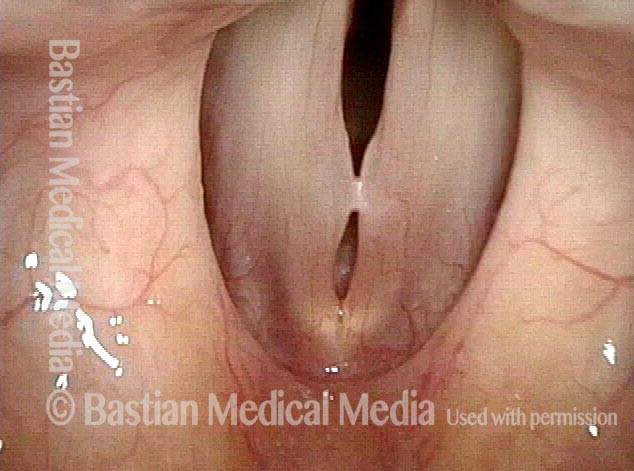
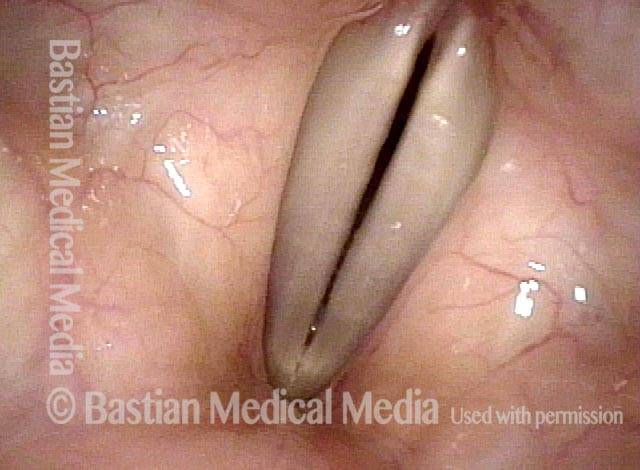
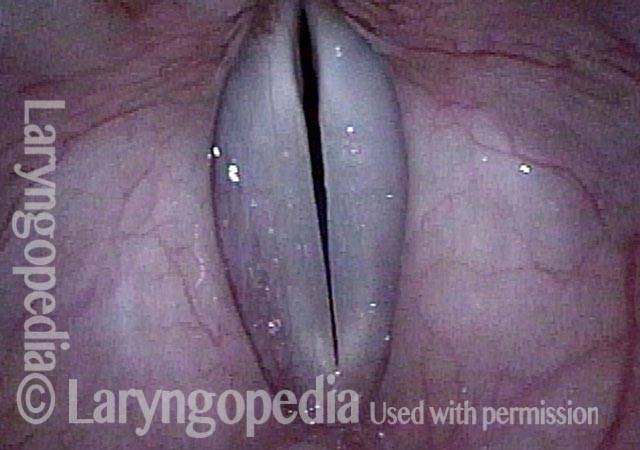
Muscular tension dysphonia (2 of 3)
Strobe light, closed phase of vibration at B-flat 3 (approximately 233 Hz). The translucent, polypoid nodules come into early contact, but equally if not more importantly, the posterior vocal cords remain significantly separated as a vocal cord positioning inefficiency.
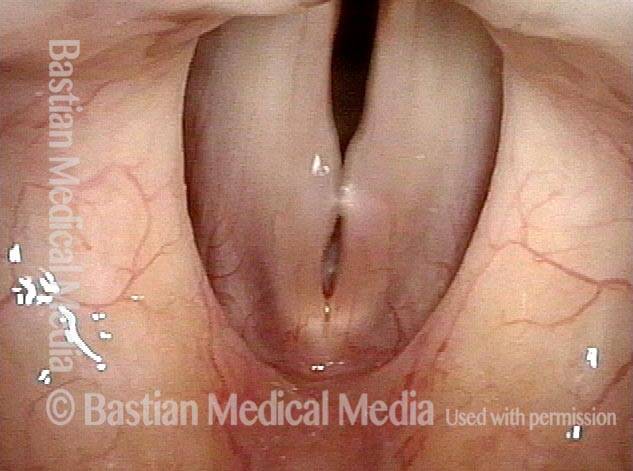
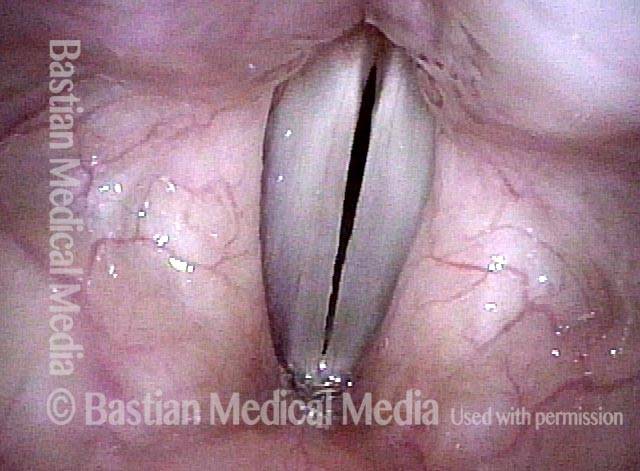
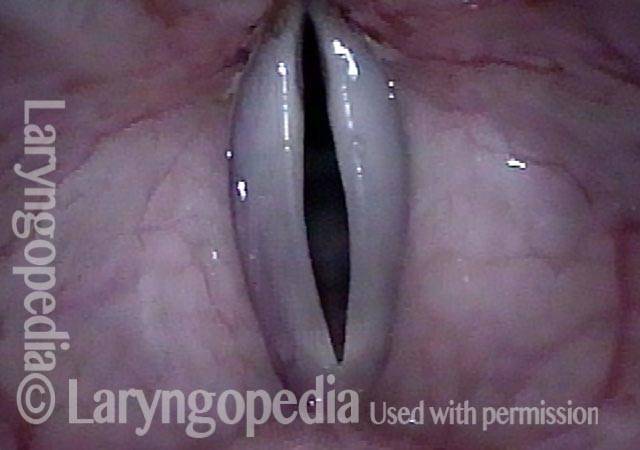
Muscular tension dysphonia (3 of 3)
Open phase of vibration at the same pitch.
To See MTD, You Must See Posterior Commissure and Vocal Process Mucosa Especially at High Pitch
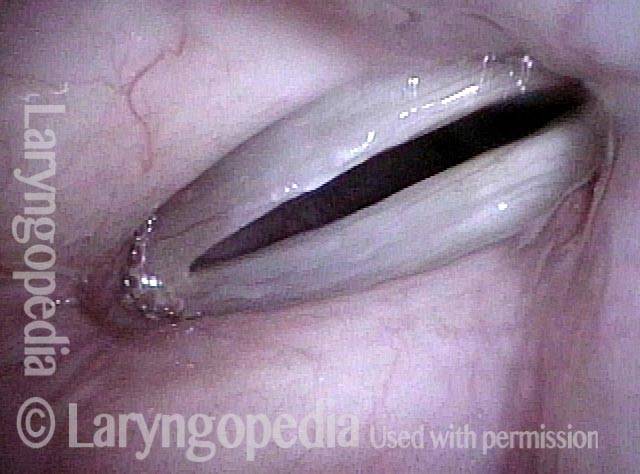
Breathy voice (1 of 4)
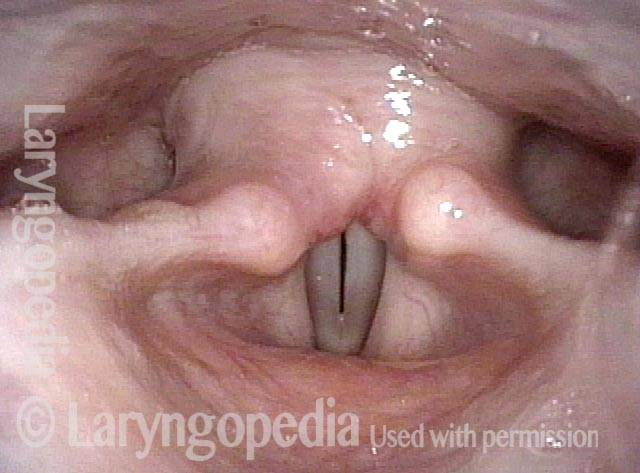
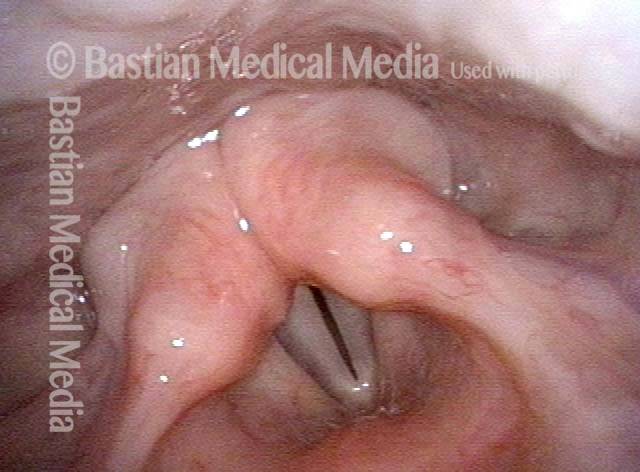
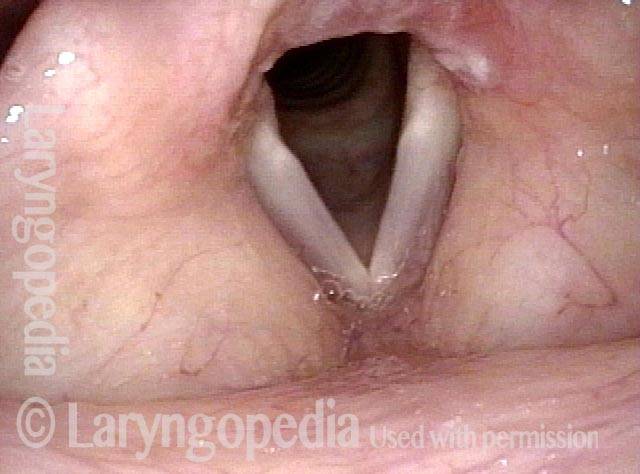
Young female singer developed breathy voice quality, a feeling of strain in the anterior neck and some cracking of the voice when using upper singing range. In this view, the explanation is not obvious for 2 reasons: First, the view is distant, and second, the posterior commissure is not seen due to overhang of the arytenoid apices.
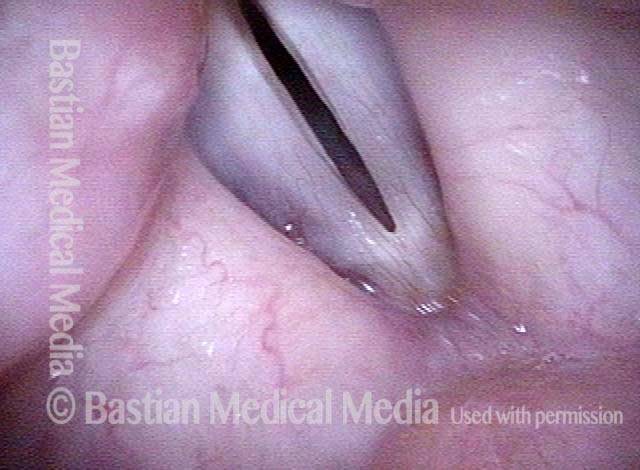
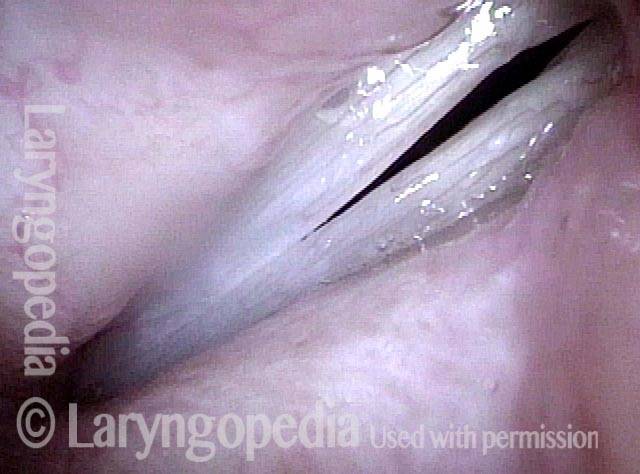
Posterior gap (2 of 4)
Closer range, but at low pitch of B3 (247 Hz). Here, a posterior gap strongly suggests the diagnosis of MTD, but the view is still inadequate because the posterior commissure and specifically vocal process mucosa is still not seen.

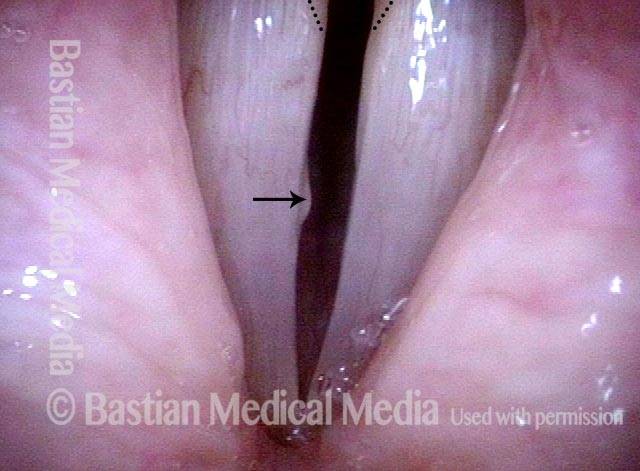
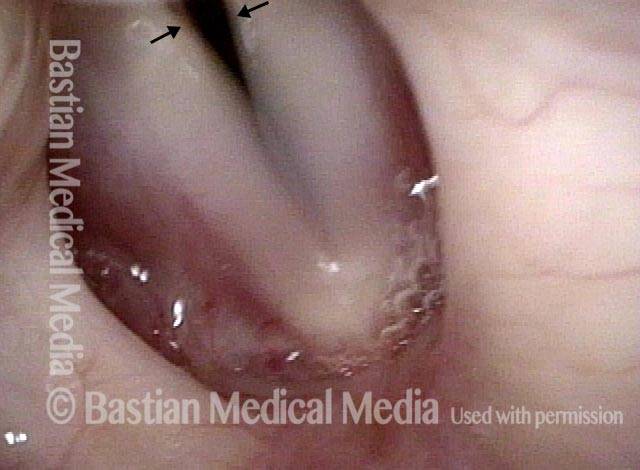
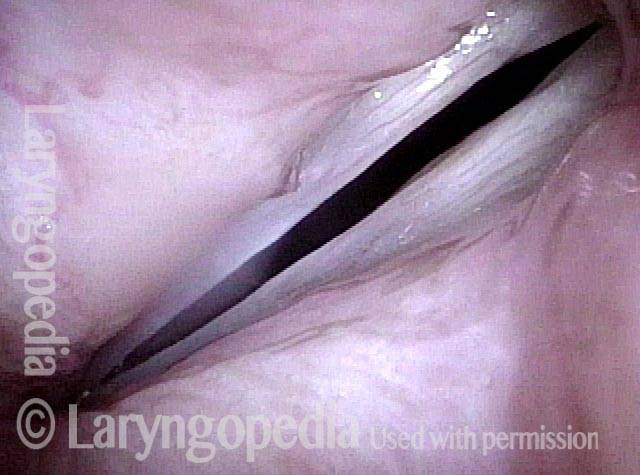
MTD (3 of 4)
At slightly closer range under strobe light, and at much higher pitch of G5 (784 Hz) the explanation for her vocal symptoms is clearly seen. The vocal processes (covered by more “grey” mucosa indicated by tiny arrows) are not together. This is a classic finding of MTD. Even in this closed phase of vibration view, the gap between the cords is large, explaining the breathiness and short phrase lengths.

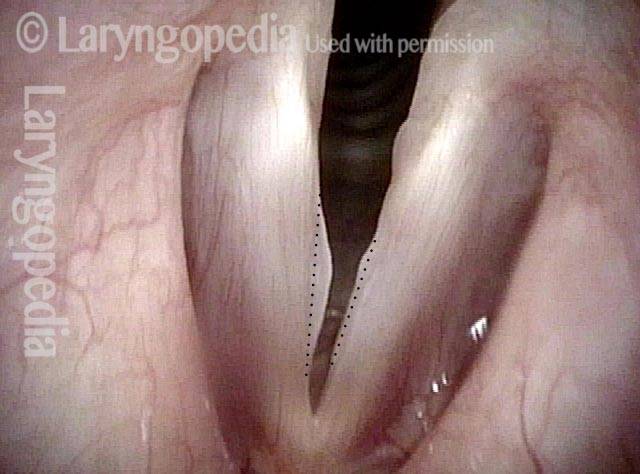
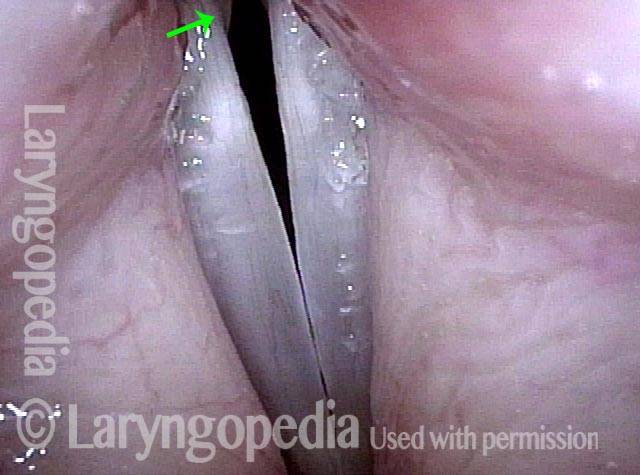
Open phase (4 of 4)
At the same pitch of G5, but now open phase of vibration. The arrows here are overlying the vocal process mucosa and diverge (point slightly laterally). If the vocal cord posture were correct, the arrows would point directly forward in parallel with each other.

Severe MTD With “Red Herring” Mucus Retention Cyst and “Reflux” Findings
Possible reflux, barely visible lesion (1 of 4)
Singer in late teens, already with 11 years of vocal training but breathy quality. In this quiet breathing view, the dotted oval outlines interarytenoid pachyderma ( suggesting reflux). This, and a barely-visible lesion of the right cord (left of photo, indicated by black arrow) draw attention, but are red herrings. Dotted lines are for comparison with following photo.
Closed phase at D4, posterior gap (2 of 4)
Closer view under strobe light at D4 (approx. 294 Hz). This is the maximum closed phase, yet there is still a large gap posteriorly. Notice that the vocal processes (embedded beneath the grey area indicated by dotted lines) are inappropriately separated—the hallmark of MTD.

Closed phase at F#5, posterior gap (3 of 4)
Also under strobe light but at F#5 (approx. 740 Hz). This dramatic and undesirable, dysfunctional gap is seen at the maximum closed phase and is one visual correlate of this singer’s remarkably breathy voice.
Red herring mucus retention cyst (4 of 4)
Again at F#5 under strobe light, but at the maximum open phase of vibration. Now seen is a small mucus retention cyst of the right vocal cord (left of photo) at arrow, entirely a red herring finding. The important finding is the remarkable separation of the vocal processes, as in photos 2 and 3, indicated by dotted lines.
MTD at Prephonatory Instant, and During Phonatory Blurring
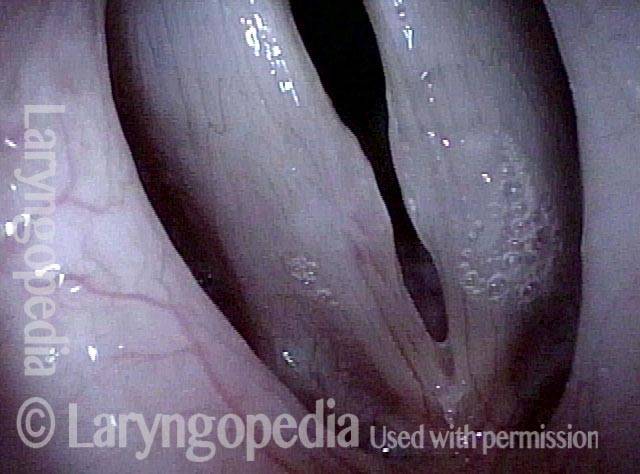
Prephonatory instant (1 of 2)
Nineteen year-old singer with “small, quiet, breathy voice,” whose throat feels strained, tight, and choked when she tries to sing. This view shows the position of the cords one frame (1/30 th of a second) before vibration begins. Note the remarkably wide “stance” of the cords.
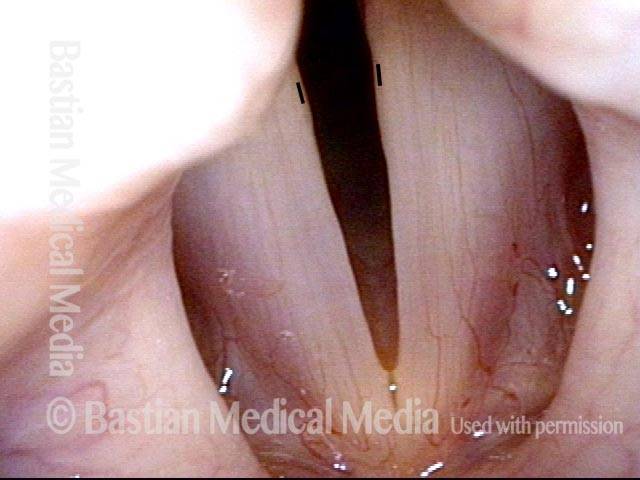
Phonatory blur (2 of 2)
Eleven video frames (1/3 of a second) later, during phonation, the vibratory blur makes the cords appear slightly closer, but the “stance” of the cords is actually the same as in photo 1 above. See short vertical lines for reference between photos.
Looks Like MTD, but Isn’t
Weak, effortful voice (1 of 4)
A middle aged woman describes a weak, effortful voice. Many months earlier, she recovered fully from a grave illness that put her in a coma for several days. She dates the voice change from that event.
Prephonatory instant (2 of 4)
At the prephonatory instant, a split-second before vibration begins, showing that the cords do not adduct fully.
Phonatory blur (3 of 4)
Phonatory blur under standard light. Notice that the vocal cords are separated posteriorly to the same degree as in the prior photo. This can be mistaken for MTD, but is not.
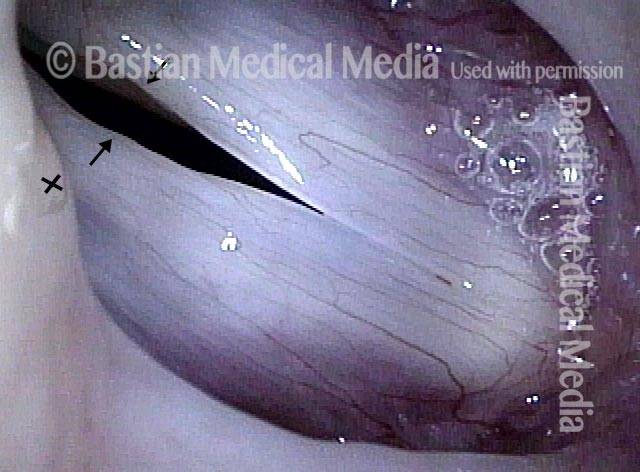
Endotracheal tube injury (4 of 4)
At closer breathing view, one can see an endotracheal tube injury. There is an erosion of the posterior left vocal cord (right of photo), with loss of the expected straight line ( dotted lines). The ‘X’ shows additional area of scarring from the endotracheal tube. The issue here is that the cricoarytenoid joints are damaged; they allow full abduction (separation) of the cords for breathing, as in this photo and photo 1, but do not allow full adduction (approximation) for voicing (seen in photos 2 and 3). Hence, her normal breathing, but weak and air-wasting voice. The therapy approach here would be similar to for MTD, however, and there are some modestly-helpful surgical interventions that can also be considered.
Persistent MTD and Pharynx Recruitment in Young Singer After Sulcus Removal
Squamous mucosa lining the sulcus (1 of 5)
Closed phase at A5 (880 Hz) under strobe light. Arrow points to line of sulcus. The entire white area (within dotted line) is buried squamous mucosa lining the sulcus.
Open phase, distance posteriorly of cords (2 of 5)
Also at A5, but open phase of vibration. Sulcus opening (arrow) is a little more evident. Note most of all that the distance between the cords at their posterior ends is similar (a little greater in this view due to mucosal displacement of the upper surface of the cords).
Closed phase, distance posteriorly of cords (3 of 5)
In a more distant view under standard light at A5 (880 Hz) that shows the posterior vocal cord separation more clearly during phonation (note blurring caused by vibration).
Two weeks post-surgery, MTD (4 of 5)
Two weeks after successful surgery to remove the right sulcus (left cord margin elevation undisturbed pending verification of restored right cord oscillatory ability). The prephonatory instant at A5 (880 Hz), shows that the posterior commissure separation is virtually identical to preoperatively, proving that the MTD posturing abnormality, and not only the sulcus, is a primary issue for this voice.
Re-posture vocal mechanism (5 of 5)
Still under standard light as in photo 4, phonation (and blurring of the margins) has begun and both cords vibrate well. Upper range has been extended by this surgery, but breathiness throughout the range is still evident. The remaining challenges are to re-posture the vocal mechanism, and then consider smoothing the left cord margin (right of photo), depending upon residual limitations caused by it, and patient needs.
MTD and Postoperative “Gap Memory”
Prephonatory instant (1 of 6)
Nodules and severe MTD. This is prephonatory instant, standard light at low pitch (C4, or approximately 262 Hz).
Phonatory blur (2 of 6)
A moment later, with phonatory blur, also under standard light.
Post-op, persistant gap (3 of 6)
Eight days after removal of the nodules. Prephonatory instant at a much higher pitch (E5, or approximately 659 Hz). Notice the persistent gap. Slight irregularities will model away with time.
Large gap (4 of 6)
A moment later, with phonatory blur. The large gap remains evident.
Strobe light (5 of 6)
E5 but now under strobe light at “closed” phase which is of course not at all closed due to the MTD.
Strobe light, open phase (6 of 6)
Open phase. This person has an excellent surgical result but will need considerable work to bring the cords into full approximation.
MTD Briefly Abolished with Creaky Voice
Breathing position (1 of 6)
This choral teacher/ singer is troubled by breathiness and short phrase length. Here during quiet breathing, the vocal cords do not appear to be injured.
MTD posturing (2 of 6)
This photo is characteristic of her entire range: Classic MTD posturing abnormality with poor posterior closure.
Gap (3 of 6)
Strobe light, closed phase of vibration at G4 (392 Hz) shows persistent posterior commissure gap.
Open phase (4 of 6)
Open phase of vibration also at G4.
Creaky voice (5 of 6)
The patient has been requested to produce creaky voice, again at G4. In closer view of closed phase, she successfully closes the posterior commissure, though voice quality is not ideal. Compare with photo 3.

Open phase (6 of 6)
Open phase of vibration, still at G4 with creaky voice. Compare with photo 4.

Mind the GAP!
Bilateral vocal cord swellings (1 of 5)
Young mezzo-soprano with “fuzziness” in her sound. In this abducted, breathing position, one can see bilateral vocal cord swellings, at the arrows.

MTD gap (2 of 5)
Pre-phonatory position for E5 (659 Hz) under standard light. The swellings are more clearly seen, but the MTD gap is enormous and greater than would be needed to accommodate the swellings.

Phonatory blur (3 of 5)
Phonatory blur as she sings E5. Large gap remains.

Vocal processes (4 of 5)
Under strobe light, closed phase of vibration at A-flat 5 (831 Hz). The arrows indicate vocal processes widely separated. The points of these two arrows should instead touch.
Surgery? (5 of 5)
Still at A-flat 5, open phase, with wide separation of the posterior cords. Surgery would improve this voice a lot, but other than the occasional ‘self-correcting’ individual, would not fix this large MTD gap.
Indicator Lesions and MTD
Breathy voice (1 of 6)
Distant view at the prephonatory instant in young female singer. There is a wide gap between the cords. The explanation for this gap is not immediately evident, but the voice is breathy.
Phonation (2 of 6)
Phonation has started with margin blurring, and the sense of extra space between the cords remains.

Open phase (3 of 6)
Strobe light, open phase of vibration at B4 (494 Hz)
Closed phase (4 of 6)
Closed phase of vibration, still at B4. Note the incomplete closure posteriorly caused by MTD. Arrows indicate the vocal processes.
Open phase, indicator lesions (5 of 6)
Open phase of vibration, strobe light, at F#5 (740 Hz). Here, the subtle indicator lesions are seen more clearly; vocal cord margins are not perfectly straight.

“Closed” phase, MTD (6 of 6)
“Closed” phase of vibration is not really closed and the vocal processes do not come into full closure, again consistent with MTD.
Quasi-Muscular Tension Dysphonia: the Real Thing Is Usually Throughout the Range
Seemingly normal vocal cords (1 of 7)
Normal-appearing vocal cords in young singer plagued by inconsistency of capability, effortfulness, breathy voice quality in middle and lower range.

Good approximation (2 of 7)
At the high pitch of G5 (784 Hz), vocal cords come into fairly good approximation, including posteriorly, at the arrows.

Muscular tension dysphonia (3 of 7)
In low voice C4, during phonation (blur, under standard light), the posterior cords separate (arrows) into the posture of muscular tension dysphonia, with breathy quality. None of the photos so far are adequate, however, to evaluate posterior commissure.
Breathiness (4 of 7)
Under strobe light, at C#4 (277 Hz), closed phase. Note the large separation between the vocal processes, responsible for breathiness.
Open phase (5 of 7)
Still at C#4, but open phase of vibration.
Closed phase (6 of 7)
At the high pitch of F5 (698 Hz), closed phase, note that the vocal processes come into approximation, and there is no breathiness.
Approximated vocal processes (7 of 7)
Again at F5, closed phase isn’t quite closed, but note again that vocal processes remain approximated.
Severe MTD or Bilateral LCA Weakness?
Breathiness (1 of 6)
Older middle-aged woman with a great deal of breathiness creeping into her voice, despite good training and long singing experience. Here, in breathing position, the vocal cords look fairly normal.
Phonation (2 of 6)
At closer range during phonation at G3, note that the vocal processes are both turned slightly laterally. The membranous folds are blurred due to vibration.
Closed phase (3 of 6)
As seen under strobe light during closed phase of vibration at G3 (196 Hz), the lateral turn of the vocal processes is again seen.
Open phase (4 of 6)
Open phase at the same pitch.
Large gap (5 of 6)
At the higher pitch of G4 (392 Hz), note the lengthening of the vocal cords, which often turns vocal processes a little bit more to the midline, but they remain distinctly turned laterally, explaining the large gap.
Open phase (6 of 6)
Open phase at the same pitch. This appears to be bilateral LCA weakness given relative abruptness of onset in a highly trained and experienced singer. Why this happened is unknown.
MTD: Vocal Cord Posture and Pharynx Recruitment Often Come Together
Phonation, A3 (1 of 4)
Middle-aged soprano with loss of upper voice, and tremendous strain attempting to make it. Here producing A3 (below middle C), the pharynx is relatively uncontracted and makes a long broad arch (see line).
Pharynx contracted (2 of 4)
At only middle C (~262 Hz), the pharynx is already surprisingly contracted and is beginning to close the pyriform sinuses and “hug” the larynx.
Maximum contraction (3 of 4)
Truly remarkably, at just A4 (~440 Hz) the pharynx is practically maximally contracted, and the patient experiences paralaryngeal aching trying to make a pitch a full octave below what should be possible for her.
“Closed” phase (4 of 4)
“Closed” phase of vibration at G4 is not closed, in classic “MTD” fashion, and the vocal processes indicated by dotted lines should be completely together but are not.

MTD at A Distance and Up Close
Posterior gap (1 fo 6)
In a somewhat distant view under standard light, the findings of MTD are seen but not clearly. Note that at the prephonatory instant, the gap between the vocal cords becomes gradually wider as it travels posteriorly (to the upper part of the photo).

Phonation (2 of 6)
Now during phonation (note blurring), the vocal cords are still separated posteriorly.

Strobe light, closed phase (3 of 6)
At a more appropriate distance and under strobe light at G4 (~392 Hz), closed phase of vibration. The vocal processes remain separated.

Strobe light, open phase (4 of 6)
Open phase of vibration, at the same pitch, same vocal process separation.
Closed phase (5 of 6)
Closed phase of vibration at D5 (~587 Hz). Note that the vocal cords are longer, and look again at the vocal processes.
Open phase (6 of 6)
At open phase of vibration, also at D5, the MTD remains obvious.
Self-correcting MTD
Swellings (1 of 5)
This is a young soprano opera singer with significant margin swellings bilaterally. The dotted lines indicate what would be the normal margins. The upper voice is very impaired and swelling checks were strongly positive.
Closed phase (2 of 5)
Closed phase of vibration under strobe light at E5 (659 Hz). Early contact of the swellings, and significant gap of MTD posteriorly at the vocal processes (indicated by dots).
Open phase (3 of 5)
Open phase of vibration at the same pitch also shows gap, if anything a little exaggerated.
Post microsurgery (4 of 5)
Six weeks after microsurgical removal of the nodules. Strobe light at G5 (784 Hz). Voice now has “original equipment” capabilities, and swelling checks are normal even to C6 (1047 Hz).
MTD post surgery (5 of 5)
Open phase of vibration still at G5, showing accurate match and bilaterally equal mucosal vibratory excursions. The MTD gap at dots remains, but has partially self-corrected. In some other patients, the gap remains precisely the same after surgery as before, and in that case, necessitates further work with a MTD-qualified voice teacher or speech pathologist.

MTD Phonatory Gap Greater Than Required By Swelling
Open phase (1 of 2)
Open phase of vibration at A4 (440 Hz). Moderate-sized vocal nodules, but the gap between the vocal processes (at dots) seems wider than the combined projection of the nodules.
Closed phase (2 of 2)
Closed phase of vibration shows that the nodules barely touch. It appears that the MTD gap is greater than would be necessary to accommodate the nodules. After surgical removal, this gap sometimes self-corrects; sometimes it does not, as if the “ghosts” of the nodules remain.

Released to Sing, and A Surprise Explanation for Pain
Voice major complains of pain (1 of 4)
A soprano voice performance major worked in a summer resort musical theater troupe. By the end of summer she noted mild vocal decline, with increased breathiness, but also a pain left mid-neck. With a history of successful microlaryngoscopy for removal of nodules 3 years earlier, she was concerned that she might have a significant injury, and shouldn’t sing for the first few weeks of school. Here, she produces voice under standard light at D5 (587 Hz). Large posterior commissure gap suggests MTD, which can cause a sense of “strain” with voice production, but does not require voice rest.
Open phase (2 of 4)
Under strobe light at B5, open phase, the grey vocal process mucosa (at green arrow) is barely within the field of view, but clinches the diagnosis of MTD. Still, no finding here suggests that voice rest required. Technical work on her MTD is indicated instead.

Closed phase (3 of 4)
“Closed” phase of vibration at the same pitch, and now a subtle, very low profile convexity of the left vocal cord (right of photo) serves as an “indicator lesion” but it is so subtle just 3 days after her singing job ended, that again, mild vocal prudence at most is indicated.
Cause of pain (4 of 4)
Saving the real explanation for focal pain to the end: Here we see the cause of her left-sided mid-neck pain: an “arytenoid perichondritis” sort of lesion, unrelated to voice use, and not requiring voice rest. The patient is relieved that she does not have recurrent nodules, and that she can resume voice lessons to battle her MTD.
Search not Only for Nodules, but Also for Segmental Vibration and Look at the Posterior Commissure for MTD
Open phase (1 of 4)
In a young pop-style singer, the open phase of vibration under strobe light at C#5 (554 Hz). This magnified view is best to see the large fusiform nodules.
Closed phase (2 of 4)
Closed phase of vibration at the same pitch shows touch closure—that is, that the nodules barely come into contact.
Segmental vibration (3 of 4)
Even when patients are grossly impaired in the upper voice as is the case here, the clinician always requests an attempt to produce voice above G5 (784 Hz), in order to detect segmental vibration. Here, the pitch suddenly breaks to a tiny, crystal-clear D6 (1175 Hz) Only the anterior segment (arrows) vibrates.

Posterior commissure (4 of 4)
A more panoramic view that intentionally includes the posterior commissure to show that the vocal processes, covered by the more ‘grey’ mucosa (arrows), do not come into contact. This failure to close posteriorly is a primary visual finding of muscular tension dysphonia posturing abnormality.
Muscular, not Mucosal Ceiling Diagnosable Even with Distant Views
Low voice at a distance, pharynx is relaxed (1 of 3)
This very accomplished but “natural” singer is in late middle age and has lost most of her upper range. She has not been ill nor has there been any episode of increased voice use. Low voice (131 Hz) viewed at a distance gives no significant information.

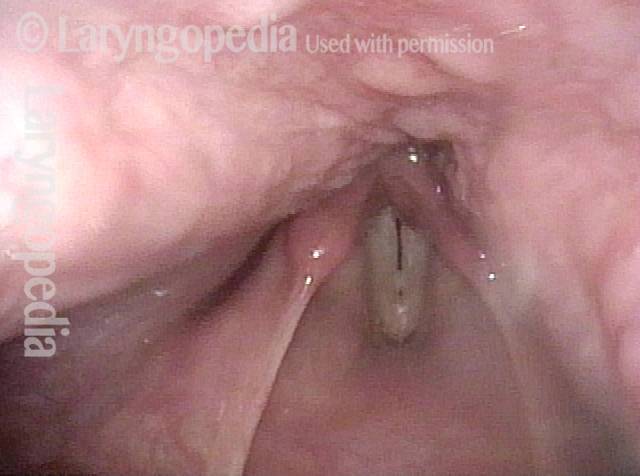
Maximal contraction of pharynx (2 of 3)
Attempted C5 (523 Hz), still distant view. The patient undershoots the pitch and is only able to produce B-flat 4 (466 Hz), and only with effort and muscular strain. Simultaneously, we see maximal contraction of the pharynx, hugging the larynx and obliterating the pyriform sinuses.
Vocal cord swellings are red herrings (3 of 3)
Closer visualization of the vocal cords shows small elevations. They are not the problem; premature pharynx contraction (as seen in photos 1 and 2) reveals that the lowered ceiling of the voice is “muscular” and not “mucosal.”