Saccular cyst is a closed sac originating from a formerly open and functioning laryngeal saccule. An analogy for a saccular cyst is a velvet bag used to hold coins which has its opening cinched shut by a drawstring.
The mouth of the saccule becomes blocked, and mucus secreted within the saccule cannot escape through the normal opening in the anterior ventricle. This closed sac gradually expands, causing the false cord and aryepiglottic cord to bulge; the sac can further expand over the top of the thyroid cartilage and into the neck.
Anterior Saccular Cyst, before and after Removal
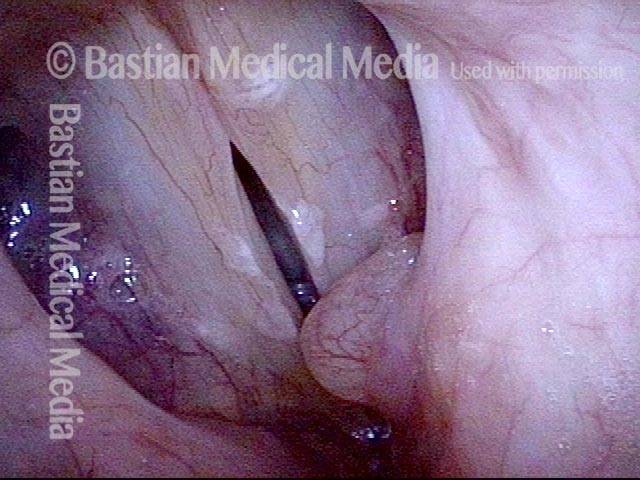
Anterior saccular cyst (1 of 4)
Phonation, open phase of vibration, under strobe light. Left-sided cyst (right of image) causes mildly rough voice quality.
Anterior saccular cyst (2 of 4)
Four years later. Phonation, open phase of vibration, under strobe light. The cyst has enlarged, and voice quality has deteriorated. The patient wants this removed.

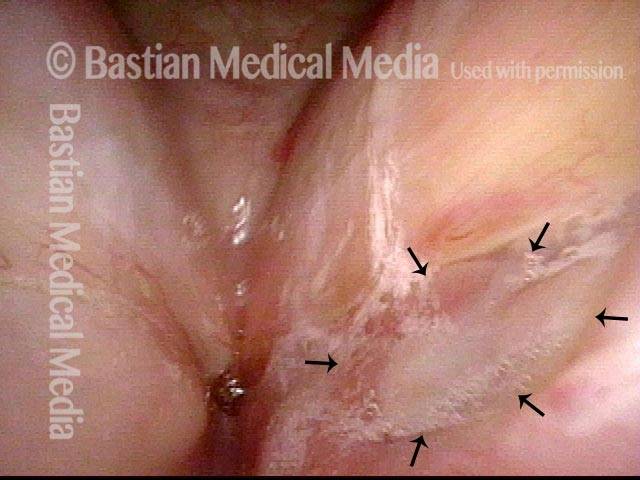
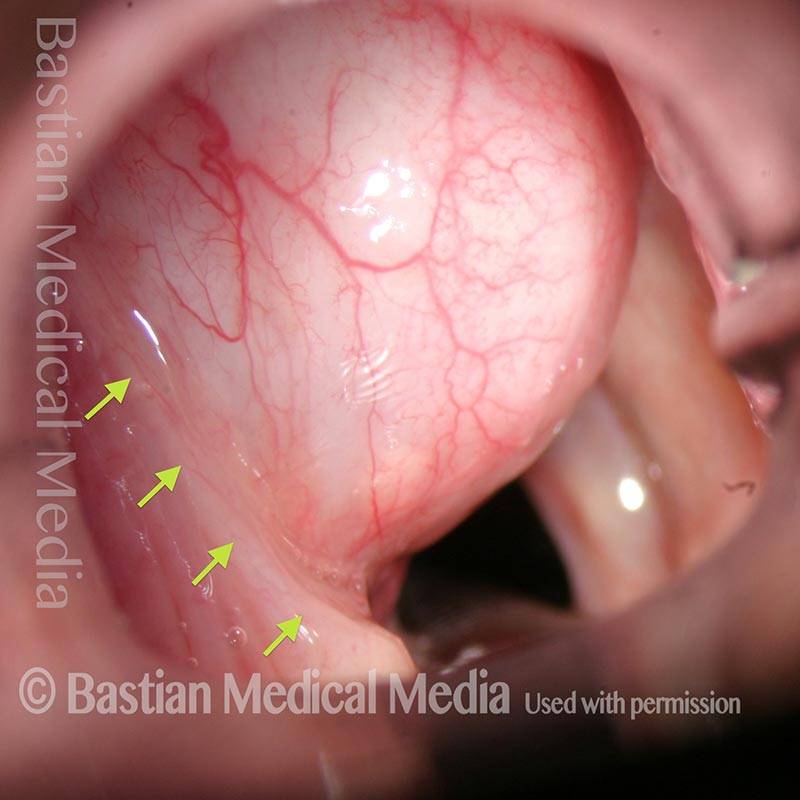
Anterior saccular cyst, removed (3 of 4)
Ten days after laser dissection of the complete cyst (not simple unroofing). At close range, looking into the left ventricle. The raw area (at arrows) is the bed of excision.
Anterior saccular cyst, removed (4 of 4)
Phonation, standard light. Some residual bruising of the left vocal cord (right of image), but voice quality and capabilities are normal.

20 Years after Saccular Cyst Removal!
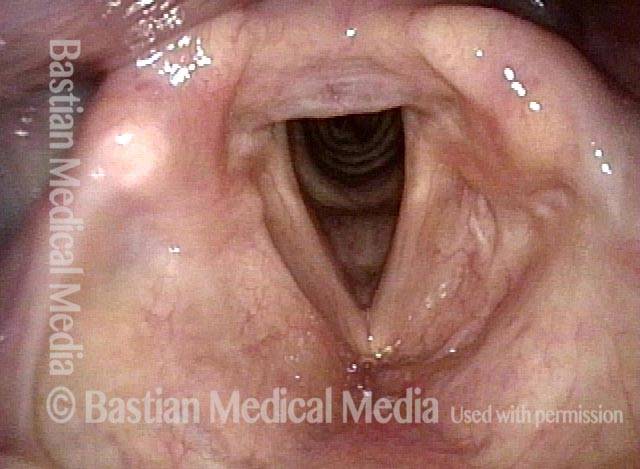
Saccular cyst (1 of 3)
Saccular cyst on the left was removed ~ 20 years ago. In this panoramic view, notice that the left false cord is surgically absent.
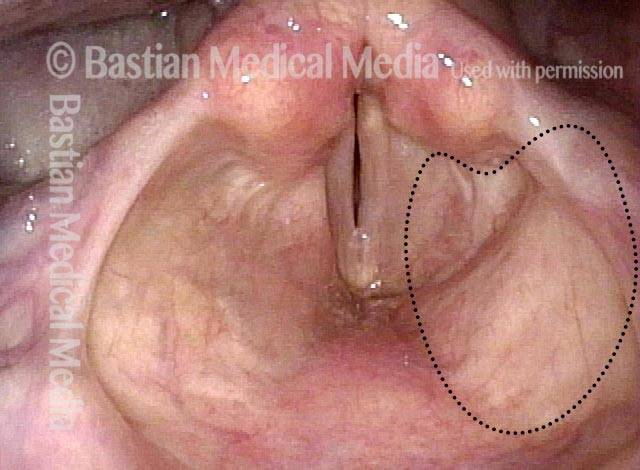
Phonation (2 of 3)
Voice is normal during this view of phonation. Dotted line indicates the outline of the original cyst, as much was delivered from within the aryepiglottic cord.
Respiration (3 of 3)
A closer view during respiration.
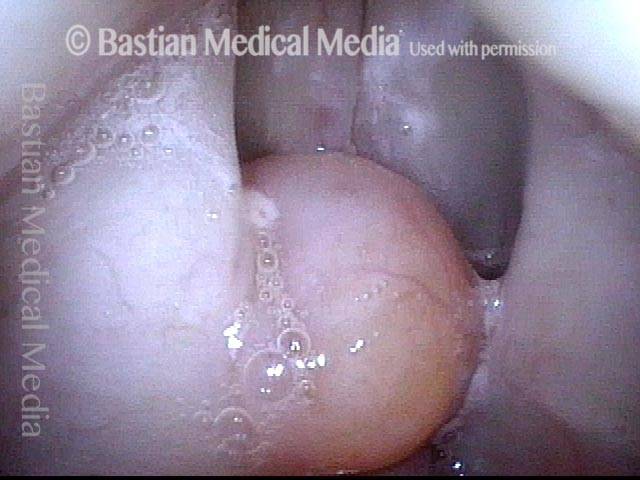
Anterior Saccular Cyst
Anterior saccular cyst (1 of 4)
Breathing position, with a saccular cyst protruding from the right anterior ventricle (left of image). The cyst’s location, color, and superficial vessels indicate that it is neither a polyp nor granuloma.
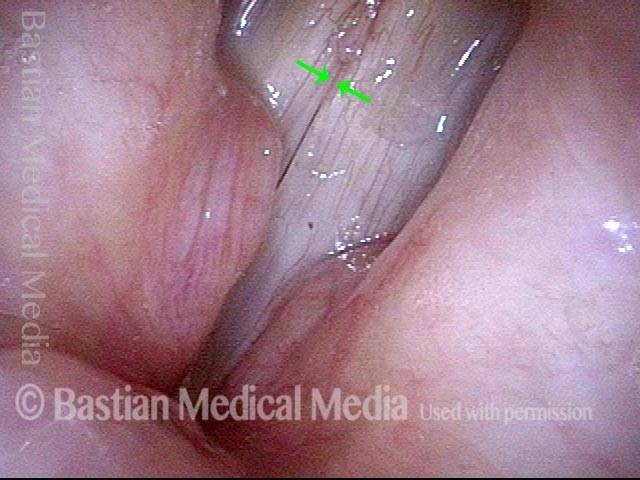
Closer view (2 of 4)
Still closer view (under strobe light), breathing position, showing that the cyst does not arise from the cord, but appears to be depressing the anterior end of the right cord (left of image) slightly. On the left cord is an incidental finding of margin swelling, which is unsurprising in this very talkative individual.
Cyst vibrates when speaking (3 of 4)
Phonation, strobe light, open phase of vibration. The laryngeal vestibule between the false cords is partially blocked. The cyst occasionally participates in vibration, making an extra sound.
Anterior saccular cyst (4 of 4)
Phonation, strobe light, closed phase of vibration.
Bilateral Anterior Saccular Cysts
Bilateral anterior saccular cysts (1 of 6)
Bilateral anterior saccular cysts (faint dotted lines), with vocal cords in open, breathing position. The right cyst (left of image) is larger than the left. These present only into the ventricle, and not significantly upwards into the false cords, nor downwards to press down on the true cords.

Phonation (2 of 6)
Phonation, at a high pitch, so that the laryngeal vestibule (the “airspace” above the vocal cords) is mostly open. Voice sounds normal.

Bilateral anterior saccular cysts (3 of 6)
Phonation at a high pitch again, but under strobe lighting, and at the closed phase of vibration. Note that there is good vibratory closure and that neither cord is pushed down by the cysts; again, the voice sounds normal at this pitch.
Bilateral anterior saccular cysts (4 of 6)
Phonation at a high pitch again, under strobe lighting, but at the open phase of vibration. Note that the cords aren’t impaired from oscillating laterally; again, the voice sounds normal.

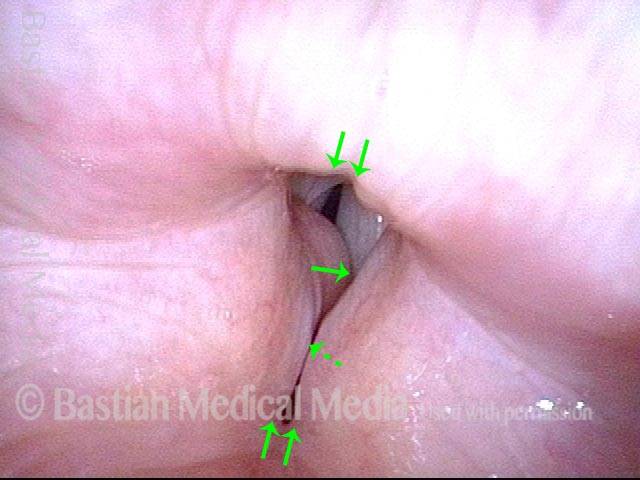
Bilateral anterior saccular cysts (5 of 6)
Phonation at a mid-range pitch. The vocal cords shorten at this pitch, which constricts the laryngeal vestibule (up-down pairs of arrows) and brings the saccular cysts further over the cord (left-right arrows). Voice is still fairly normal.
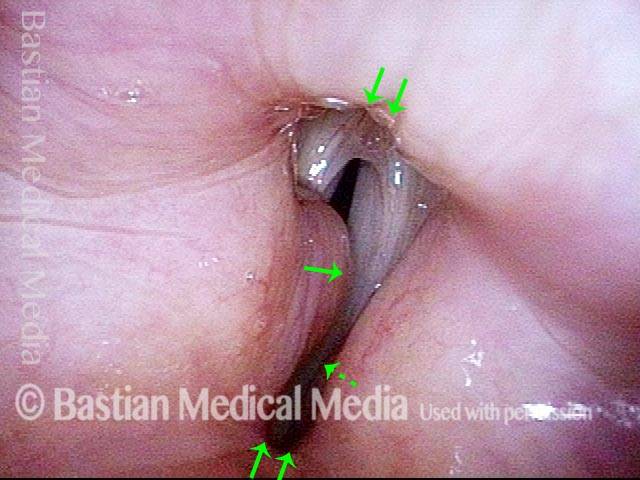
Bilateral anterior saccular cysts (6 of 6)
Phonation at a low pitch. The laryngeal vestibule constricts even further (up-down pairs of arrows), bringing the cysts, especially the larger one, further yet over the cords ( left-right arrows), so that they interfere more with vibration. Voice at this pitch sounds congested or bottled up.
Removal of Lateral Saccular Cyst, Endoscopic Approach
Lateral saccular cyst removal, endoscopic approach (1 of 4)
Note margin of false cord, at line of arrows.
Lateral saccular cyst removal, endoscopic approach (2 of 4)
Removal begins by excising the false cord margin in order to dissect downward to the lining of the saccule.
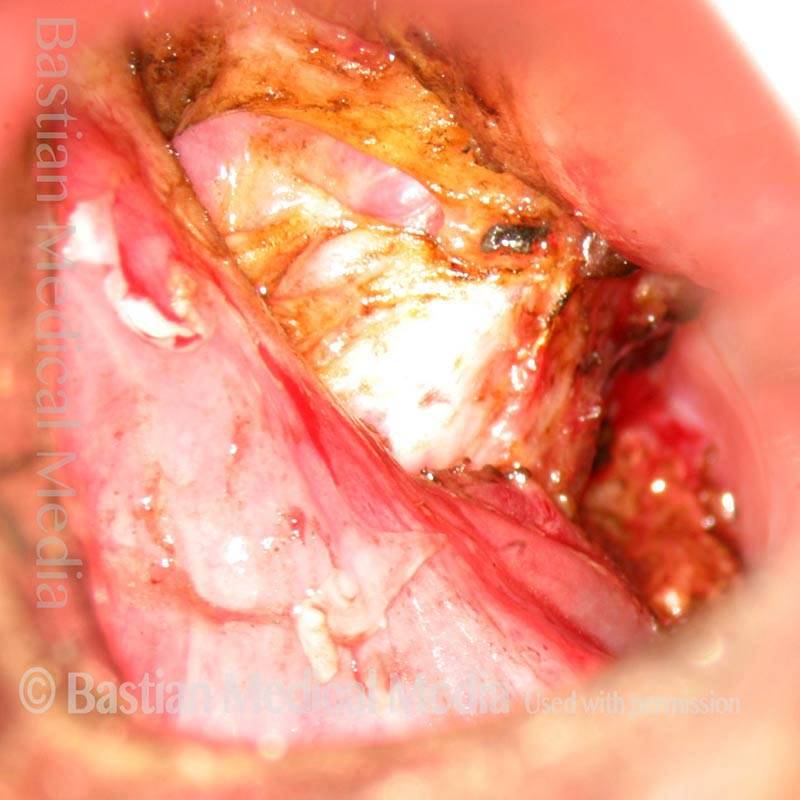
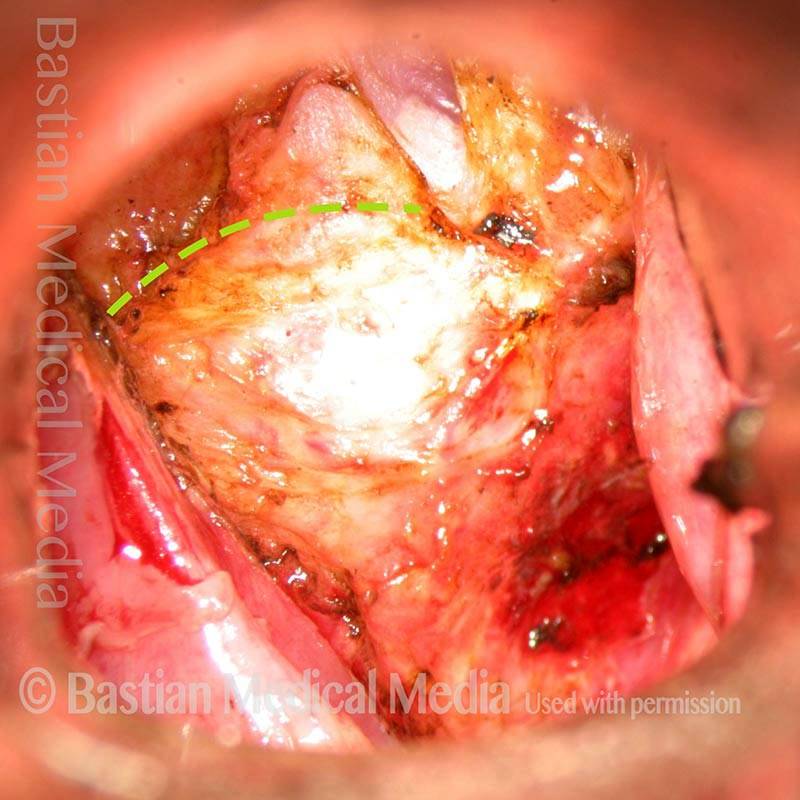
Lateral saccular cyst removal, endoscopic approach (3 of 4)
After removal, see upper border of inner surface of thyroid cartilage, at dotted line (distal end of laryngoscope aimed laterally towards neck contents).
Lateral saccular cyst removal, endoscopic approach (4 of 4)
In-line view of vocal cords at conclusion of surgery.

Removal of Lateral Saccular Cyst, External Approach
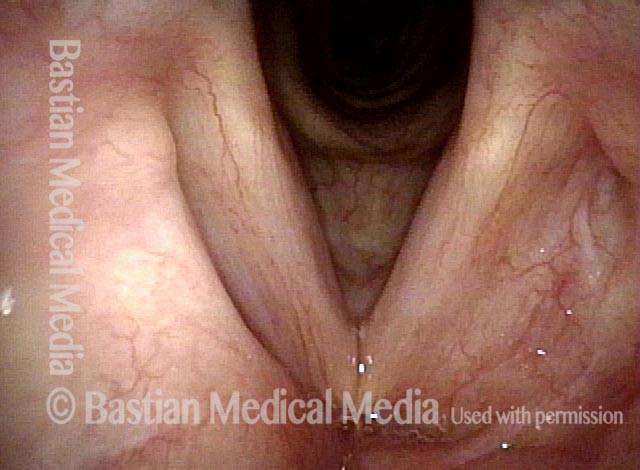
Lateral saccular cyst removal, external approach (1 of 3)
Right of photo is superior, at chin. Note dome of cyst at arrow.
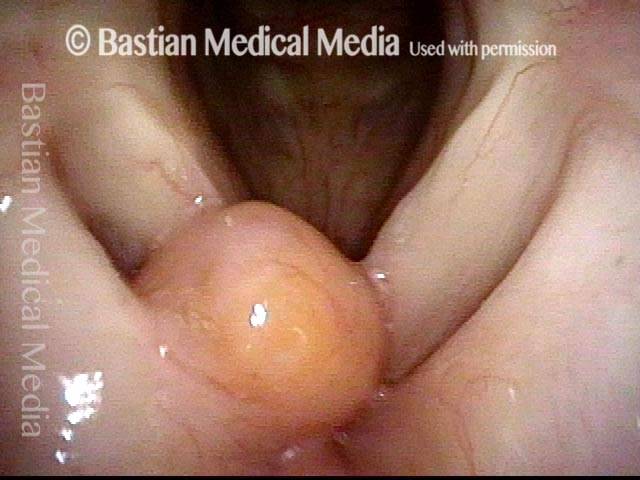
Lateral saccular cyst removal, external approach (2 of 3)
Near completion of dissection, cyst has ruptured and spilled its contents.

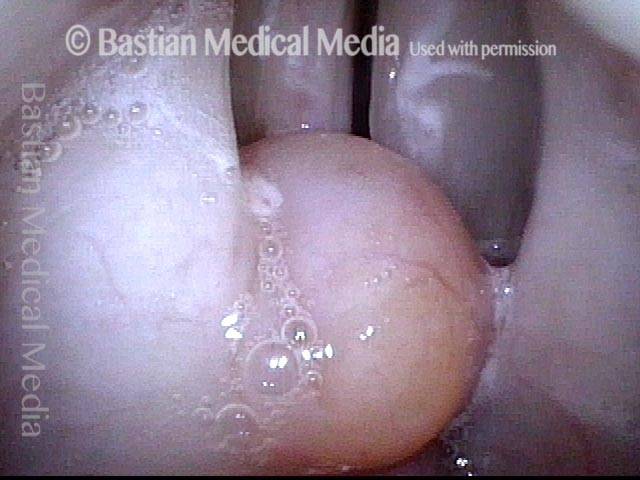
Lateral saccular cyst removal, external approach (3 of 3)
Complete, if collapsed, cyst.

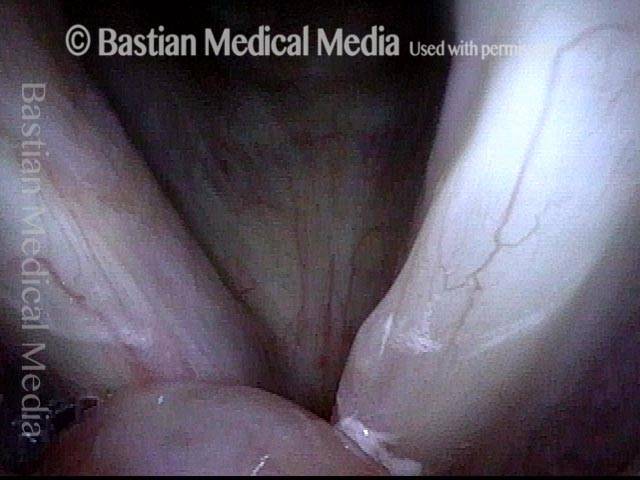
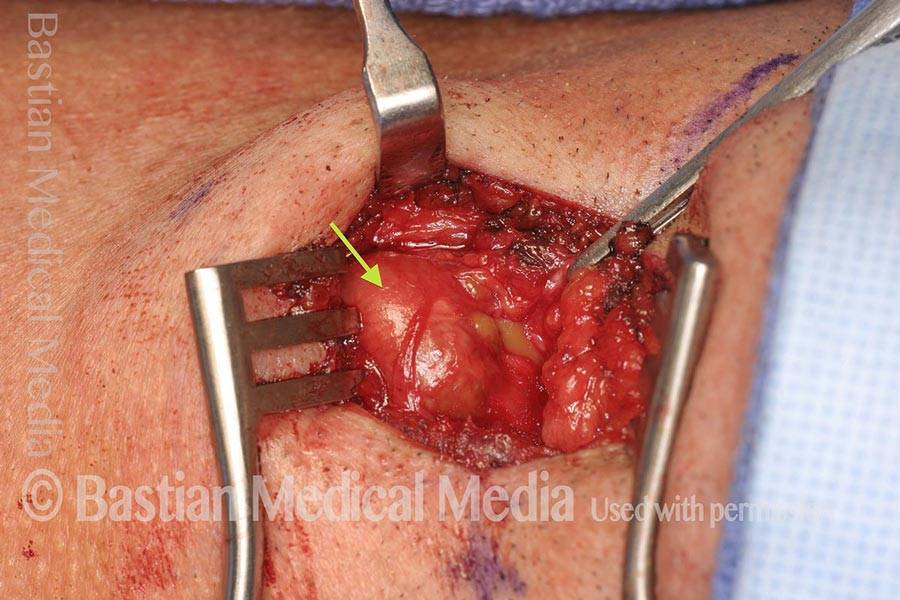
Lateral saccular cyst, external approach
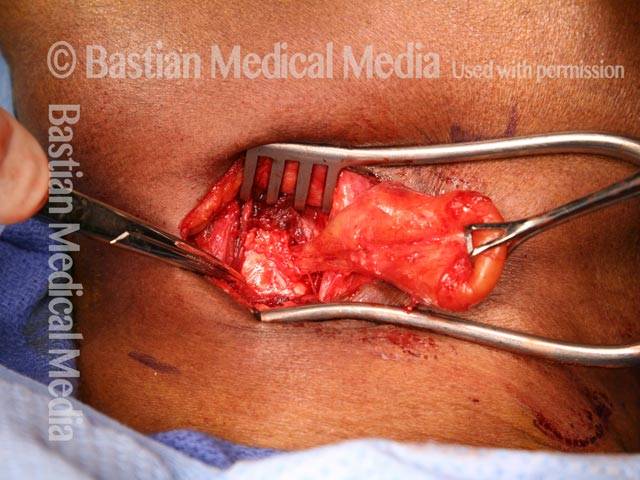
Lateral saccular cyst, external approach (1 of 1)
The hemostat in the lower photo points to the upper part of the thyroid cartilage. The neck of the sack is being followed over the top of the cartilage and between the thyroid cartilage and soft tissue, to its origin at the ventricle.
Saccular Cyst with Extensive Oncocytic Metaplasia
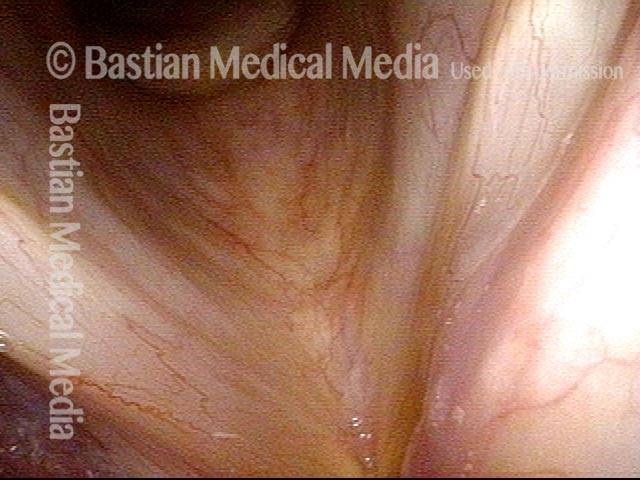
Spherical submucosal mass (1 of 7)
Spherical submucosal mass fills the left supraglottis (right of photo) and bulges into the medial left pyriform sinus, best seen using a “trumpet maneuver”.

Closer view (2 of 7)
Close range endoscopy shows that although the mass obscures the left true vocal cord (right of photo), it is clearly separate.
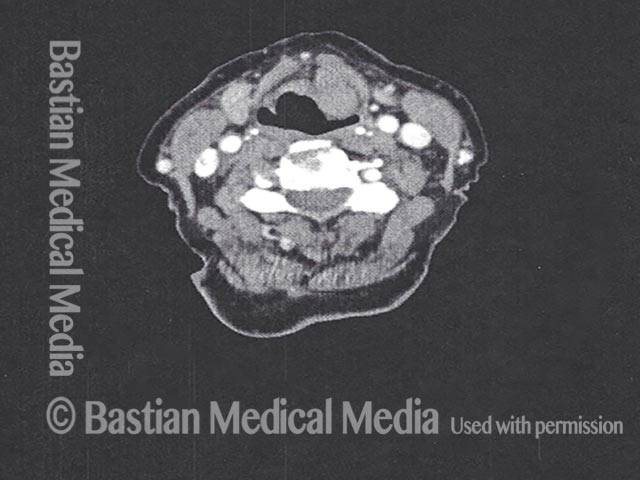
Preoperative CT (3 of 7)
On preoperative CT, the homogeneous, smoothly-marginated mass pushes superiorly into the preepiglottic space.3
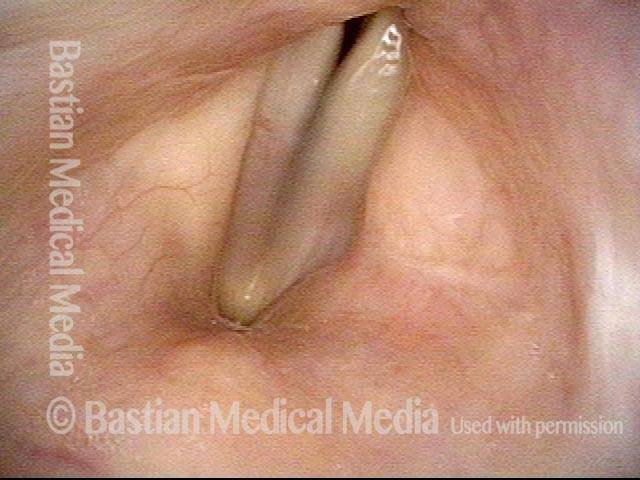
Post laser resection (4 of 7)
Two months after endoscopic transoral laser resection. The normal contours of the supraglottis and medial pyriform have been restored, and the left vocal cord (right of photo) is now fully visible. Her voice has returned to normal.
Postoperative CT (5 of 7)
3 month postoperative CT shows complete excision of mass.

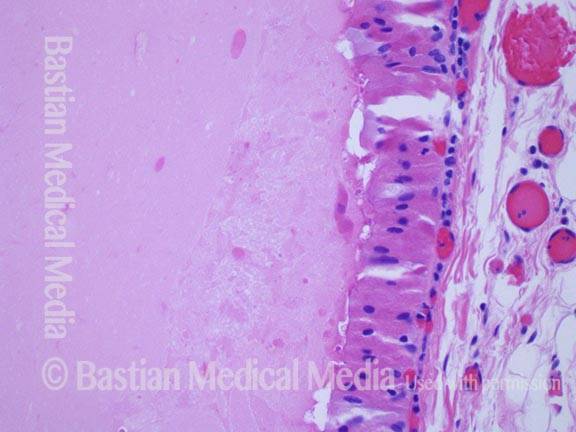
Pathology diagnosis (6 of 7)
Saccular cyst with extensive oncocytic metaplasia. Note the presence of both respiratory ciliated mucosa and granular oncocytic cells in the cyst lining.
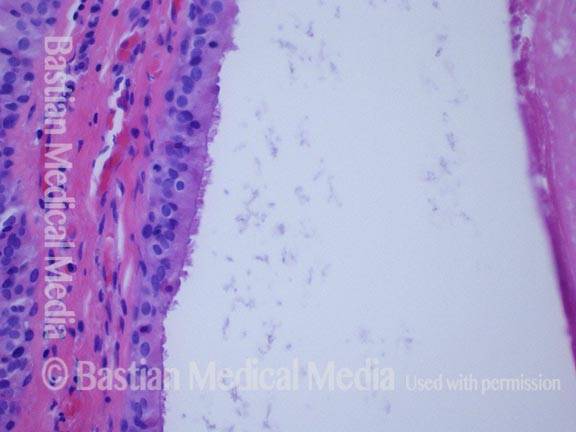
Portion of cyst (7 of 7)
Portion of the cyst, lined by oncocytes.
Polyp or Cyst?
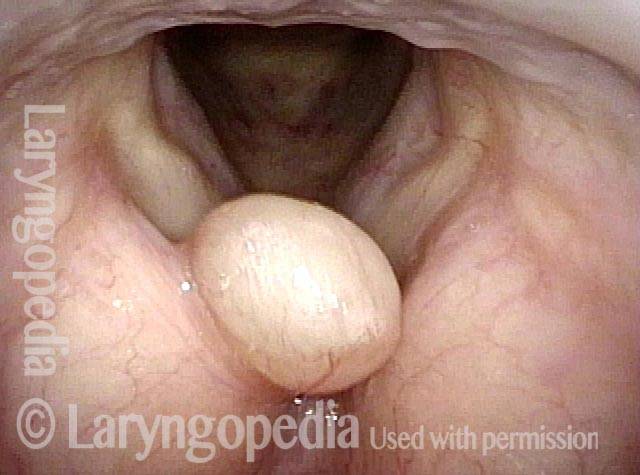
Hoarseness (1 of 4)
During an upper respiratory infection, this older woman developed hoarseness that has not gone away during the past year. Is this the end stage perhaps of a hemorrhagic polyp?

Position of lesion (2 of 4)
In this slightly closer view, with the patient breathing out, the lesion appears too “high” within the laryngeal vestibule, and not truly at the level of the vocal cords.
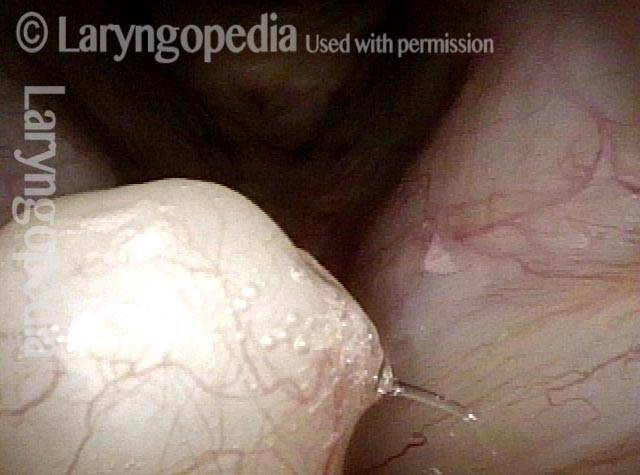
Close view (3 of 4)
This close view is on the way to determining if there is any attachment to the vocal cords themselves. Not quite yet able to tell…
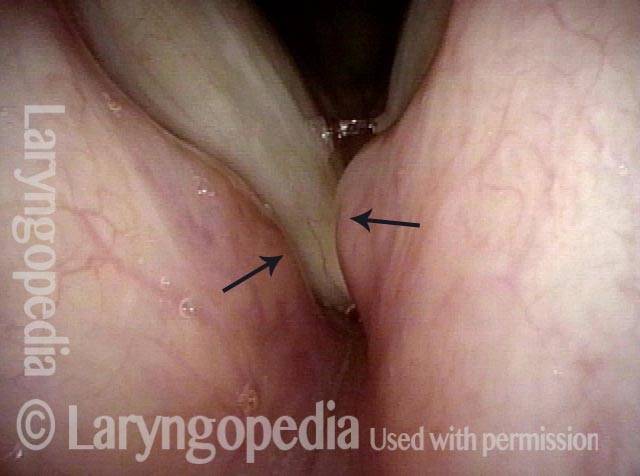
Anterior saccular cyst (4 of 4)
The tip of the scope has just passed the lesion and the vocal cords are unaffected. As it appears to be arising from the ventricle, it could be classified as an anterior saccular cyst. Likely the saccule or a mucus gland became plugged due to inflammation during the upper respiratory infection a year earlier, and it filled with mucus.

Anterior Saccular Cysts, Swellings, and Mucus: What’s the Main Issue?
Are cysts the main issue? (1 of 4)
An experienced R & B singer has begun to experience loss of clarity and a “paper rattling” sound especially upper range. Are the bilateral saccular cysts (arrows) the explanation? Let’s look closer.

Closer range (2 of 4)
At closer range and higher pitch of G4 (392 Hz) produced with light falsetto, now we can also see bilateral margin swellings and a tiny capillary “dot.” Is this the explanation? Let’s look further.

Pressed chest voice (3 of 4)
Now using pressed chest voice more typical of the patient’s singing style at E4 (330 Hz), the saccular cysts come into greater contact and considerable mucus begins to form.

Vibrating cysts and mucus (4 of 4)
Detailed review at the same pitch reveals that the rattling sound comes from a combination of vibratory participation of the saccular cysts, and a “boiling” sympathetic vibration of the mucus. If hydration, and a brief reflux trial do not help, the cysts will be removed.

Anterior Saccular Cysts as Incidental Finding
Polyps? (1 of 3)
This man was examined elsewhere for another reason and sent for evaluation of “polyps” in his larynx. Notice the anterior saccular cysts protruding from the anterior ventricle and false cord margin bilaterally (see arrows). He considers his voice to be normal.
Cysts, not polyps (2 of 3)
At closer range, asterisks mark each cyst.
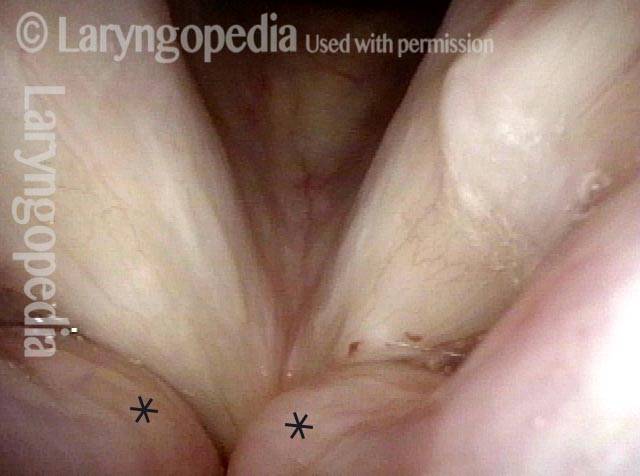
No voice disturbance (3 of 3)
During voice making, notice that neither cyst presses downwards on the vocal cords. That is why voice is normal. Cysts of this sort, diagnosed by intense visual criteria, can be followed once or twice at long intervals, and only occasionally need to be removed due to voice disturbance.

{kind=link}