A cough is an explosion of air from the lungs, sent up between suddenly opened vocal cords, in order to clear the airway of mucus or foreign particles, or in response to certain sensations in the airway, such as a tickle.
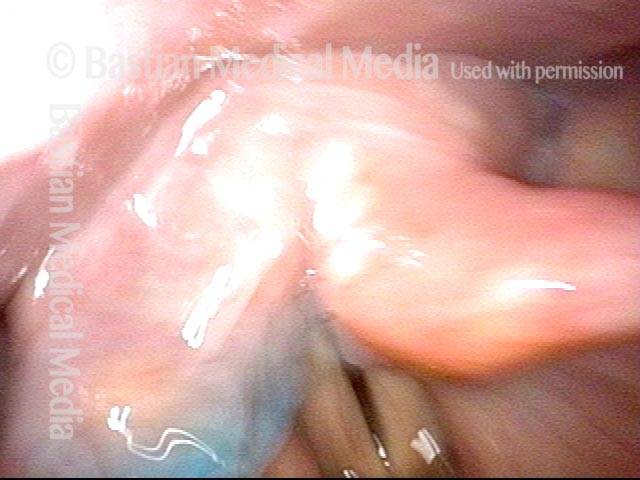
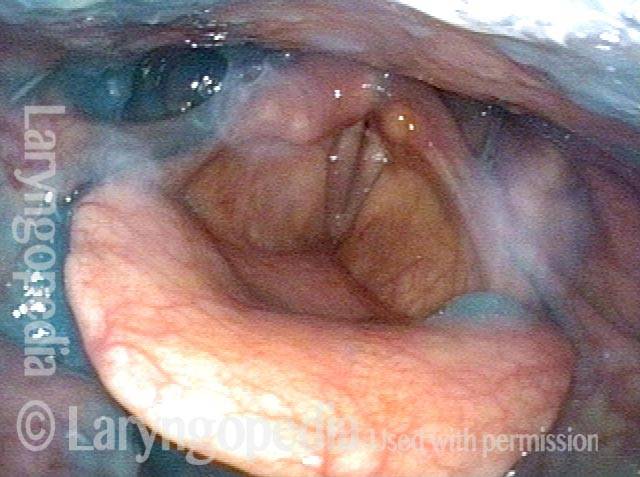
Bruise from coughing (1 of 3)
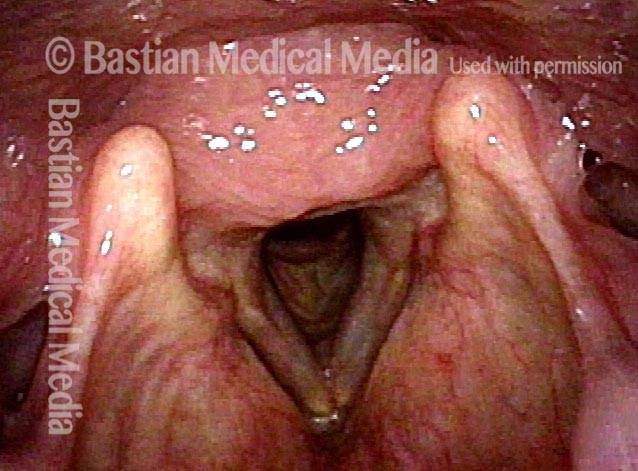
This man had an episode of aggressive coughing a week earlier. Note the bruising over the vocal processes, which receive the major collisional force during coughing.

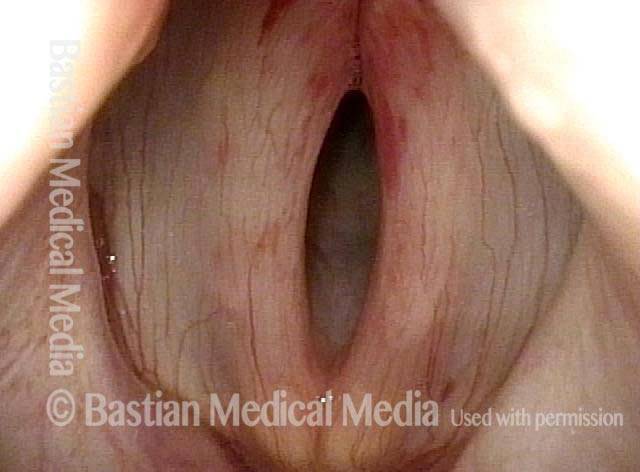
Pre-phonatory instant (2 of 3)
The vocal processes are approaching the point of touching (contact would occur gently with onset of talking and more aggressively with coughing).

Phonation (3 of 3)
Vocal cords are now in full contact. Note the unrelated moderately-severe vocal cord bowing.
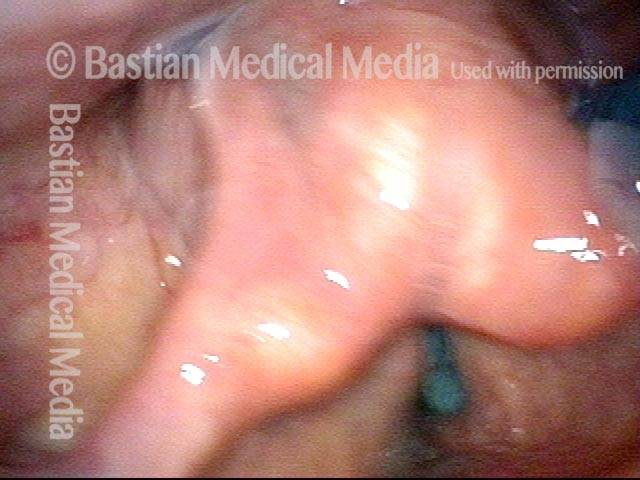
Bruise Caused by Cough
Closer view of bruise (2 of 2)
Closer view of bruise, with small collection of white mucus in the middle.
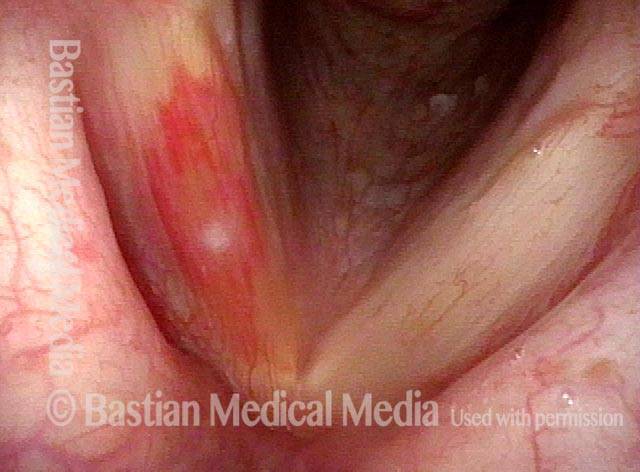
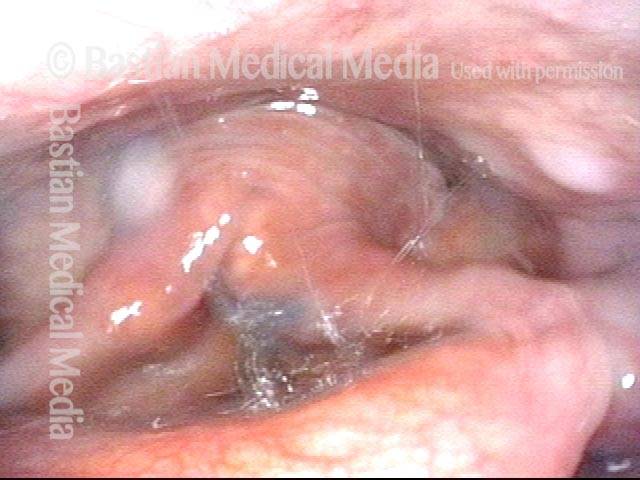
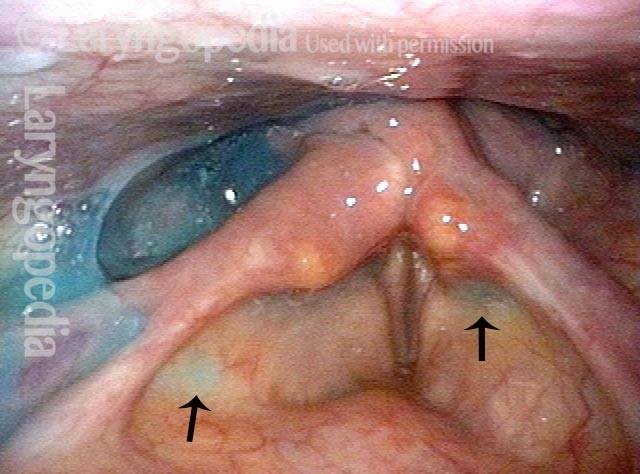
Bruise caused by violent coughing (1 of 2)
A person with violent sensory neuropathic coughing may injure the vocal cords, as illustrated by this bruise, right vocal cord (left of photo).
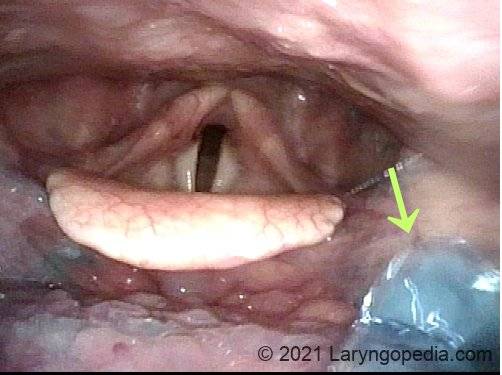
Aspiration
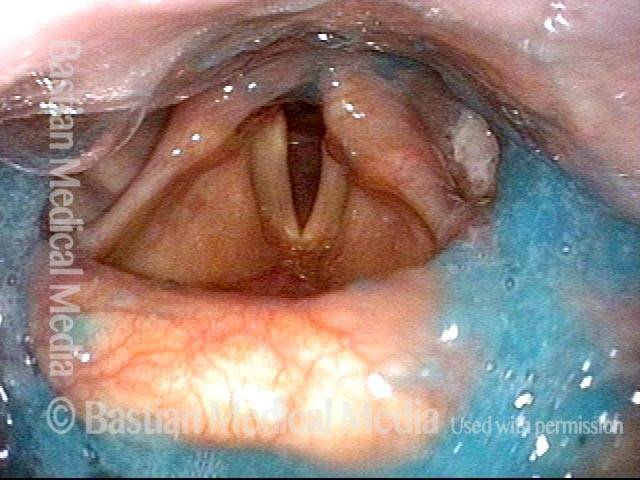
Aspiration
After patient swallows blue-stained applesauce, some enters the trachea. Vigorous coughing can clear this away so that even chronic aspiration of this sort does not necessarily cause pneumonia.

Tracheal Hyperflexibility
Tracheal hyperflexibility (1 of 6)
This patient has COPD as well as a “wet and productive” sounding cough. The explanation for this is not actual mucus, but tracheal vibration that sounds like a mucus-y cough. This panoramic view shows inspiration and normal abduction of the vocal cords. As we will see in photo 3, the trachea is patent at this moment.
Tracheal hyperflexibility (2 of 6)
Expiratory partial closure of the true vocal cords, similar to the lip-pursing maneuver persons with COPD often use to prevent lower airway collapse. As we see in photo 4, collapse is happening in spite of this lip-pursing maneuver.

Tracheal hyperflexibility (3 of 6)
Mid-trachea during deep inspiration, corresponding to the vocal cord position in photo 1. The white arrow indicates a speck of mucus which will also be seen in photo 4.
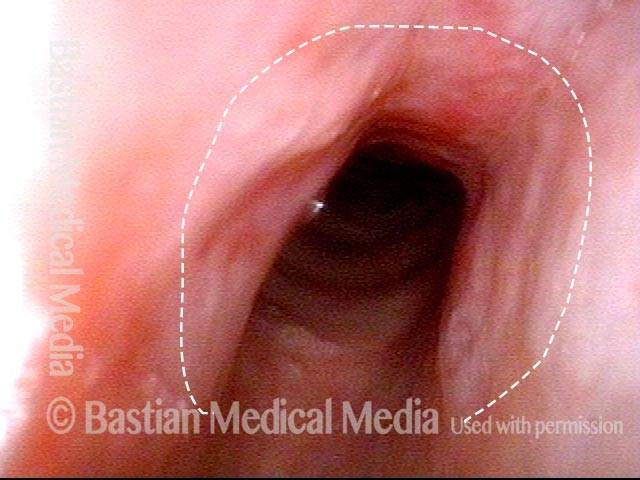
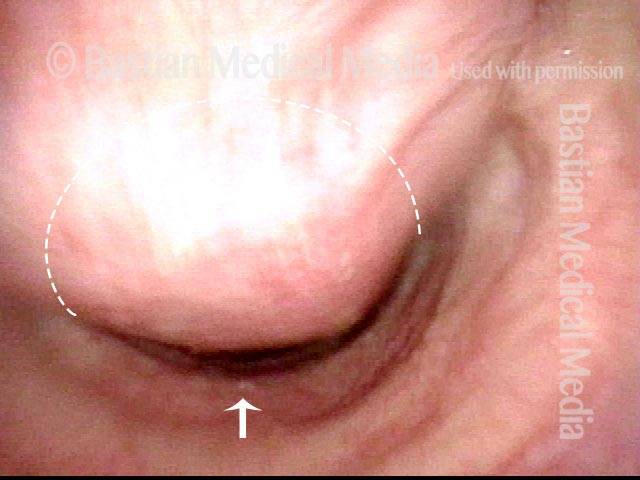
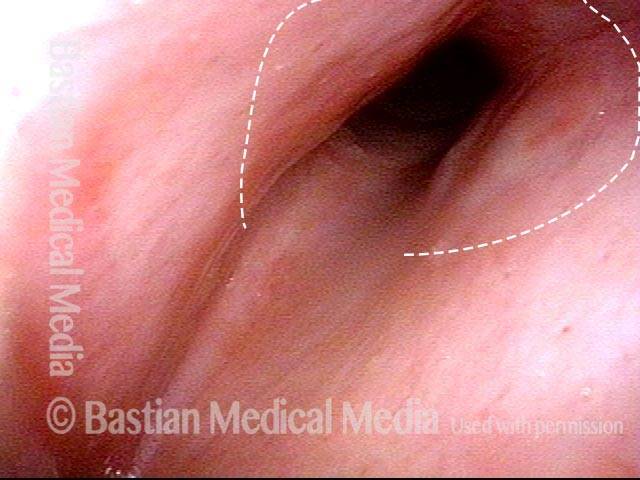
Tracheal hyperflexibility (4 of 6)
Mid-trachea, showing the same position as photo 3 but now during expiration. The membranous tracheal wall is bulging inward and nearly blocking the trachea. A wheezing sound is heard as air whistles though this narrow lumen (the expected lumen is indicated by the curved dotted line). The same speck of mucus that was seen in photo 3 is indicated again by the white arrow.
Tracheal hyperflexibility (5 of 6)
A little farther down the trachea, during inspiration.

Tracheal hyperflexibility (6 of 6)
At the same position as photo 5, during a cough. The membranous trachea not only bulges inward, but it also vibrates impressively (note blur), creating a deep and rumbling cough whose “wet” quality is not actually from mucus, but from vibration of the tracheoesophageal party wall.

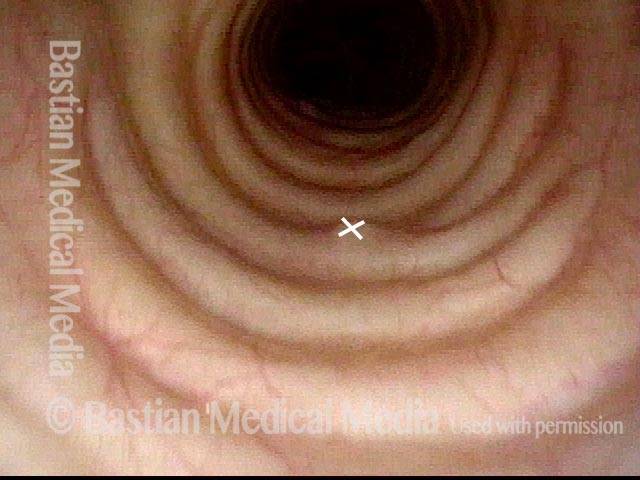
Tracheal Dynamics of a Cough that Is Normal but “Wheezy.”
Distal trachea (1 of 2)
Distal trachea, where it splits into the two mainstem bronchi. Arrow at speck of mucus is just for reference to photo 2.

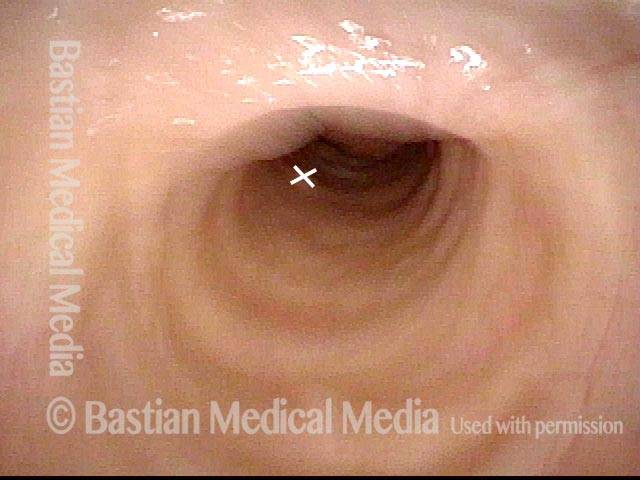
Tracheal membrane (2 of 2)
The patient is coughing at this moment, and the membranous tracheal wall bulges to partially block the trachea, causing a wheezing component to the sound of his cough. This tracheal physiology is seen to some degree when virtually everybody coughs, and it helps to speed the velocity of air exploding upwards from the lungs as it must pass through the narrowed segment.

VESS Demonstrating Presbyphagia, Chin Tuck Maneuver, Hypopharyngeal Pooling, Laryngeal Penetration and Effective Cough
VESS (1 of 5)
The patient swallowed a bolus of blue-stained applesauce to verify basic (though abnormal) capability. This photo follows 4 additional boluses delivered in a rapid, pressured fashion, intentionally seeking the patient’s “limits.” Note pooled blue applesauce, but without soiling of the laryngeal vestibule.
Chin tuck maneuver (2 of 5)
Moments later, the patient was asked to swallow again, but with chin tucked down towards chest. Note how effective this maneuver was in clearing away the residual material seen in the prior photo.

Aspiration (3 of 5)
Due to its lower viscosity, blue-stained water flows more quickly than applesauce, and enters the laryngeal vestibule. Fortunately, the patient is closing the vocal cords simultaneously, so that aspiration does not occur.
Laryngeal penetration (4 of 5)
Just after the swallow is completed, one can see a trace of blue-stained water just above the not-yet-opened cords. This is technically penetration, and not aspiration.
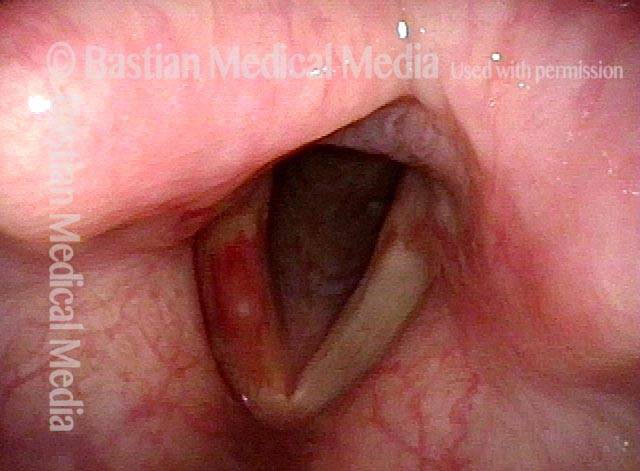
Air is blasted out of vestibule (5 of 5)
Using “stored” pulmonary air, this trace of penetrated water is “blasted” up and out of the laryngeal vestibule, and is never aspirated.”
All It Takes Is A Drip to Make You Cough
Coughing (1 of 4)
This patient is annoyed by occasional coughing when she sips liquids. She has had no pneumonias, weight loss, or increased time required to eat/drink. Here, the patient has just taken a sip of blue water and holds it in her mouth.

Coughing (2 of 4)
Just before swallowing, a tiny drip of blue water “gets away” and begins to trickle down into her throat. Vocal cords remain unsuspectingly open.
Coughing (3 of 4)
The drip (arrow) has now reached the left aryepiglottic fold, which is the “side of the boat” that keeps liquid out of the airway. The drip looks smaller than in photo 2 because it is farther away. She does not cough.
Coughing (4 of 4)
During a different swallow, if a much larger amount of water were to drip prematurely down into her throat, a part of it would enter the laryngeal entrance and provoke coughing. If coughed back up, there would be little risk of pneumonia.
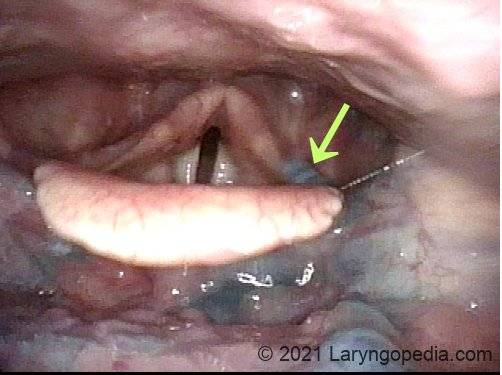
Rumbling Vibration of the Tracheoesophageal Party Wall can make Coughing Sound “Infectious and Productive” when it isn’t
Tracheobronchial cough vibration (1 of 2)
Patient with SNC who is treated for presumed infection because of her congested rumbling “productive-sounding” cough. The “X” marks the same place in this photo and the following photo.
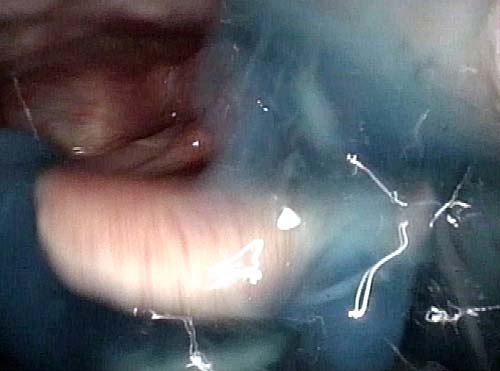
Tracheobronchial cough vibration (2 of 2)
Patient is at the moment of a deep, productive-sounding cough, but in fact it is not productive. Her many courses of antibiotics are probably unnecessary. The narrowing of the lumen is due to inward bulging of the membranous tracheal wall. The blur is caused by vibration during this cough.
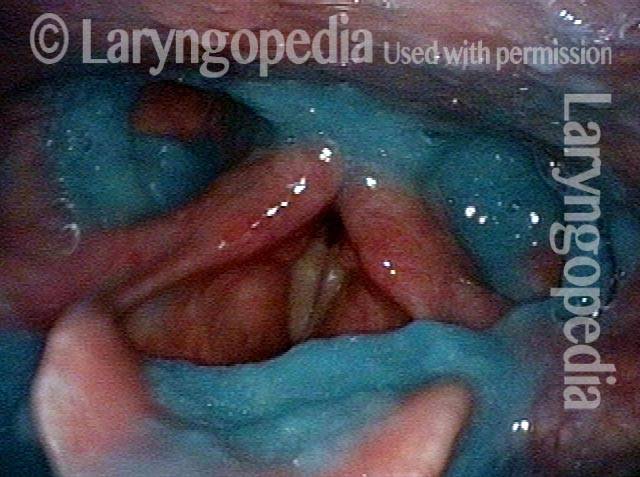
Secretional Pooling Predicts Swallowing Function
Pooling (1 of 4)
This man coughs frequently especially when drinking. While his palate elevation, pharynx squeeze, and vocal cord functions are intact (as determined during VESS part 1A), note the pooling of saliva especially in the right pyriform sinus (left of photo) and on the pharyngeal wall (arrows) as well as within the laryngeal vestibule (bottom, left arrow). This predicts that his swallowing of blue-stained applesauce, water, and cracker will also be abnormal.

Residue (2 of 4)
As predicted by the information in photo 1, after administration of blue-stained applesauce, we see here an amount and location of residue that mirrors that of the saliva in photo 1. Greater residue in the right pyriform sinus (left of photo) is often seen with right-sided pharynx weakness, but that is not the case here.
Cracker (3 of 4)
After administration of cheese cracker, some of it remains in the vallecula, where it has displaced some of the applesauce.

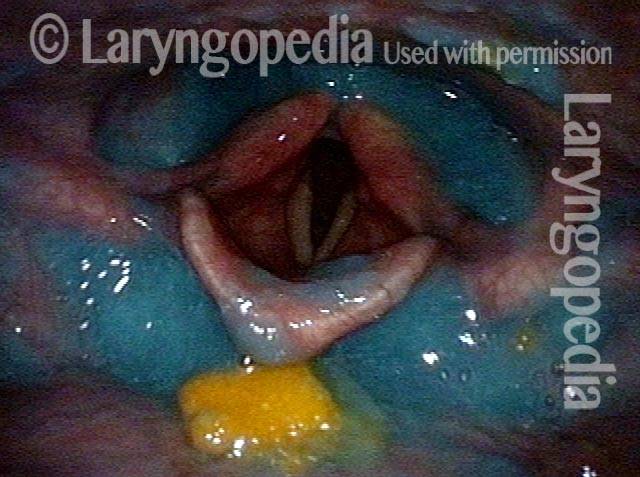
Blue-stained water (4 of 4)
After administration of blue-stained water, most of cracker and applesauce are washed through. Some minimal blue-staining of the laryngeal vestibule explains why coughing tends to occur when drinking (especially thin liquids).
Aspiration, and Fountain of Returned Aspirate after Coughing
Salivary pooling (1 of 5)
This young man has a chromosome disorder. He has trouble swallowing but no history of pneumonia. The palate, pharynx, and larynx motor function is normal, but the salivary pooling seen here predicts what follows…

After applesauce (2 of 5)
After several boluses of blue-stained applesauce, there is significant pooling (residue), but nothing down at the level of the vocal cords.
After cheese cracker (3 of 5)
After chewing and swallowing a cheese cracker, a part is lodged in the vallecular.
After water (4 of 5)
During administration of blue-stained water, a large drip is seen falling downwards, directly into the laryngeal vestibule.
Cough expels the water from airway (5 of 5)
A moment later, a cough sprays the aspirated blue-stained water upwards and out of the airway.

Who knew…? Many Such Injuries Are Never Found
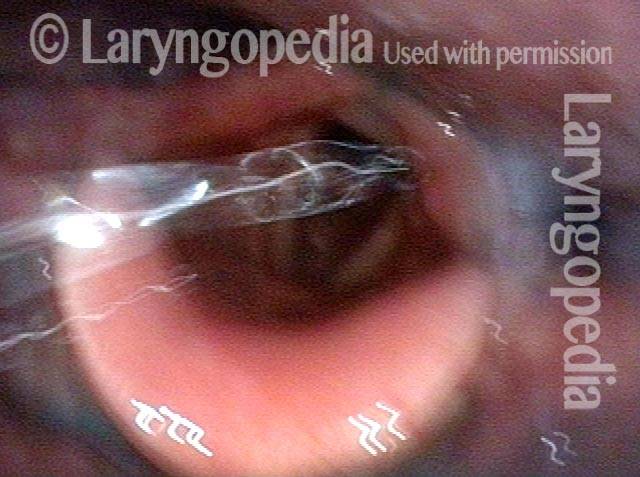
Coughing evaluation (1 of 6)
An octogenarian is being evaluated for recent coughing of months duration. To evaluate her complaint of major mucus production, an “exam of opportunity” mini-bronchoscopy was done. Salivary pooling (see bubbles) is seen, likely due to interference with swallowing caused by topical anesthesia.
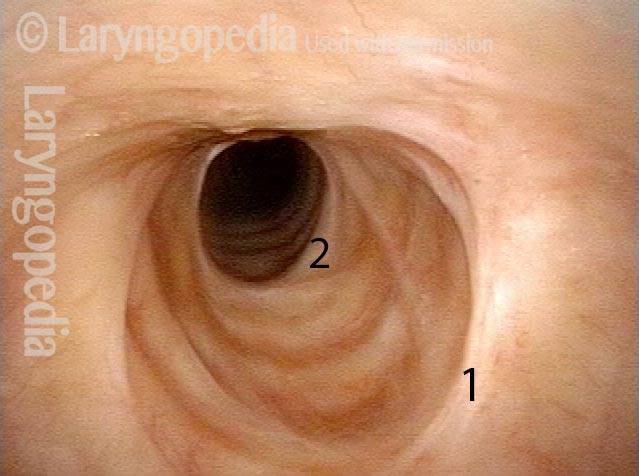
Intubation scars (2 of 6)
Just barely through the vocal cords, two circumferential scars are seen at 1 and 2. This prompted a conversation during which the patient noted that decades earlier, she had been intubated for 11 days during a grave illness.

Stenosis (3 of 6)
At closer range, the zone of stenosis is seen better. This is an incidental finding at this time, and is not responsible for her sensory neuropathic cough. She has no shortness of breath or sense of exercise limitation.
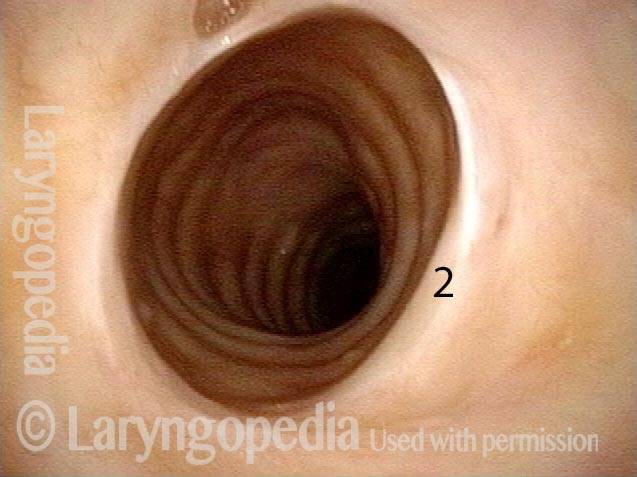
Further down trachea (4 of 6)
The trachea beyond the lower edge of the scarred segment is of normal caliber but turns to the patient’s left, giving the illusion of distal narrowing.
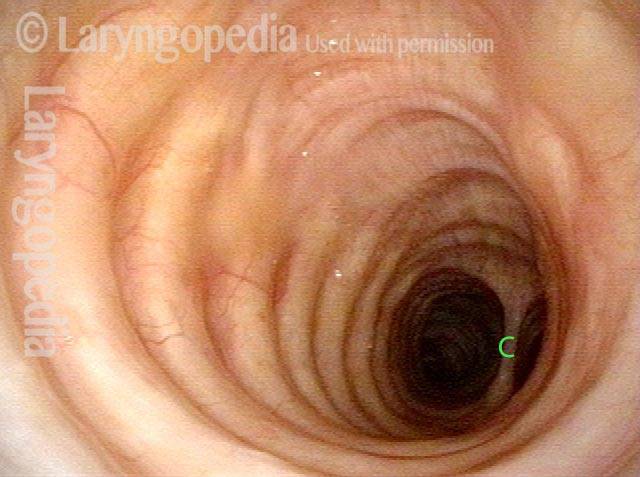
Below stenosis (5 of 6)
Just below the stenosis, the normalcy of the distal trachea is better seen. The carina is at C.
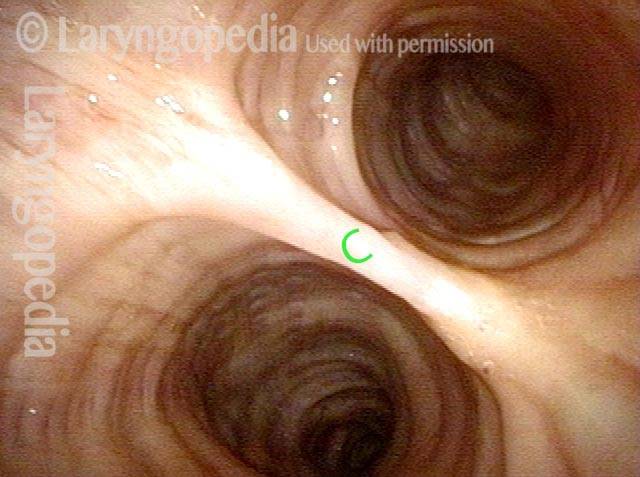
Carina (6 of 6)
Right at the carina, and looking into both mainstem bronchi. Many persons who have been intubated for a long period of time likely have asymptomatic and therefore undetected and inconsequential scars like those seen in photos 2, 3, and 4.
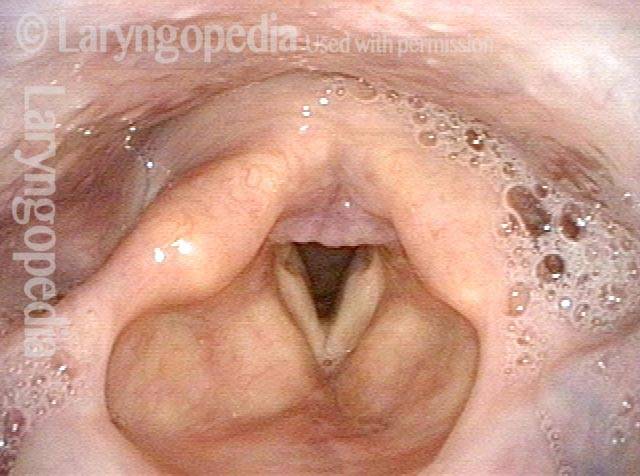
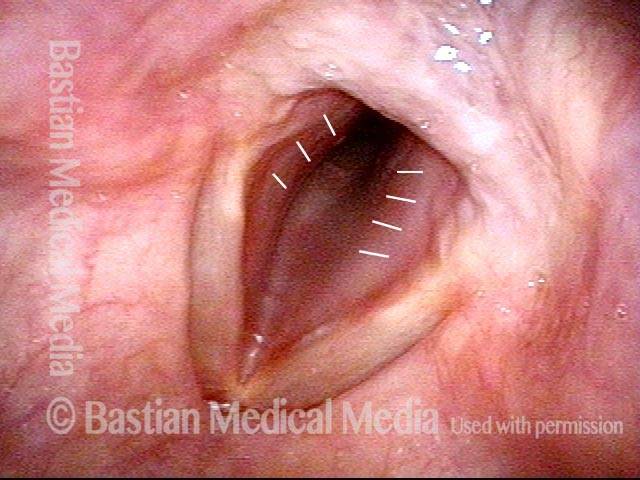
Croup, aka Laryngotracheitis
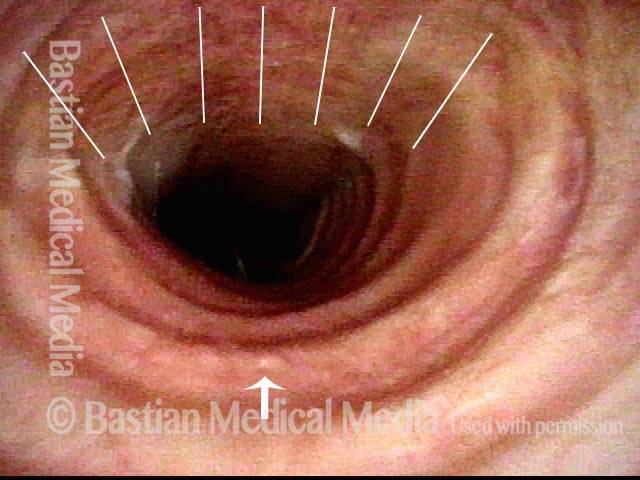
Croup, aka laryngotracheitis (1 of 4)
Though croup is most often seen in children, this woman developed a barking cough and mild, non-anxiety provoking stridor in the context of an upper respiratory infection. In this panoramic view note in particular the prominence and redness of the conus part of the vocal cords (indicated by white lines).
Croup, aka laryngotracheitis (2 of 4)
Closer view. Dotted lines signify normal airway diameter.
Croup, aka laryngotracheitis (3 of 4)
Even closer view showing redness and narrowing of the posterior subglottic airway.
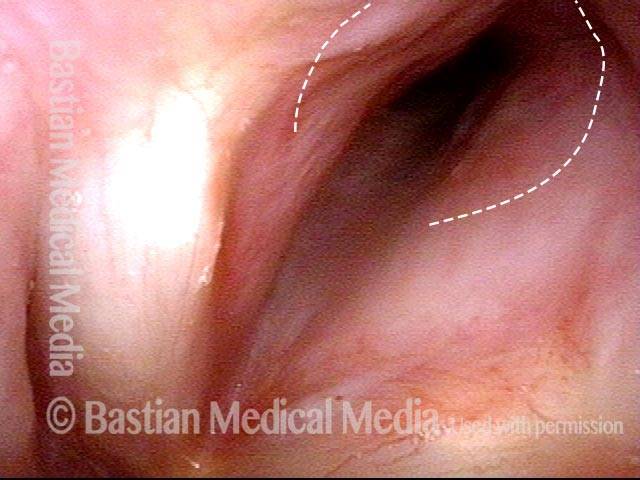
Croup, aka laryngotracheitis (4 of 4)
View within the posterior subglottic narrowing.