Can’t Burp?
You’ve come to the right place.
![]()
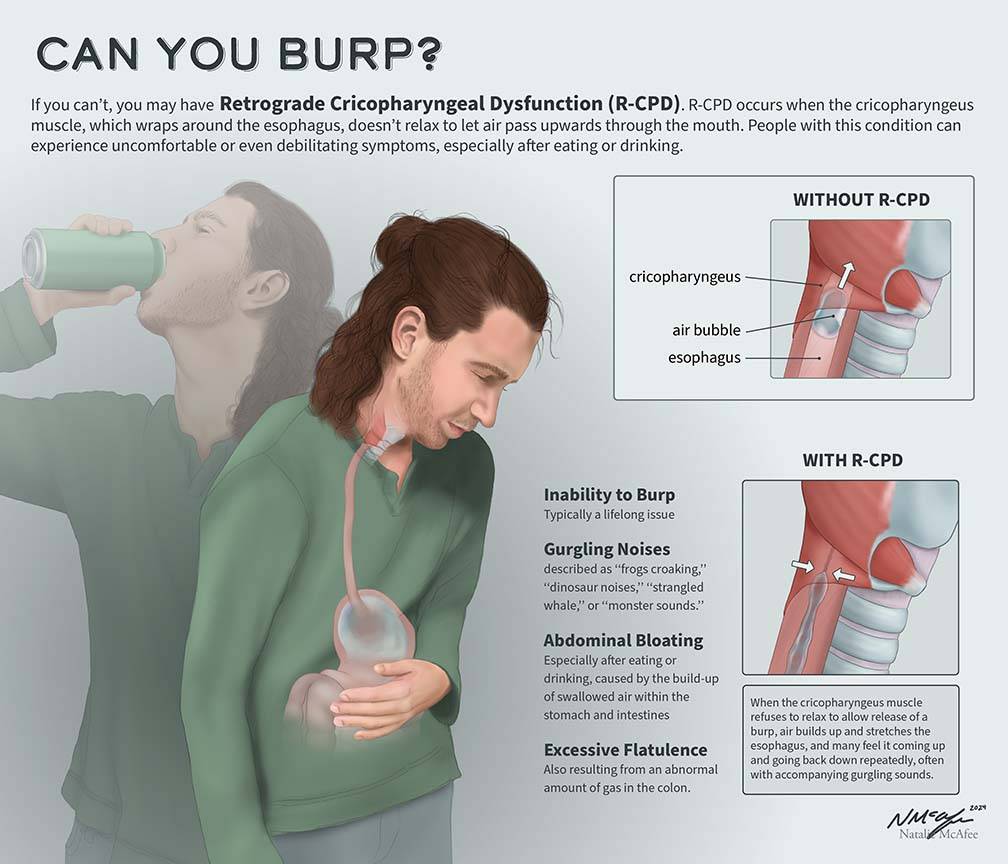
What is R-CPD (Inability to burp, no-burp)?
![]()
The Top 4 Symptoms of R-CPD

![]()
Less Common Symptoms of R-CPD
![]()
What Causes R-CPD?
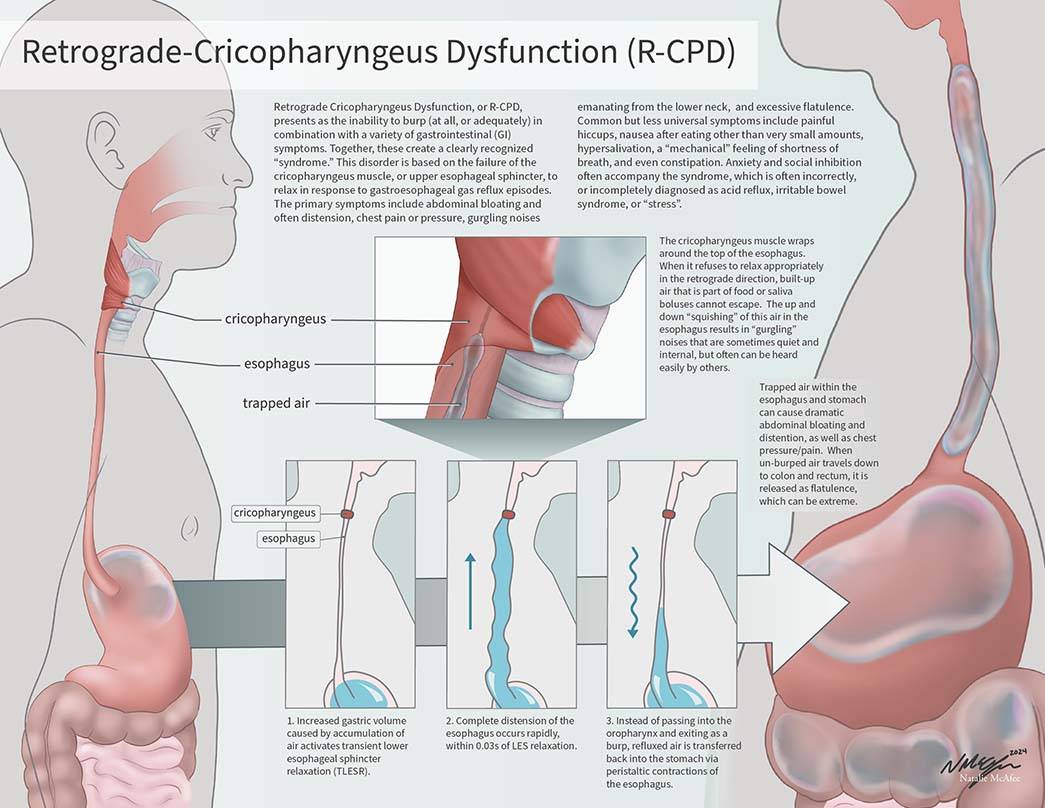
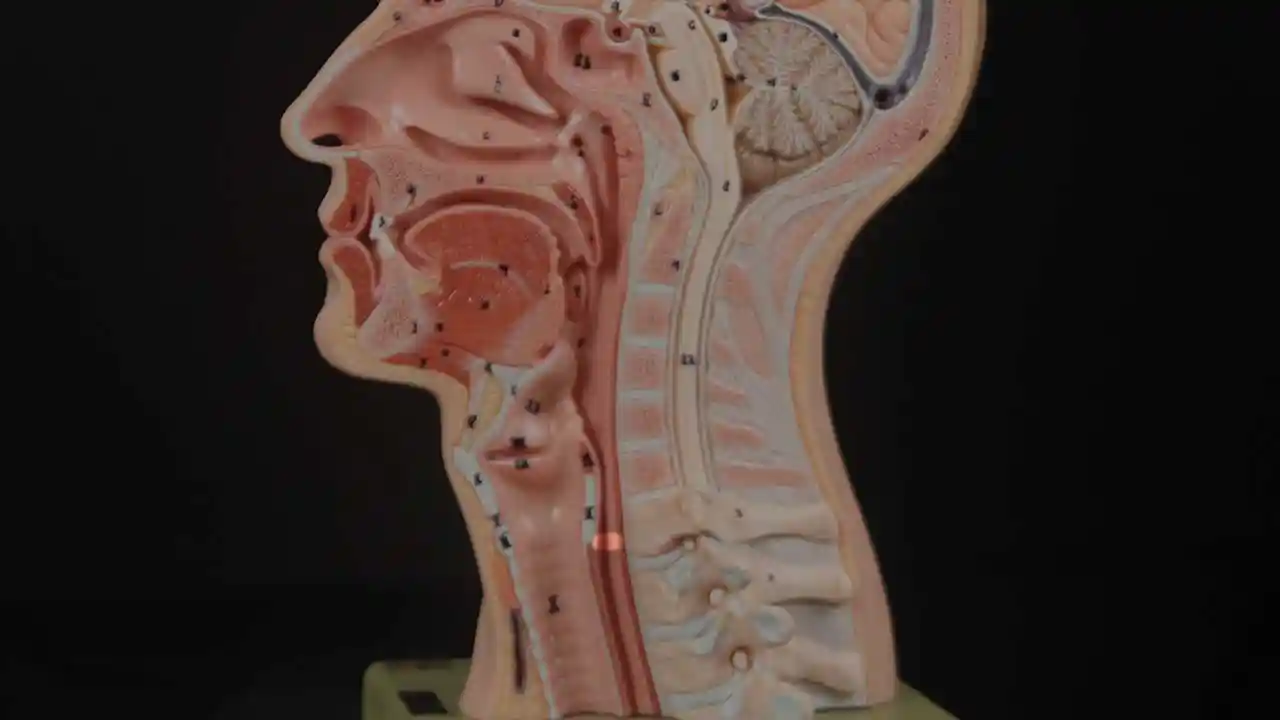
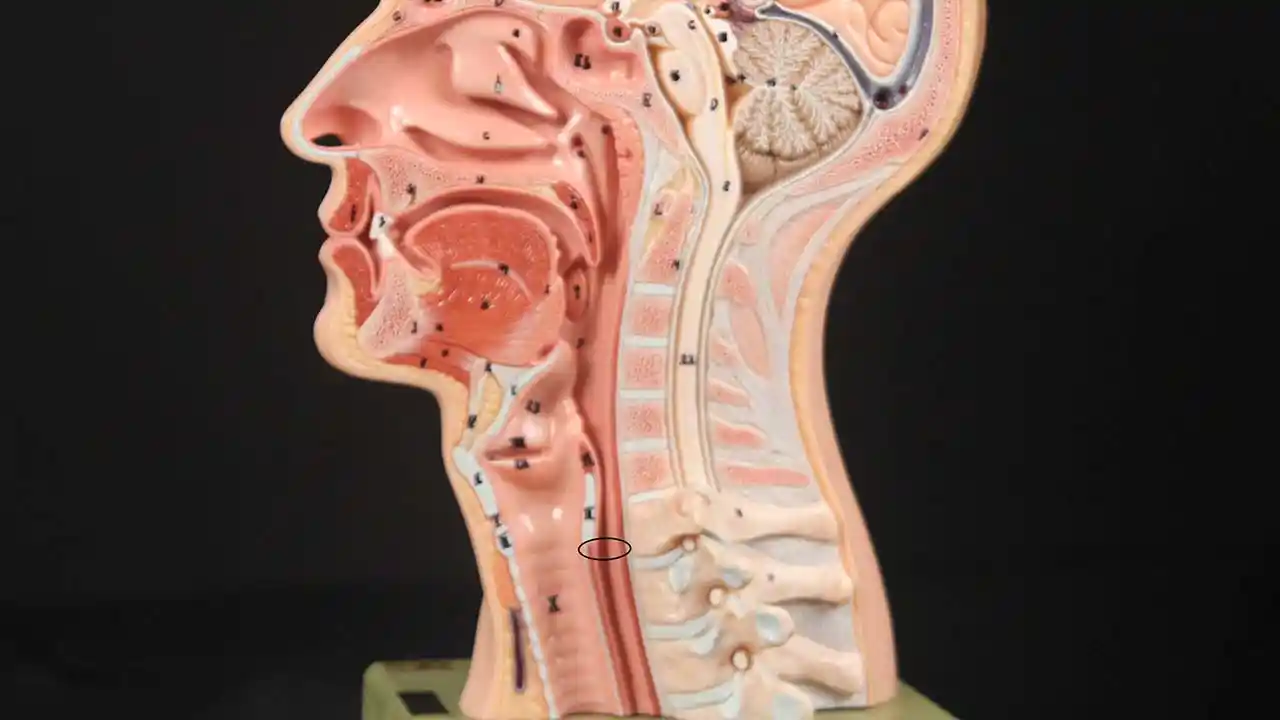
Inability to burp or belch occurs when the upper esophageal sphincter (cricopharyngeus muscle) cannot relax in order to release the “bubble” of air. The sphincter is a muscular valve that encircles the upper end of the esophagus just below the lower end of the throat passage. If looking from the front at a person’s neck, it is just below the “Adam’s / Eve’s apple,” directly behind the cricoid cartilage.
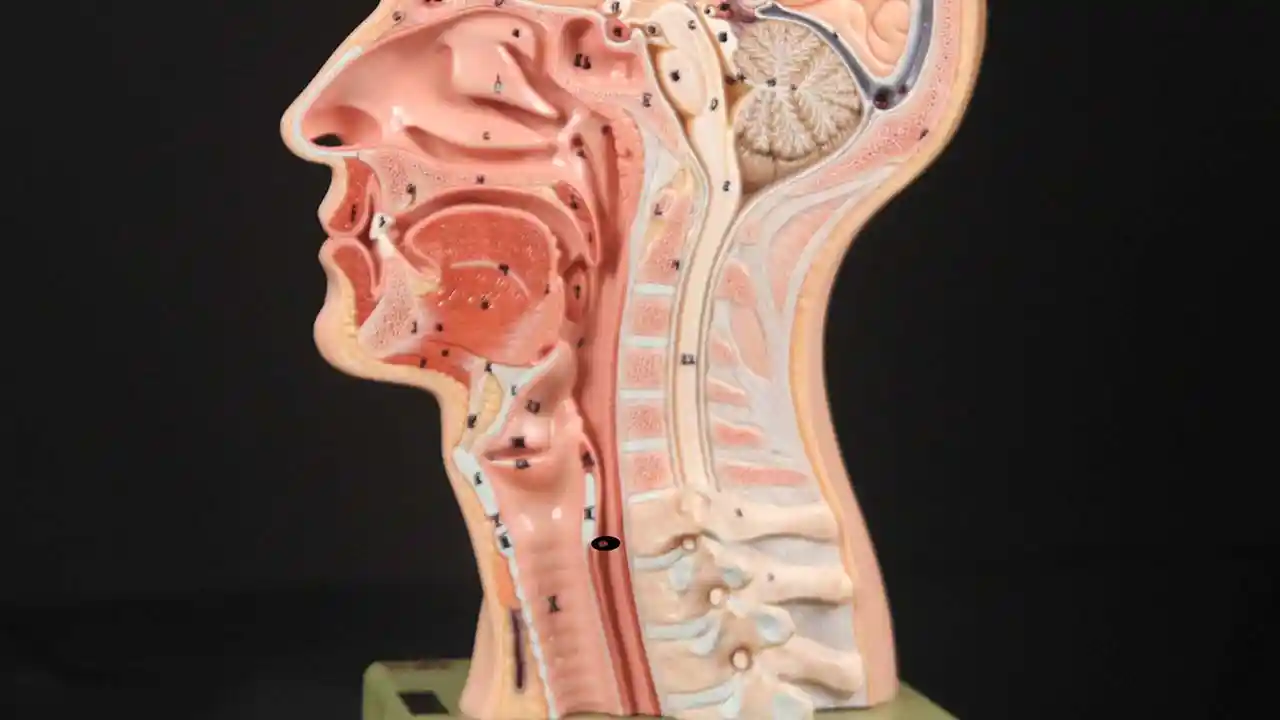
If you care to see this on a model, look at the photos below. That sphincter muscle relaxes for about a second every time we swallow saliva, food, or drink. All of the rest of the time it is contracted. Whenever a person belches, the same sphincter needs to let go for a split second in order for the excess air to escape upwards.
In other words, just as it is necessary that the sphincter “let go” to admit food and drink downwards in the normal act swallowing, it is also necessary that the sphincter be able to “let go” to release air upwards for belching.
Cricopharyngeus Muscle (1 of 3)
Open Cricopharyngeus Muscle (2 of 3)
Closed (3 of 3)
![]()
Treatment for R-CPD
Botox Injection at Bastian Voice Institute
For people who experience this problem to the point of discomfort and reduced quality of life, here is one approach:
First, a videofluoroscopic swallow study, perhaps with effervescent granules. This establishes that the sphincter works normally in a forward (antegrade) swallowing direction, but not in a reverse (retrograde) burping or regurgitating fashion. Along with the symptoms described above, this establishes the diagnosis of retrograde-only cricopharyngeus dysfunction (non-relaxation).
Second, a treatment trial involving placement of Botox into the malfunctioning sphincter muscle. The desired effect of Botox in muscle is to weaken it for at least several months. The person thus has many weeks to verify that the problem is solved or at least minimized. (See video, What Tests are Necessary for R-CPD?)
The Botox injection could potentially be done in an office setting, but we recommend the first time (at least) placing it during a very brief general anesthetic in an outpatient operating room. That’s because the first time, it is important to answer the question definitively, that is, that the sphincter’s inability to relax when presented with a bubble of air from below, is the problem.
Lifting the CPM for a R-CPD Injection
These are intra-operative photos of one of nearly 2,000 persons treated for R-CPD as of December 2024. This sequence shows several things:
- The dilated, “always open” esophagus distal (below) the muscle
- How to identify the cricopharyngeus muscle
- One way of injecting the muscle.
Above the CPM (1 of 5)

Ridge of the CPM (2 of 5)

Exposed CPM (3 of 5)

CPM Palpated (4 of 5)

Botox injection (5 of 5)

How Many Units of Botox Should My Doctor Inject for R-CPD?
Unsatisfyingly, the answer is “that depends,” for two main reasons. The first is placement. If the doctor’s is very accurate, the amount injected can be less than if inaccurate. (And any good ENT doctor should be able to aim accurately without difficulty.)
The second reason is the innate difference of individual sensitivity to Botox. It is known from other sites that one person may need a bigger dose than another to get the same result. And it doesn’t correlate with age, sex, weight, height, etc. and so there is no predicting…
In the larynx, where we inject botox for a rare neurological voice disorder, the dose varies by a factor of at least 20. Most lie in a middle range, of course, but there are “outliers” on both the “hypersensitive” and “insensitive” ends of the scale.
The muscle we are injecting is small, and that is why I initially thought that 50 units—the dose I used for my first 200 patients—was generous. That dose worked well for virtually everyone I injected. In fact, it was likely a higher dose than needed for some. But it was not enough for the very occasional patient. And so, to “capture” the rare patient who needs higher dose, I increased to 75 units for approximately the next 700 patients.
Again, a really good result followed for “almost” all 700. But for the next 150 or so, I used 100U for two reasons. One is that the patient has purchased the entire vial of 100, so I figure to just give the full amount. The second is that so many travel from such a distance (even internationally) that we want to make certain even if they are a bit insensitive to Botox, they still get a good result…
So many patients would do fine with 50 or even 75, but the above reasons explain my current dose of 100. To repeat, keep in mind it is not only dose but – critically – accurate placement that may determine the effectiveness of any given injection. Thankfully targeting is only occasionally difficult, so most people will do well with 50, 75 or 100. If we could know in advance each individual’s dose requirement, I am sure some would do well even with 25 units!
Is there any downside to using a higher dose than (in retrospect) would have been necessary?
The only downside of higher dose would be a bit more of the initial “slow swallow” which everyone gets through…
What to Expect Post Botox Procedure?
Review Dr. Bastian’s published Journal entry for a complete explanation, but in a nutshell:
- There will be no relief of R-CPD symptoms for 1—5 days.
- Only when micro-burps begin do patients start to notice the beginning of symptom relief. So do not try carbonation for lunch on the day of the injection!
- Initial Botox side effects can be “weird” for a few days to weeks.
- If you can manipulate your gurgles prior to Botox treatment, to make them softer or louder, use that technique to see if you can hurry burps along or make them bigger.
For a few months at least, patients should experience dramatic relief of their symptoms. And, early experience suggests that it may be that this single Botox injection allows the system to “reset” and the person may never lose his or her ability to belch. Of course, if the problem returns, the individual could elect to pursue additional Botox treatments, or in a truly severe case, might even elect to undergo endoscopic laser cricopharyngeus myotomy.
![]()
Frequently Asked Questions
![]()
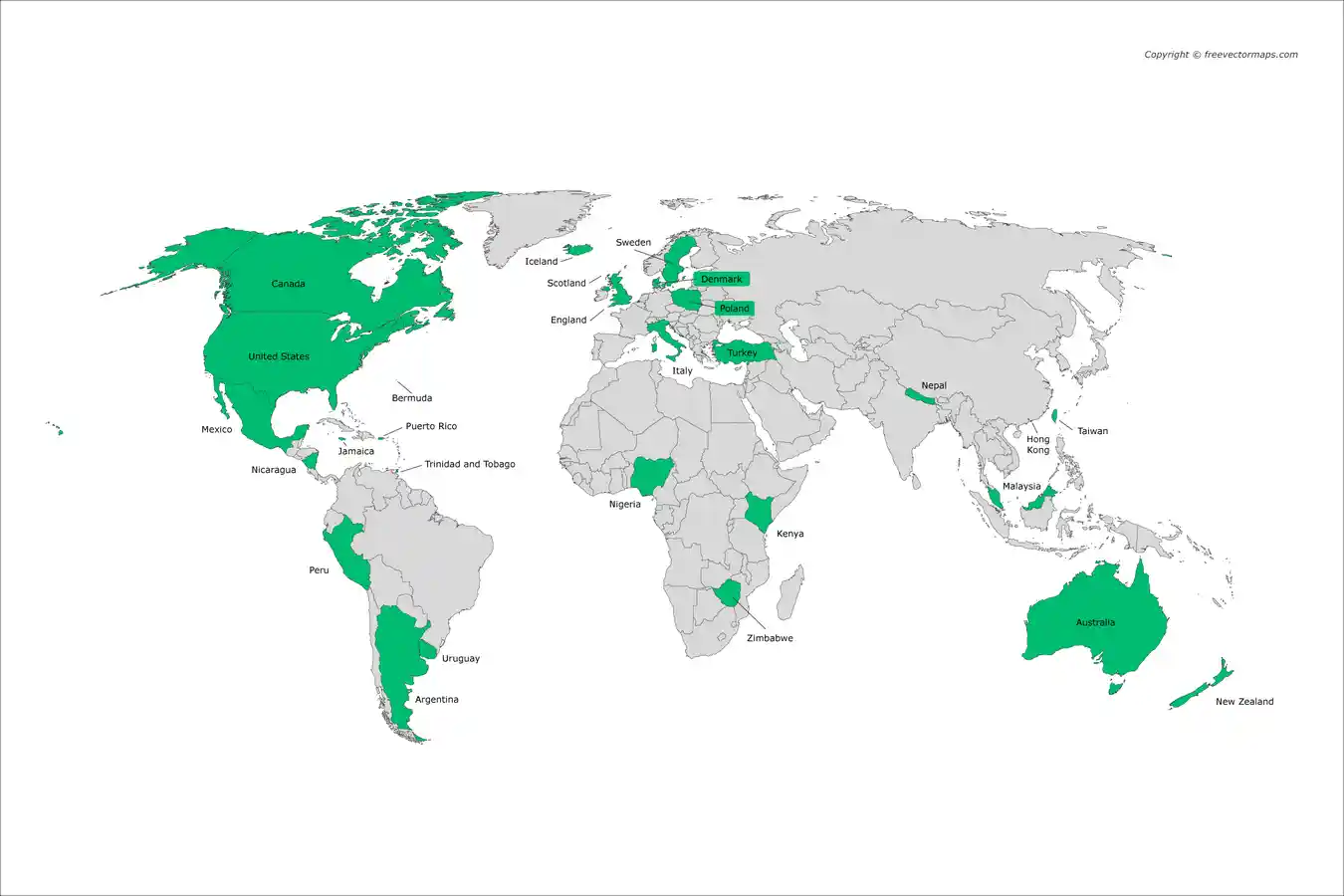
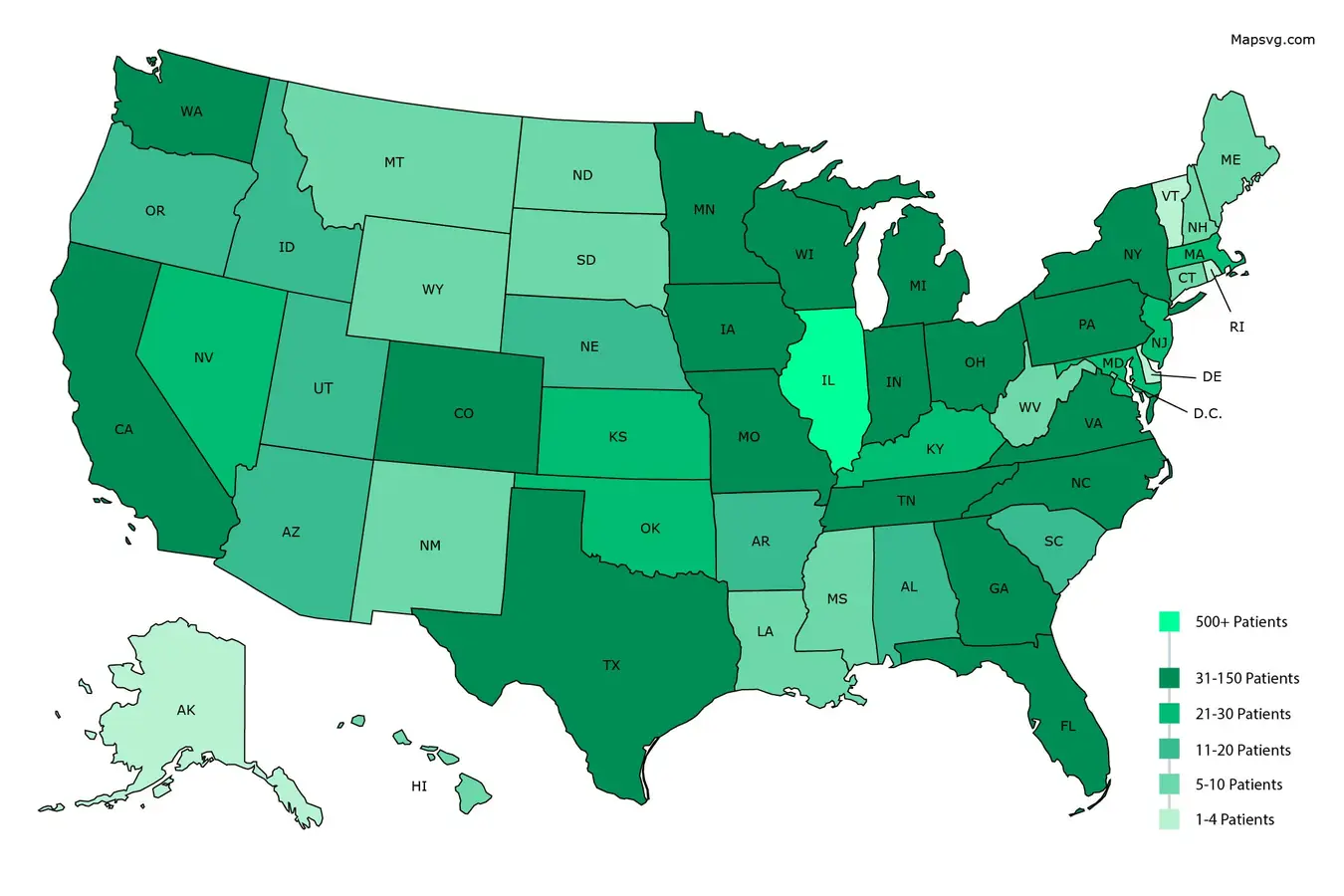
Where do Our R-CPD Patients Come From?
![]()
Photo Essays from our R-CPD Patients
R-CPD, Aerophagia and Burping
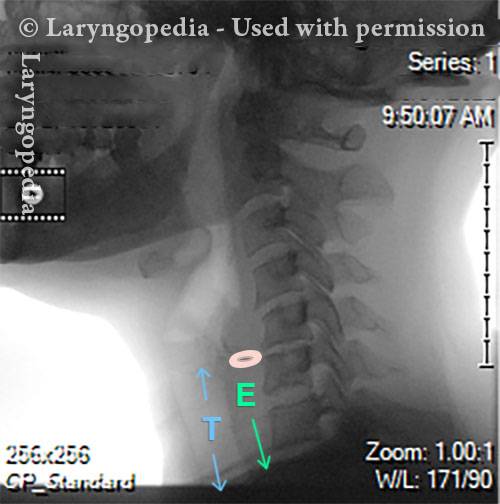
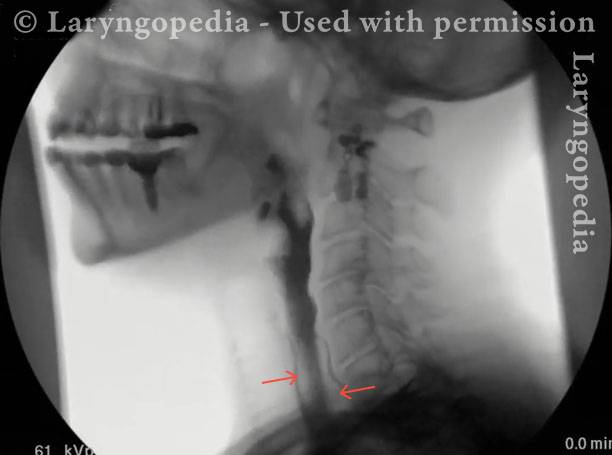
This lateral x-ray of the neck is part of a swallow study, and illustrates how air can accumulate and need to be burped up. The focus of this post is the esophagus, or “foodway,” that connects the lower part of the throat to the stomach. The esophagus is a muscular tube that remains mostly collapsed—closed—except when food, liquid, or saliva traverses it.
X-Ray of Larynx (1 of 6)
Barium swallow (2 of 6)

Collapsed esophagus (3 of 6)

Air is swallowed (4 of 6)
UES refuses to open for a burp (5 of 6)

Abdominal Distention from R-CPD (6 of 6)
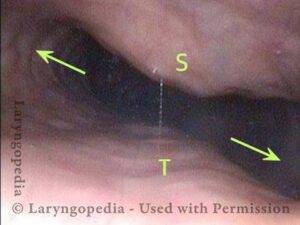
R-CPD Neck Symptoms and “Throat Nausea”
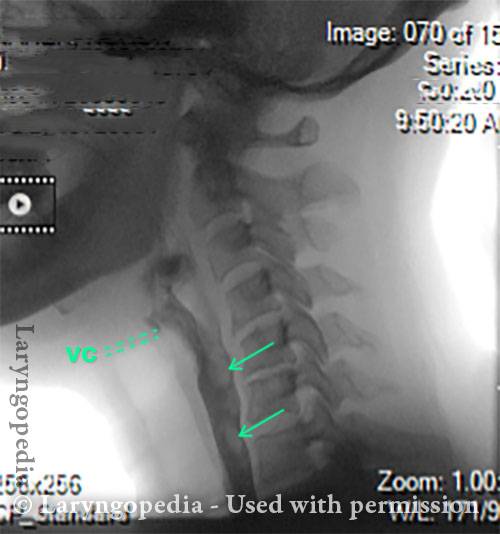
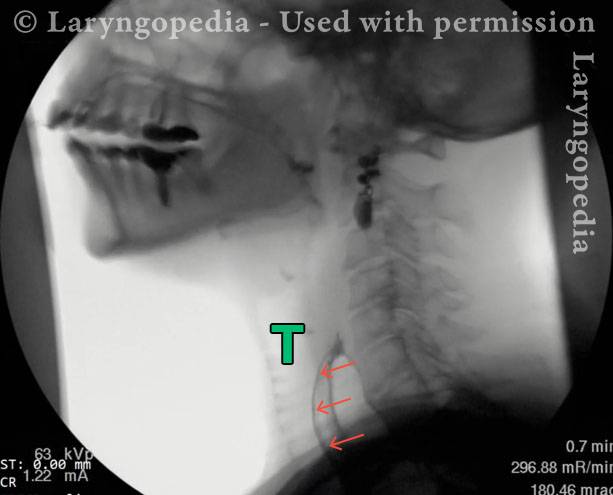
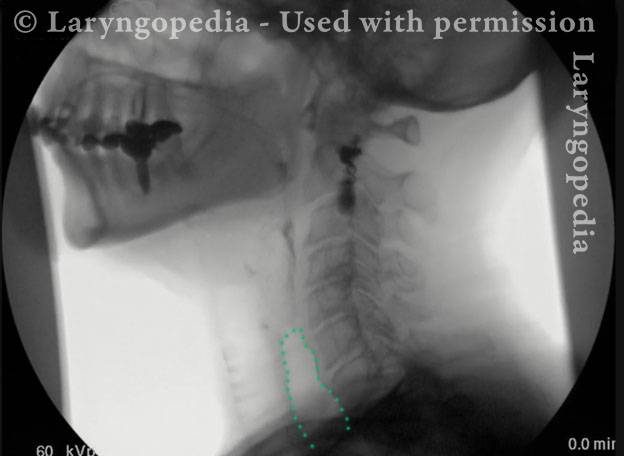
This visual series depicts a hallmark feature of R-CPD: marked dilation of the upper esophagus filled with swallowed and retained air. Normally, this air would be burped out, but in persons with R-CPD, it cannot be expelled.
The retained air can push upward, creating a sense of pressure and a distinct gagging or “throat nausea” sensation. It also explains a striking procedural observation: during office upper esophagoscopy, air insufflation is unnecessary, because the patient’s esophagus is already dilated by trapped air, allowing visualization of its walls. Read full article here.
X-Ray of Dilating Air (1 of 4)

Retained Air in Larynx (2 of 4)
Esophagus bulges anteriorly (3 of 4)
Air remains after swallow (4 of 4)
Abdominal Distention of R-CPD
Gastric Air Bubble (1 of 3)
Bloated Abdomen (2 of 3)

Non-bloated Abdomen (3 of 3)

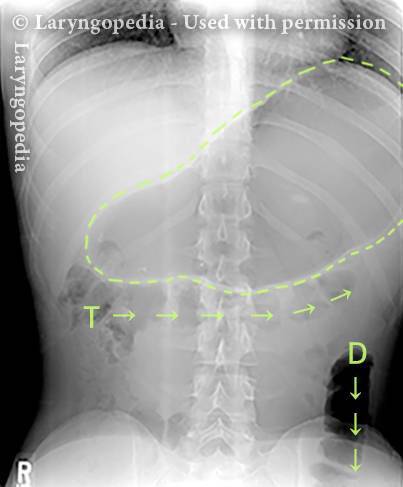
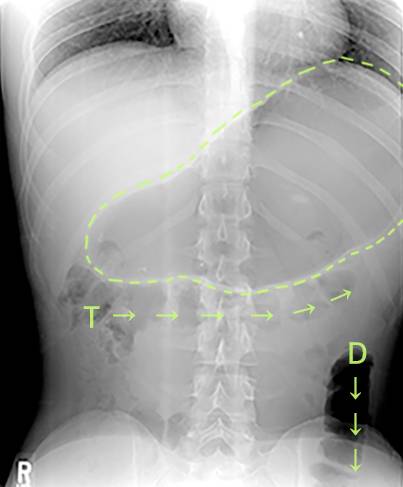
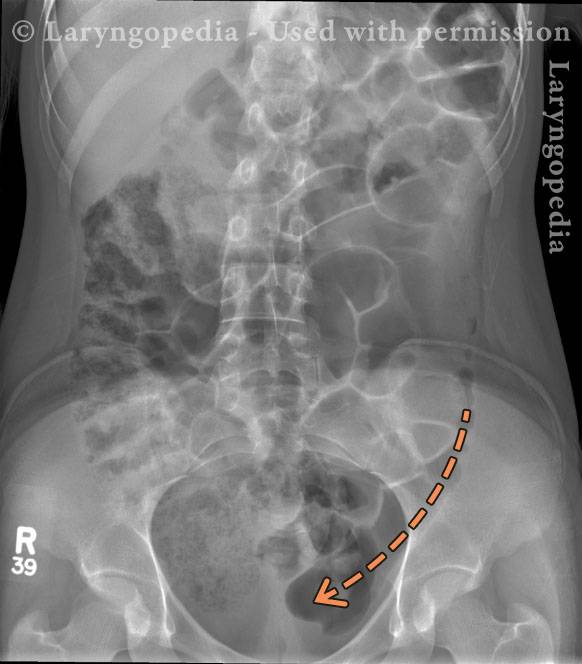
Another Example of Dramatic Gas Pattern of R-CPD that Could Be Mistaken for a Small Bowel Obstruction
This high school junior presented with classic symptoms of retrograde cricopharyngeus dysfunction (R-CPD). Her history included lifelong inability to burp — reportedly even as an infant — along with socially embarrassing gurgling sounds, chest pressure, and significant flatulence.
Prior to receiving the diagnosis of R-CPD, her evaluation was extensive and unrevealing, including chest radiography, abdominal films, 24-hour pH monitoring, upper endoscopy, and additional testing. Ultimately, the diagnosis was made clinically based on a strong syndromic match to the criteria codified by Bastian et al. (2019).
Treatment with botulinum toxin injection into the cricopharyngeus muscle successfully “taught her to burp,” with complete resolution of her symptoms.
The abdominal radiographs shown here were obtained during an acute exacerbation that prompted an emergency department visit — prior to diagnosis and treatment.
Importantly, the imaging findings did not trigger a diagnosis of small bowel obstruction. Several features argued against obstruction:
- Her abdominal distress had been a daily occurrence for years.
- There was no “smooth pipe” appearance of the bowel.
- No significant air–fluid levels were seen.
- Her primary complaint was severe pressure rather than colicky pain.
- There was no nausea or vomiting.
- She had no prior abdominal surgery.
- Bowel sounds were present.
- She continued to pass flatus.
In similar cases, patients may occasionally receive nasogastric decompression and, at times, a small enema to facilitate gas evacuation.
Extensive trapped air (1 of 2)
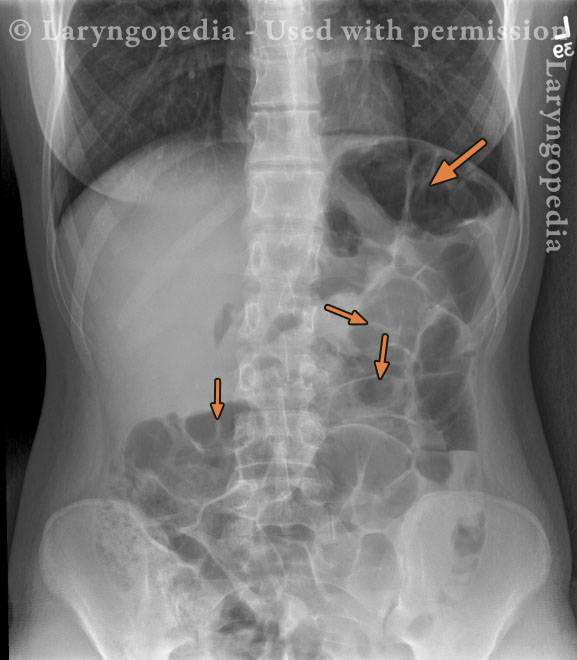
Intraluminal gas (2 of 2)
Abdominal Distention Caused by R-CPD
Bloating and abdominal distention before botox injection for inability to burp (1 of 2)

Resolved, one month after botox, with burping restored (2 of 2)

Can’t Burp: Progression of Bloating and Abdominal Distention – a Daily Cycle for Many with R-CPD
This young woman has classic R-CPD symptoms—the can’t burp syndrome. Early in the day, her symptoms are least, and abdomen at “baseline” because she has “deflated” via flatulence through the night.
In this series you see the difference in her abdominal distention between early and late in the day. The x-ray images show the remarkable amount of air retained that explains her bloating and distention. Her progression is quite typical; some with R-CPD distend even more than shown here especially after eating a large meal or consuming anything carbonated.
Side view of a bloated abdomen (1 of 6)

Front view (2 of 6)

Greater Distention (3 of 6)

Front view of a swollen belly (4 of 6)

X-ray of trapped air (5 of 6)
Side view (6 of 6)
The Daily Inflation-Deflation Cycle for R-CPD
Deflated Abdomen (1 of 4)

Bloated lateral view (2 of 4)

Deflated abdomen (3 of 4)

R-CPD distention (4 of 4)

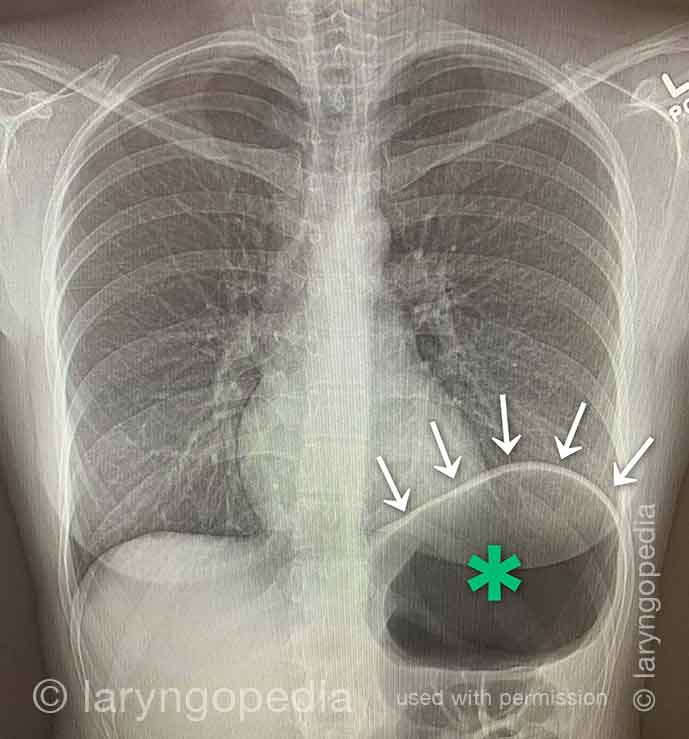
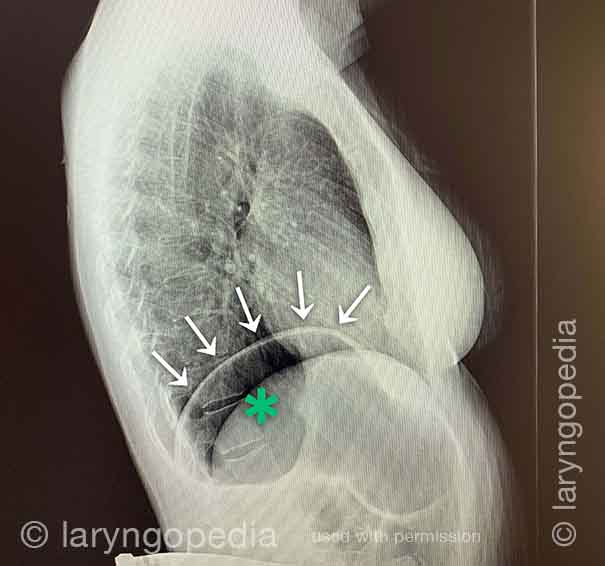
A Rare “abdominal crisis” Due to R-CPD (inability to burp)
This young man had an abdominal crisis related to R-CPD. He has had lifelong symptoms of classic R-CPD: inability to burp, gurgling, bloating, and flatulence. During a time of particular discomfort, he unfortunately took a “remedy” that was carbonated.
Here you see a massive stomach air bubble. A lot of his intestines are air-filled and pressed up and to his right (left of photo, at arrow). The internal pressure within his abdomen also shut off his ability to pass gas.
X-Ray of Abdominal Bloating (1 of 2)
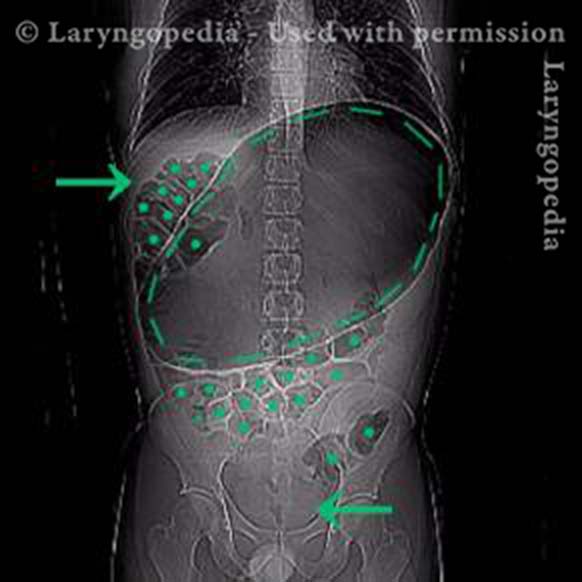
Original X-Ray (2 of 2)

Shortness of Breath Caused by No-Burp
Persons who can’t burp and have the full-blown R-CPD syndrome often say that when the bloating and distention are particularly bad—and especially when they have a sense of chest pressure, they also have a feeling of shortness of breath.
They’ll say, for example, “I’m a [singer, or runner, or cyclist or _____], but my ability is so diminished by R-CPD. If I’m competing or performing I can’t eat or drink for 6 hours beforehand.” Some even say that they can’t complete a yawn when symptoms are particularly bad. The x-rays below explain how inability to burp can cause shortness of breath.
X-ray of trapped air (1 of 2)
Side view (2 of 2)

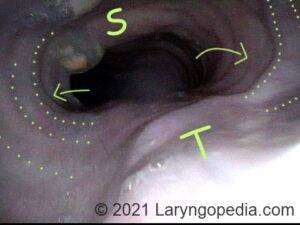
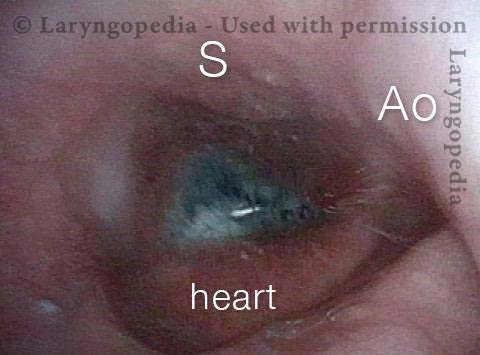
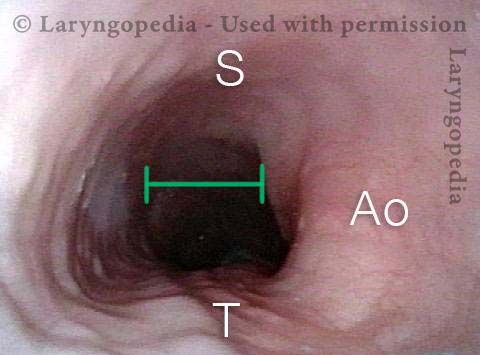
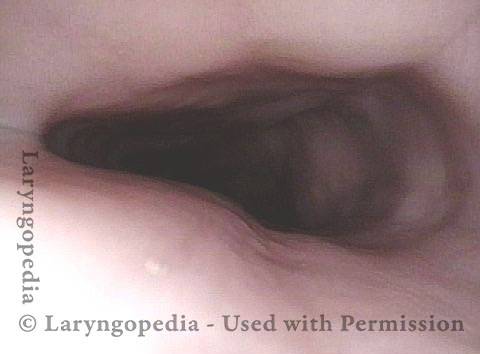
Esophageal Findings
The esophagus is typically collapsed around endoscopes inserted into them and air is pumped in through a tiny channel in order to gently expand the esophagus so that its walls can be seen. Here, the air the patient cannot belch/evacuate is doing that work for us. And the esophagus remains open for extended time, the full duration of the examination. See more photo essays…
Aortic shelf (1 of 3)
Bony spur emerges due to stretched esophagus (2 of 3)

Stretched esophagus due to unburpable air (3 of 3)
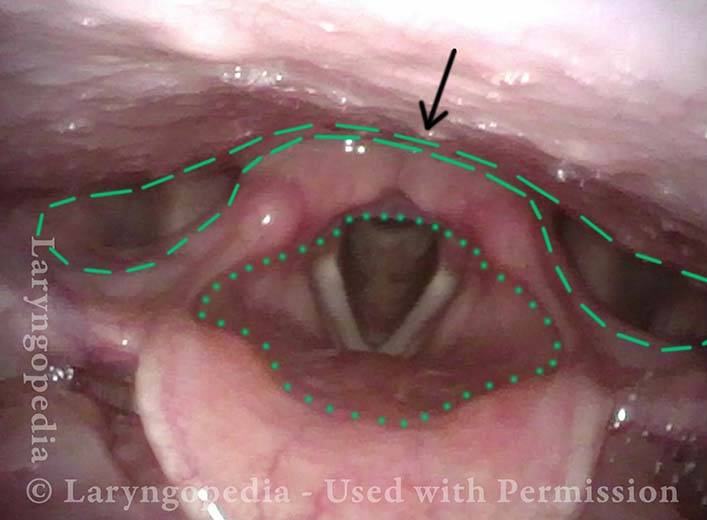
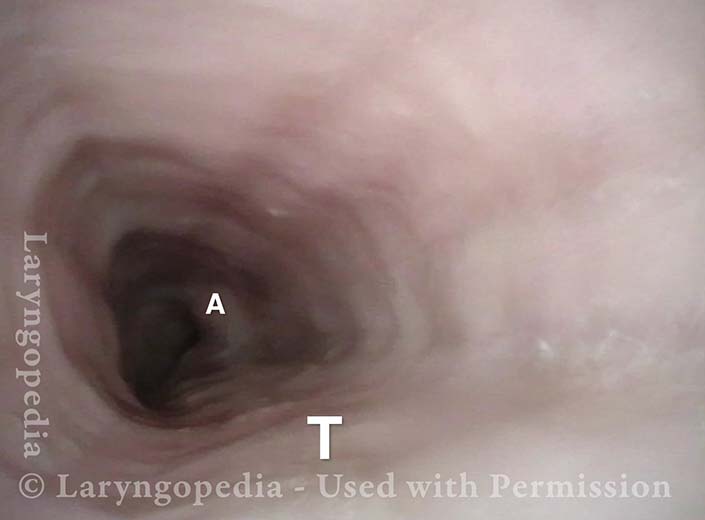
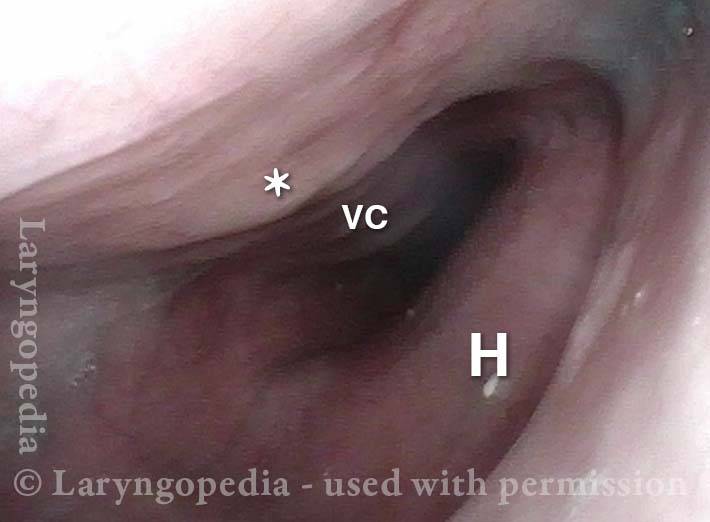
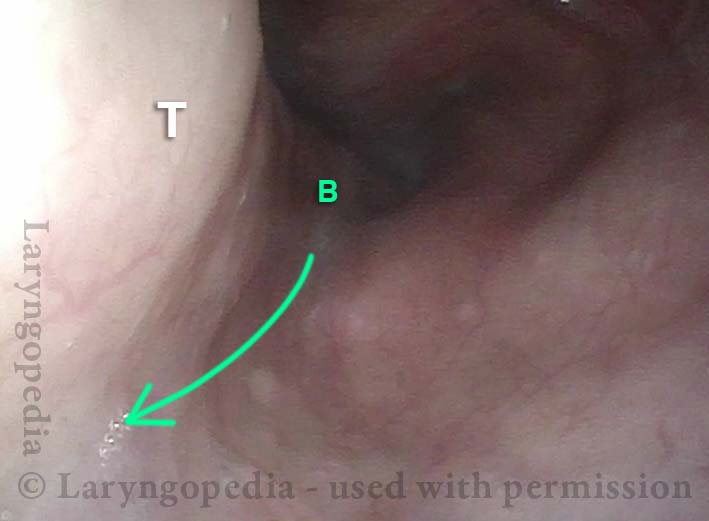
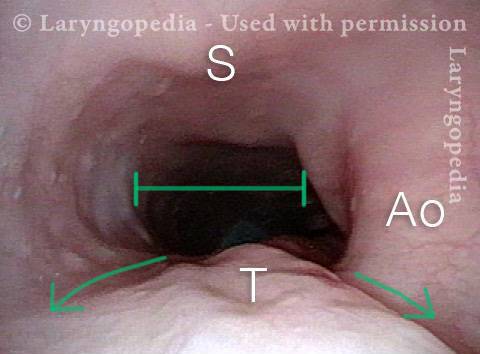
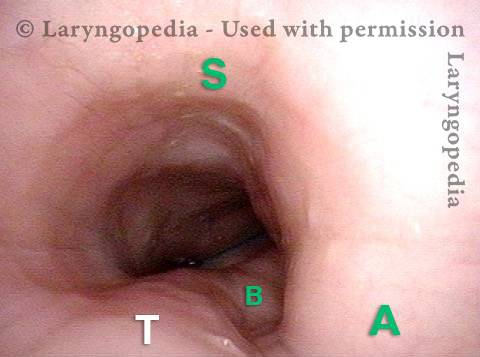
Airway, Foodway, Cricopharyngeus Muscle, and Esophagus in R-CPD
This young woman has never been able to burp normally. She experiences typical, severe R-CPD symptoms of daily bloating, loud gurgling noises, and excessive flatulence. Botulinum toxin injection of the cricopharyngeus muscle is planned to rid her of the syndrome of R-CPD in the short term, and to teach her how to burp “permanently” (even after the botulinum toxin has worn off).
Laryngopharynx (1 of 5)
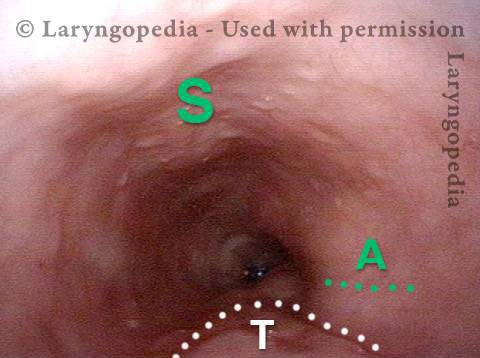
Esophageal opening (2 of 5)
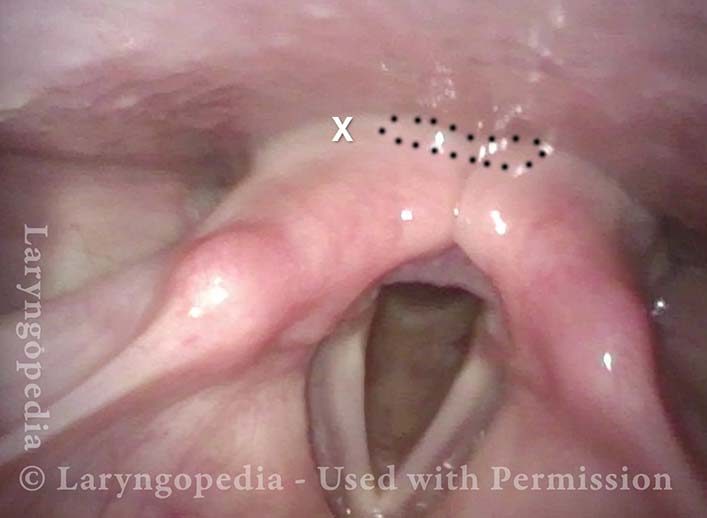
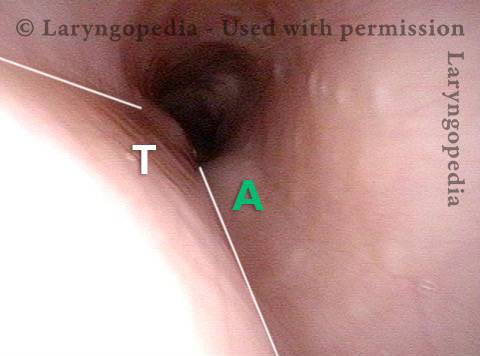
Ridge of UES (3 of 5)
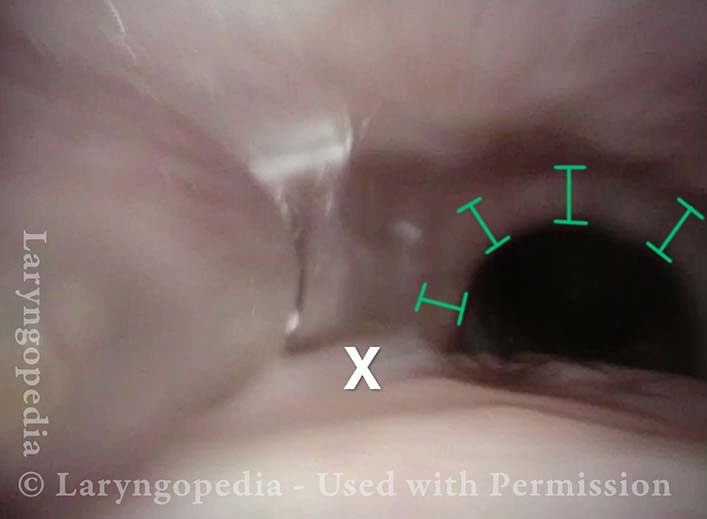
Ridge of UES (4 of 5)
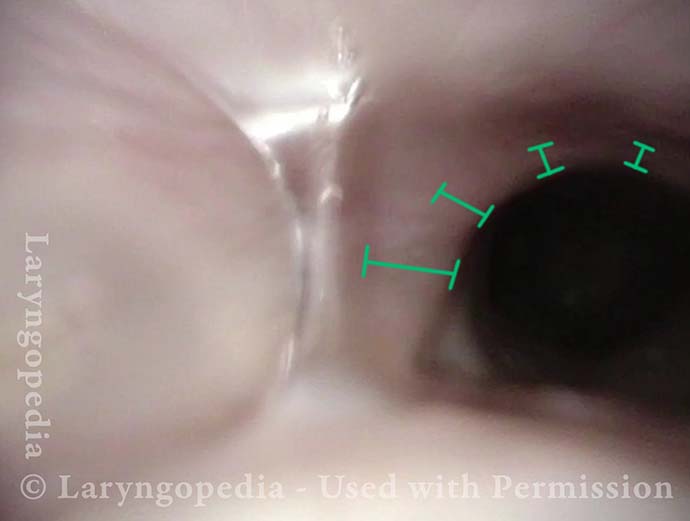
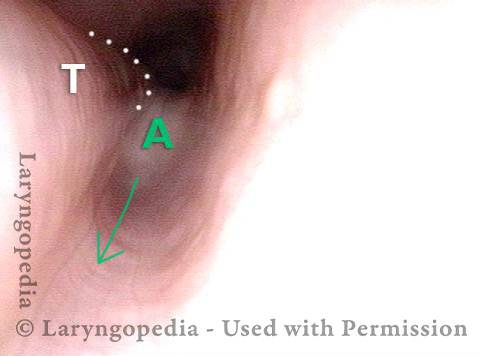
Distended Esophagus (5 of 5)
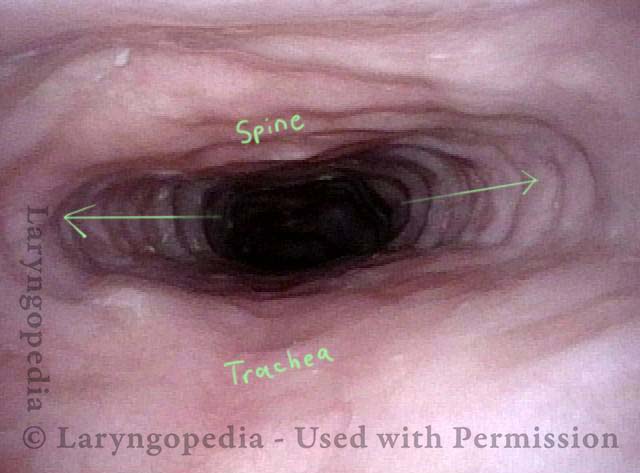
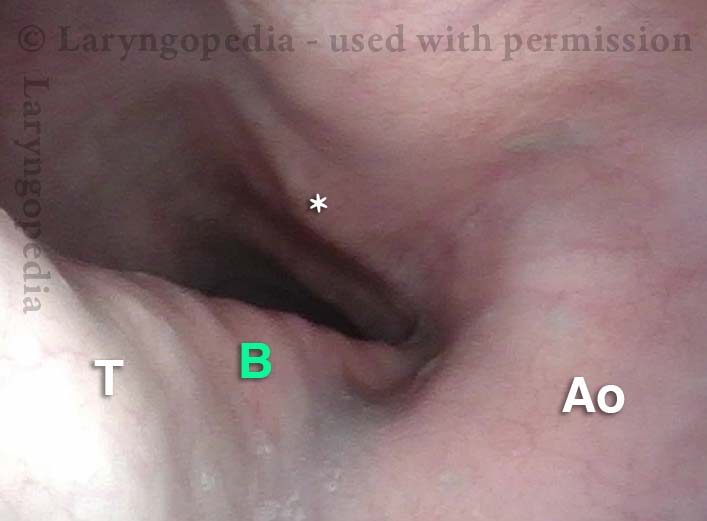
In R-CPD, Esophageal Findings May Correlate with Symptoms
This middle-aged patient has suffered all her life with inability to burp, and symptoms seem to be ever increasing. Currently, she has all 3 levels of pressure/bloating: abdomen, chest, and neck. Her abdomen often distends to “8 months pregnant” by end of day, and is flat in the morning after an evening/night of flatulence.
Abdominal symptoms are constant; when chest symptoms occur (pressure, etc.) they are even more uncomfortable. Her office upper esophagoscopy using a 3.7 mm ENT scope without air insufflation shows typical findings:
- The column of her own un-burped air, holding the esophagus in “always open” position all the way to the gastro-esophageal junction; tracheal mound, and aortic shelf.
- More than in most cases, the left mainstem bronchus is shown in high relief.
Distended upper esophagus (1 of 4)

Distended mid-esophagus (2 of 4)

Left-mainstem bronchus (3 of 4)
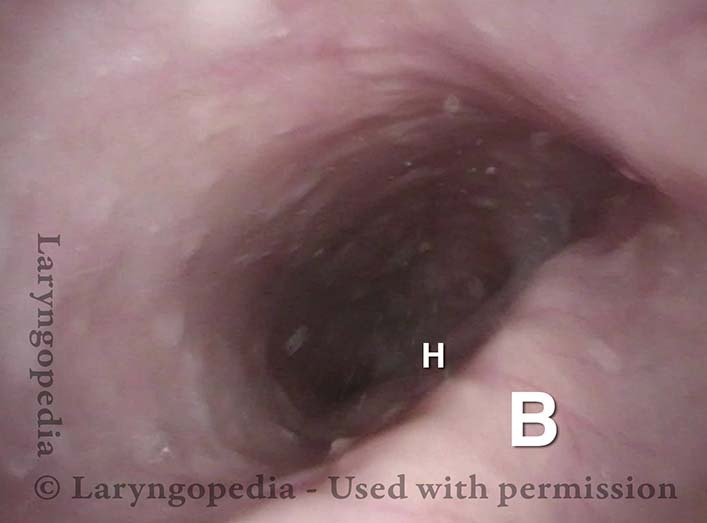
View includes open lower esophageal sphincter (4 of 4)

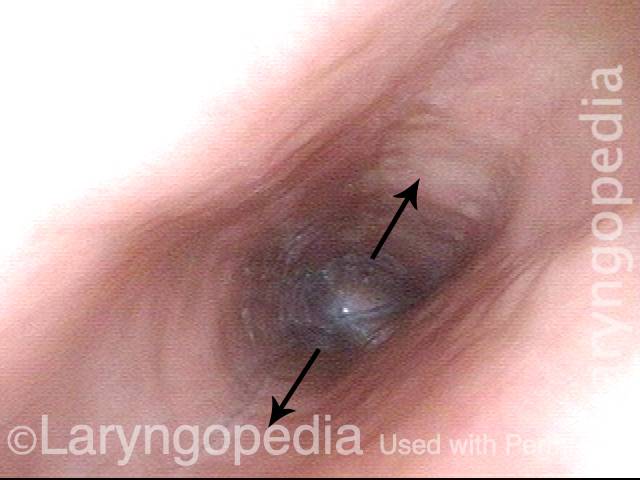
Dramatic esophageal dilation from R-CPD, even in a young person!
The central problem for persons with R-CPD is (obviously) the inability to burp. Bits of air travel through the upper esophageal sphincter (cricopharyngeus muscle) which closes behind each swallow.
Even as the air builds up, expanding the esophagus and sending increasing signals of the need to burp, the air is unable to “get back out” via burping. Initial discomfort from stuck burps-in-waiting may elicit reflexive “extra” swallows that only add more air that cannot be burped.
Gradually this dilates the esophagus (and eventually the stomach, and as air traverses the GI tract, the intestines all the way to the rectum, where it must be released as flatulence). Even in young people, esophageal dilation can be dramatic, causing chest discomfort.
The images below are from the office examination of a teenager sitting in the examination chair with a small ENT scope in his esophagus. The column of air he cannot burp up is holding the esophagus widely open. No air has been insufflated through the scope. The stretched esophagus throws structures outside it into high relief as seen below.
Stretched esophagus (1 of 3)
Mid-esophagus (2 of 3)
Stretching esophagus (3 of 3)
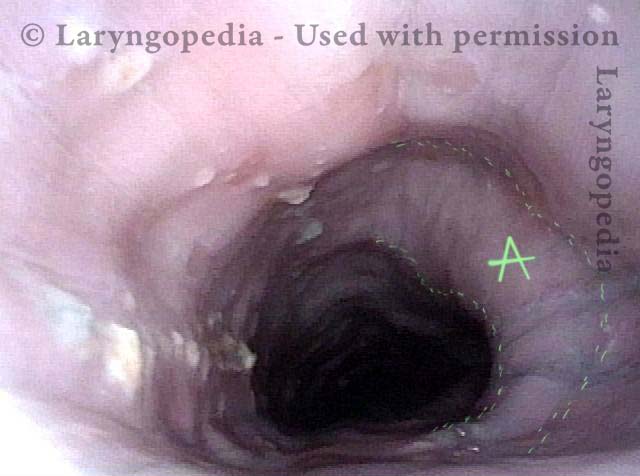
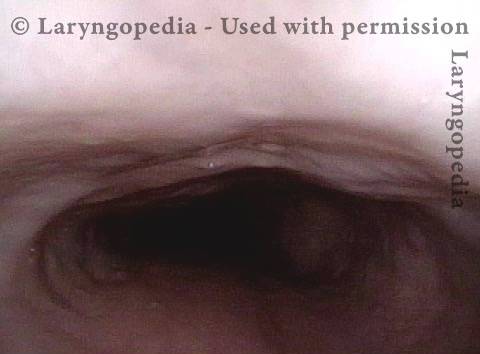
Esophageal Stretching by Unburpable Air in R-CPD
This young man has had the classic syndrome of R-CPD lifelong. His esophageal findings at the end of a videoendoscopic swallow study are classic. The esophagus is mostly a collapsed muscular tube in young people, yet his esophagus is widely open on a continuous basis due swallowed air that he cannot burp up.
Typical view of an esophagus (1 of 4)
Lower esophagus (2 of 4)
Stretched mid-esophagus (3 of 4)
Esophagus stretches laterally (4 of 4)
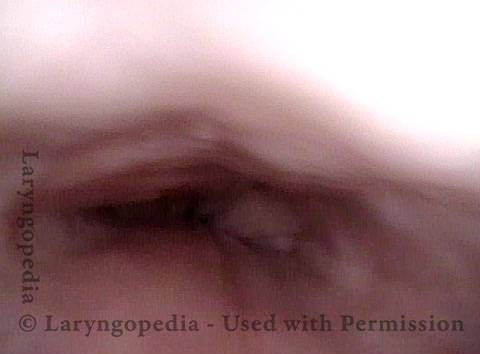
More Interesting Esophageal Findings of R-CPD (Inability to Burp)
Stretched Esophagus (1 of 4)
Tracheal Wall (2 of 4)
Over-dilation (3 of 4)
Bronchus is visible (4 of 4)
R-CPD and Esophageal Dilation
Posterior pharyngeal wall (1 of 3)
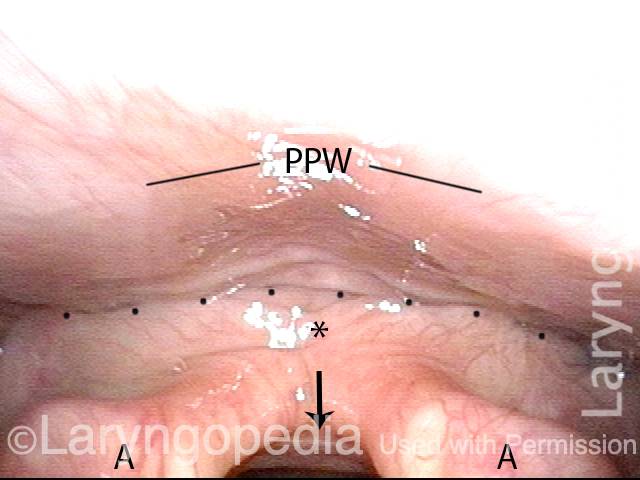
Is it R-CPD? (2 of 3)
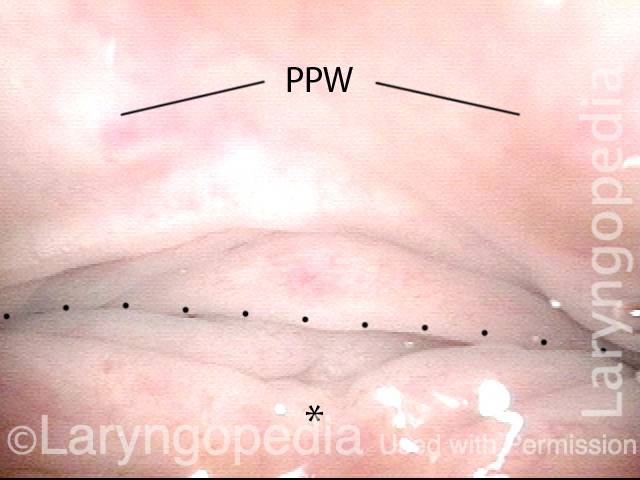
Stretched esophagus indicates R-CPD (3 of 3)
What the Esophagus Can Look Like “Below A Burp”
Baseline (1 of 3)
Pre-burp (2 of 3)
Post-burp (3 of 3)
![]()
Videos about R-CPD

![]()
Dr. Bastian’s Published R-CPD Articles
![]()
Additional R-CPD Resources







Sphincters
Made of Stronger Stuff
Gleeks & Gurgles
Reply All







No-Burp: It's not just you
(33,000+ no-burpers)

Retrograde Cricopharyngeus Dysfunction (R-CPD)
[6,500+ members]
I can now burp
@Lilamycox
My weird medical history
@Brittcurls
My R-CPD journey
Julie Anne Gay