
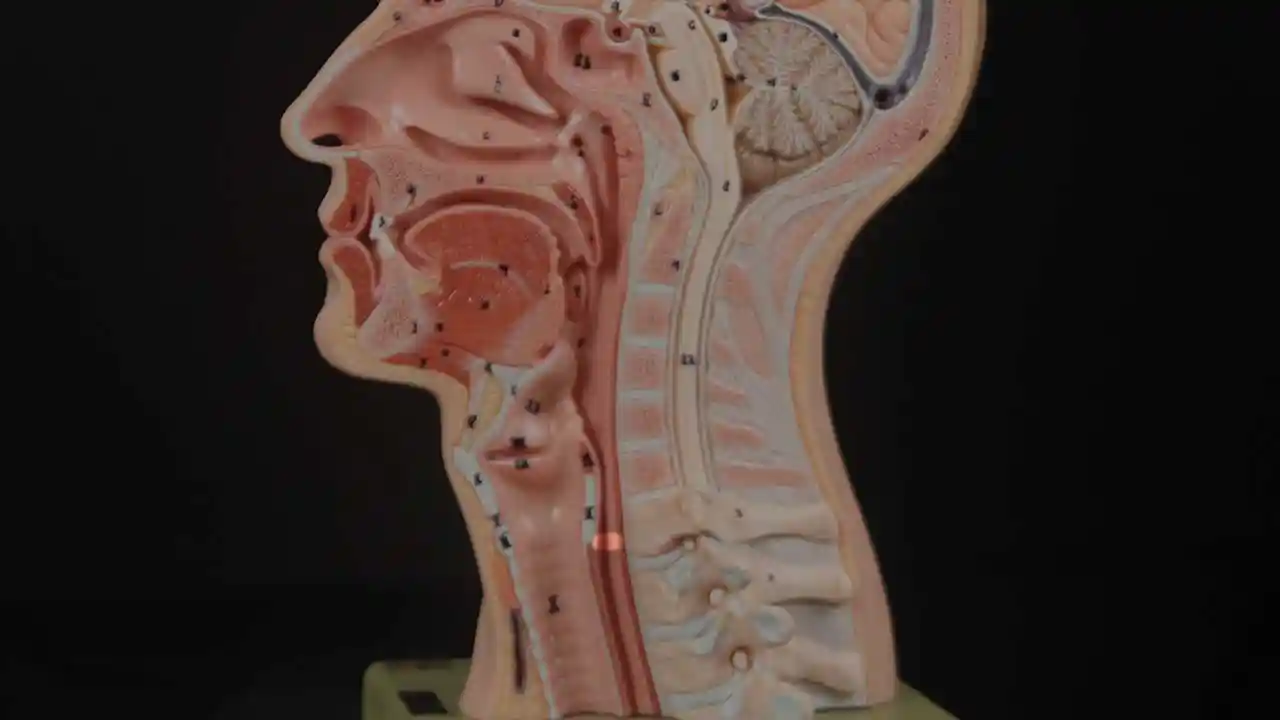
L’incapacità di ruttare o ruttare si verifica quando lo sfintere esofageo superiore (muscolo cricofaringeo) non può rilassarsi per rilasciare la “bolla” d’aria. Lo sfintere è una valvola muscolare che circonda l’estremità superiore dell’esofago appena sotto l’estremità inferiore del passaggio della gola. Se guardi dal davanti il collo di una persona, è appena sotto il “pomo di Adamo / Eva”, direttamente dietro la cartilagine cricoide.
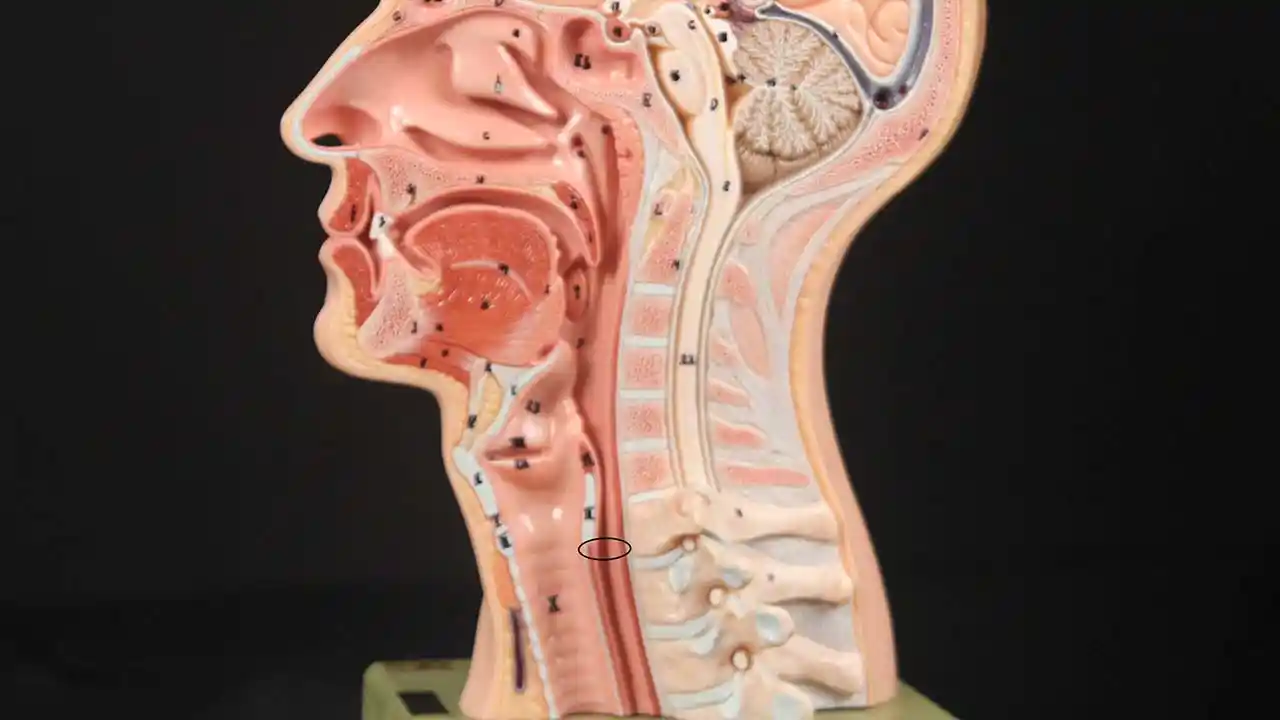
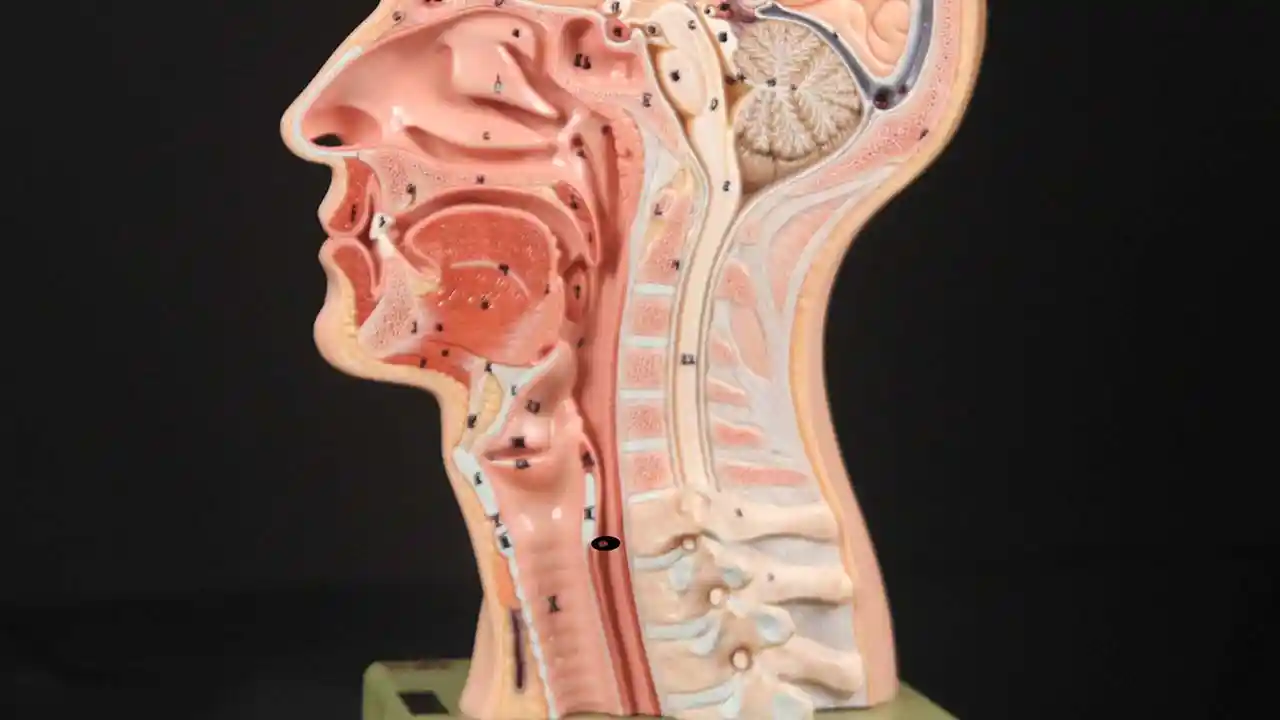
Se ti interessa vederlo su un modello, guarda la foto qui sotto. Quel muscolo dello sfintere si rilassa per circa un secondo ogni volta che ingeriamo saliva, cibo o bevande. Tutto il resto del tempo è contratto. Ogni volta che una persona rutta, lo stesso sfintere deve lasciarsi andare per una frazione di secondo affinché l’aria in eccesso possa fuoriuscire verso l’alto.
In altre parole, così come è necessario che lo sfintere “si lasci” per ammettere cibi e bevande verso il basso nel normale atto di deglutizione, è anche necessario che lo sfintere sia in grado di “lasciarsi andare” per liberare aria verso l’alto per l’eruttazione.
Cricopharyngeus Muscle (1 of 3)
Open Cricopharyngeus Muscle (2 of 3)
Closed (3 of 3)
Iniezione di Botox presso il Bastian Voice Institute
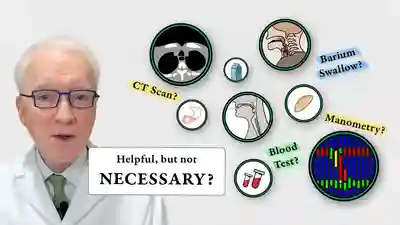
Per le persone che sperimentano questo problema fino al disagio e alla ridotta qualità della vita, ecco un approccio:
In primo luogo, uno studio videofluoroscopico della deglutizione, magari con granuli effervescenti. Ciò stabilisce che lo sfintere funziona normalmente in una direzione di deglutizione in avanti (anterograda), ma non in un modo inverso (retrogrado) di eruttazione o rigurgito. Insieme ai sintomi sopra descritti, questo stabilisce la diagnosi di disfunzione cricofaringea solo retrograda (non rilassamento).
In secondo luogo, una prova di trattamento per iniettare Botox nel muscolo sfintere malfunzionante. L’effetto desiderato del Botox nel muscolo è di indebolirlo per almeno diversi mesi. Permette a ua di verificare che il problema sia risolto o quantomeno minimizzato. (Guarda il video, Quali test sono necessari per l’R-CPD?)
L’iniezione di Botox potrebbe potenzialmente verificarsi in un ufficio, ma consigliamo la prima volta (almeno) con un’anestesia generale molto breve in una sala operatoria ambulatoriale. Questo risponde alla domanda: lo sfintere non è in grado di rilassarsi quando si presenta con una bolla d’aria dal basso? È importante rispondere alla domanda in modo definitivo al primo tentativo per vedere se è il problema di fondo
Sollevamento del CPM per un’iniezione R-CPD
Queste sono le foto intraoperatorie di una delle quasi 1500 persone trattate per R-CPD a settembre 2023. Questa sequenza mostra diverse cose:
- L’esofago dilatato, “sempre aperto” distalmente (sotto) al muscolo;
- Come identificare il muscolo cricofaringeo;
- E un modo per iniettarlo.
Above the CPM (1 of 5)

Ridge of the CPM (2 of 5)

Exposed CPM ( 3 of 5)

CPM Palpated ( 4 of 5)

Botox injection ( 5 of 5)

Cosa aspettarsi dopo la procedura Botox?
Consulta la voce del diario pubblicata dal Dr. Bastian per una spiegazione completa, ma in poche parole:
- Non ci sarà alcun sollievo dai sintomi dell’R-CPD per 1-5 giorni.
- Solo quando iniziano i microrutti i pazienti iniziano a notare l’inizio del sollievo dai sintomi. Quindi non provare la carbonatazione a pranzo il giorno dell’iniezione!
- Gli effetti collaterali iniziali del Botox possono essere “strani” per alcuni giorni o settimane.
- Se riesci a manipolare i tuoi gorgoglio prima del trattamento con Botox, per renderli più morbidi o più forti, usa questa tecnica per vedere se riesci ad affrettare i rutti o ad ingrandirli.
Per alcuni mesi almeno, i pazienti dovrebbero provare un notevole sollievo dai loro sintomi. E, le prime esperienze suggeriscono che potrebbe essere che questa singola iniezione di Botox permetta al sistema di “reimpostarsi” e la persona potrebbe non perdere mai la sua capacità di ruttare.
Naturalmente, se il problema si ripresenta, l’individuo potrebbe scegliere di perseguire ulteriori trattamenti di Botox o, in un caso veramente grave, potrebbe anche scegliere di sottoporsi a miotomia cricofaringea laser endoscopica.
Saggi fotografici dei nostri pazienti con R-CPD
R-CPD, Aerofagia ed Eruttazione
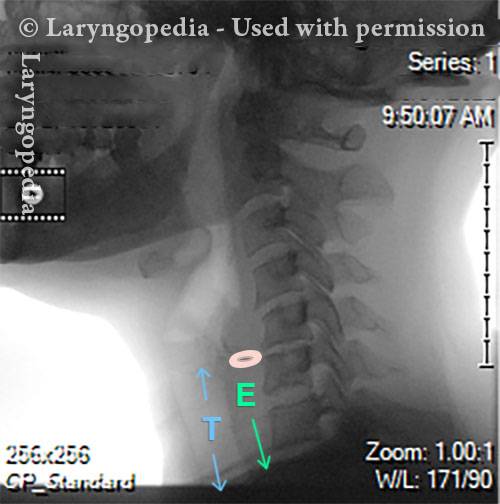
Questa radiografia laterale del collo fa parte di uno studio sulla deglutizione e illustra come l’aria può accumularsi e necessita di essere eruttata. Il focus di questo post è l’esofago, o “via alimentare”, che collega la parte inferiore della gola allo stomaco. L’esofago è un tubo muscolare che rimane per lo più collassato, chiuso, tranne quando lo attraversa il cibo, i liquidi o la saliva.
X-Ray of Larynx (1 of 6)
Barium swallow (2 of 6)

Collapsed esophagus (3 of 6)

Air is swallowed (4 of 6)
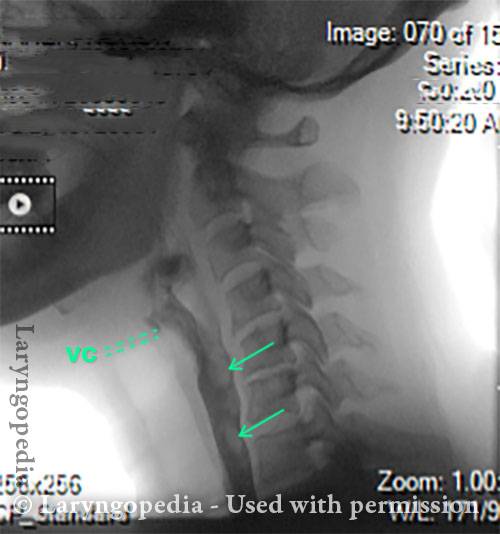
UES refuses to open for a burp (5 of 6)

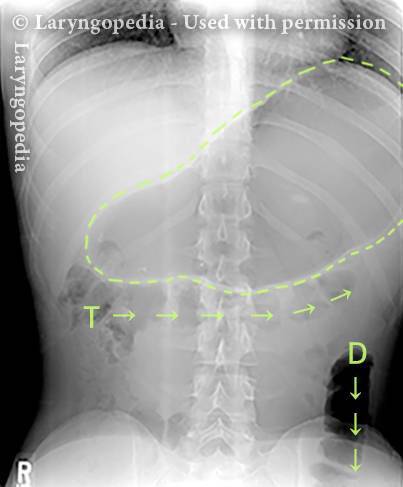
Abdominal Distention from R-CPD (6 of 6)
Distensione addominale di R-CPD
Gastric Air Bubble (1 of 3)
Bloated Abdomen (2 of 3)

Non-bloated Abdomen (3 of 3)

Il ciclo giornaliero di inflazione-deflazione per R-CPD
Deflated Abdomen (1 of 4)

Bloated lateral view (2 of 4)
Deflated abdomen (3 of 4)

R-CPD distention (4 of 4)

Progressione di gonfiore e distensione addominale: un ciclo quotidiano per molti con R-CPD
Questa giovane donna ha i classici sintomi di R-CPD: la sindrome del non poter ruttare. All’inizio della giornata, i suoi sintomi sono minimi e l’addome al “riferimento” perché si è “sgonfiata” a causa della flatulenza durante la notte. In questa serie si vede la differenza nella sua distensione addominale tra l’inizio e la fine della giornata.
Le immagini ai raggi X mostrano la notevole quantità di aria trattenuta che spiega il suo gonfiore e distensione. La sua progressione è abbastanza tipica; alcuni con R-CPD si distendono anche più di quanto mostrato qui, specialmente dopo aver consumato un pasto abbondante o aver consumato qualcosa di gassato.
Side view of a bloated abdomen (1 of 6)

Front view (2 of 6)

Greater Distention (3 of 6)

Front view of bloating stomach (4 of 6)

X-ray of trapped air (5 of 6)
Side view (6 of 6)
Distensione addominale causata da R-CPD
Quest’uomo sulla sessantina ha sopportato la miseria dell’R-CPD per tutta la vita. I suoi sintomi di incapacità di ruttare, gorgoglio, gonfiore, flatulenza (e altro) sono notevolmente alleviati dopo che la tossina botulinica nel suo muscolo cricofaringeo (sfintere esofageo superiore). Qui, vediamo anche la differenza prima e dopo nella sua distensione addominale.
Bloating and abdominal distention before botox injection for inability to burp (1 of 2)

Resolved, one month after botox, with burping restored (2 of 2)

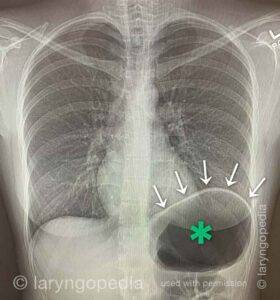
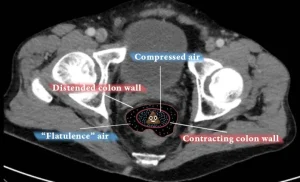
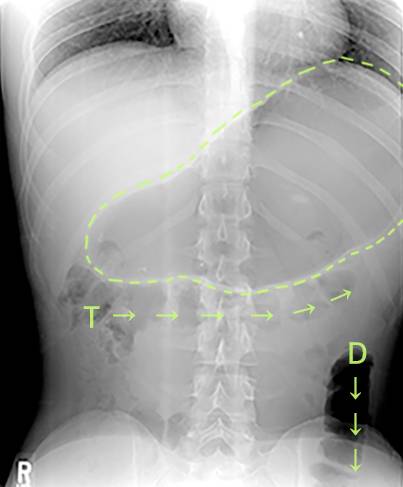
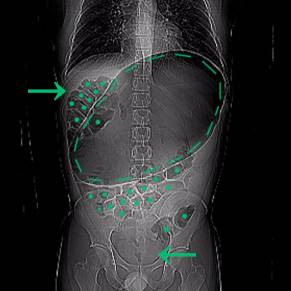
Una rara “crisi addominale” dovuta a R-CPD (incapacità di ruttare)
Questo giovane ha avuto una crisi addominale correlata alla R-CPD. Ha avuto sintomi per tutta la vita del classico R-CPD: incapacità di ruttare, gorgoglio, gonfiore e flatulenza. In un momento di particolare disagio, purtroppo ha preso un “rimedio” che era gassato.
Qui vedi un’enorme bolla d’aria nello stomaco. Molti dei suoi intestini sono pieni d’aria e pressati verso l’alto e alla sua destra (a sinistra della foto, in corrispondenza della freccia). La pressione interna all’addome ha anche interrotto la sua capacità di far passare il gas.
X-Ray of Abdominal Bloating (1 of 2)
Original X-Ray (2 of 2)

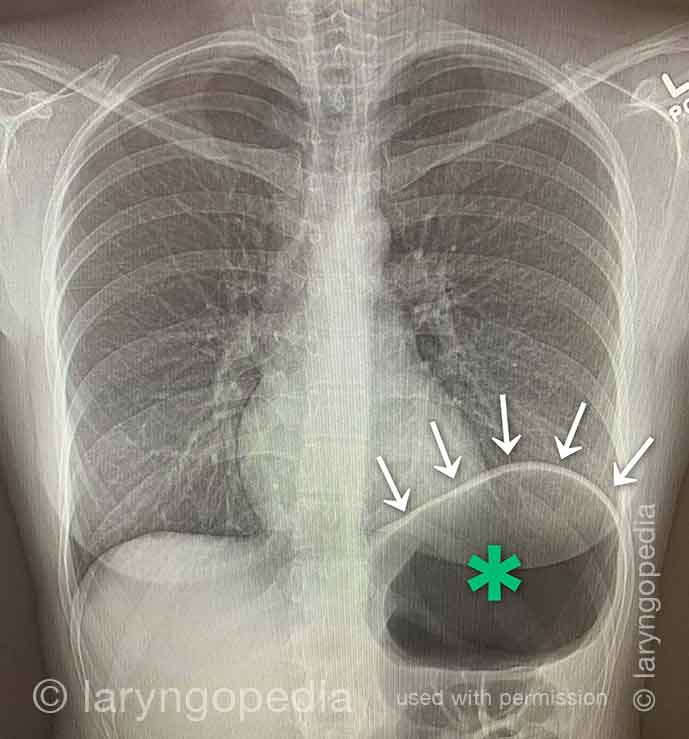
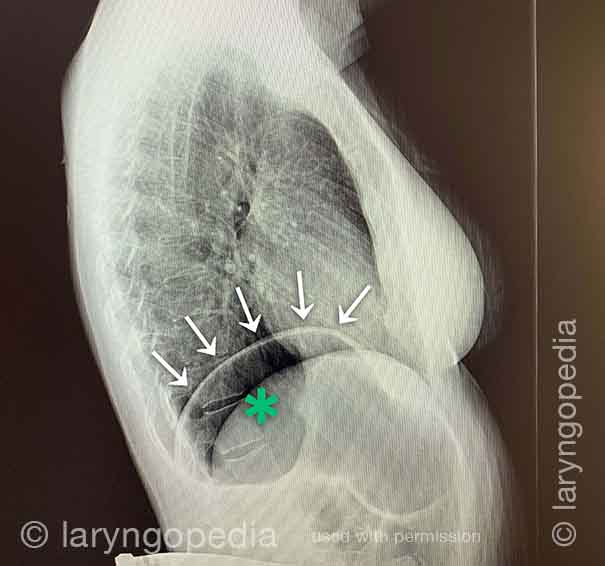
Mancanza di respiro causata da No-Burp
Le persone che non possono ruttare e hanno la sindrome R-CPD conclamata spesso dicono che quando il gonfiore e la distensione sono particolarmente gravi, e specialmente quando hanno un senso di pressione al torace, hanno anche una sensazione di mancanza di respiro. Diranno, ad esempio, “Sono un [cantante, o corridore, o ciclista o _____], ma la mia capacità è così ridotta da R-CPD. Se sto gareggiando o esibendomi, non posso mangiare o bere per 6 ore prima. Alcuni dicono addirittura che non possono completare uno sbadiglio quando i sintomi sono particolarmente gravi. I raggi X qui sotto spiegano come l’incapacità di ruttare può causare mancanza di respiro.
X-ray of trapped air (1 of 2)
Side view (2 of 2)
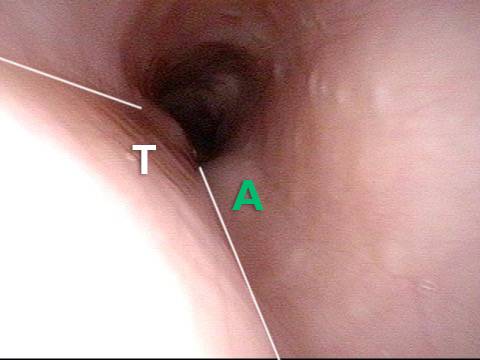
Reperti esofagei
Aortic shelf (1 of 3)
Bony spur emerges due to stretched esophagus (2 of 3)

Stretched esophagus due to unburpable air (3 of 3)
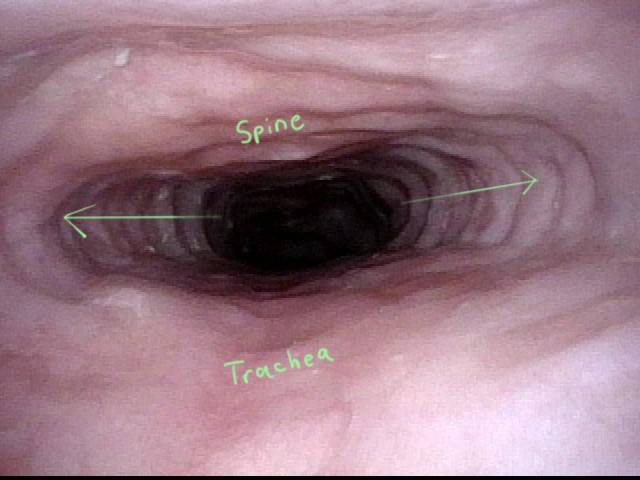
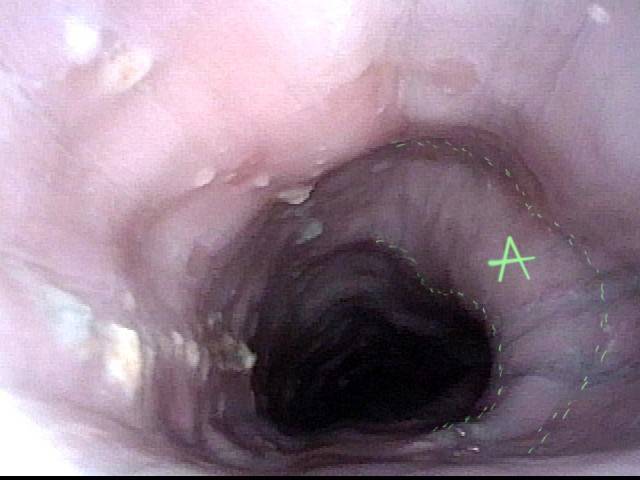
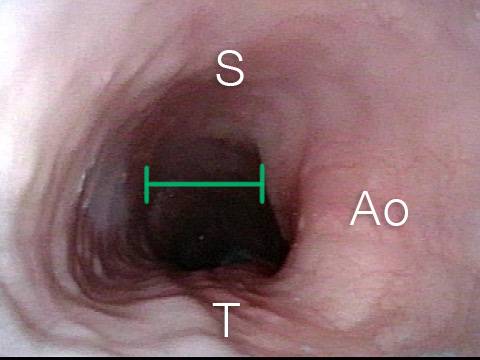
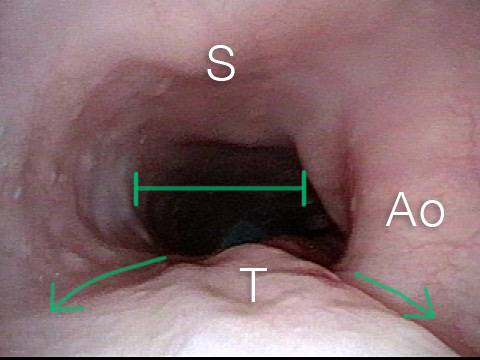
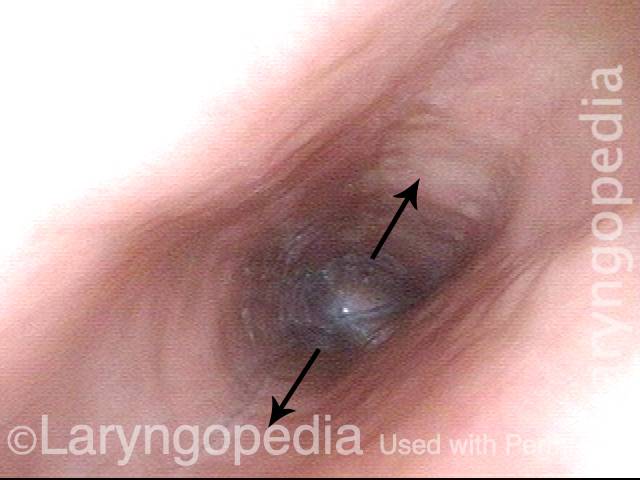
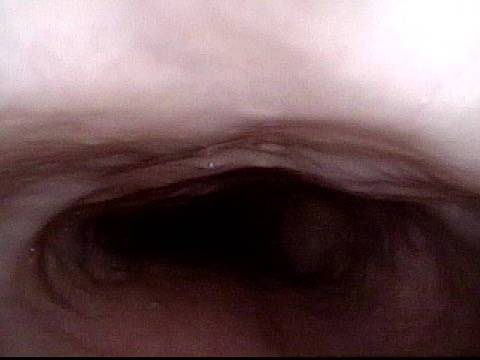
Allungamento esofageo mediante aria non eruttabile in R-CPD
Questo giovane ha avuto la classica sindrome di R-CPD per tutta la vita. I suoi reperti esofagei alla fine di uno studio videoendoscopico sulla deglutizione sono classici. L’esofago è per lo più un tubo muscolare collassato nei giovani, ma il suo esofago è ampiamente aperto su base continua a causa dell’aria inghiottita che non può ruttare.
Typical view of an esophagus (1 of 4)

Lower esophagus (2 of 4)
Stretched mid-esophagus (3 of 4)
Esophagus stretches laterally (4 of 4)
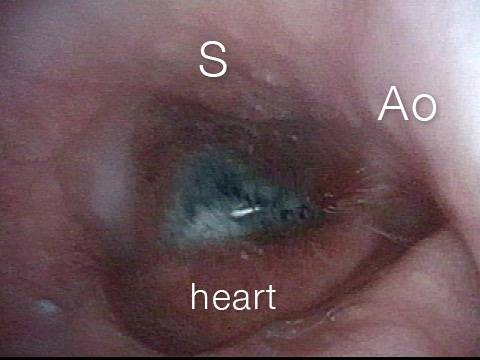
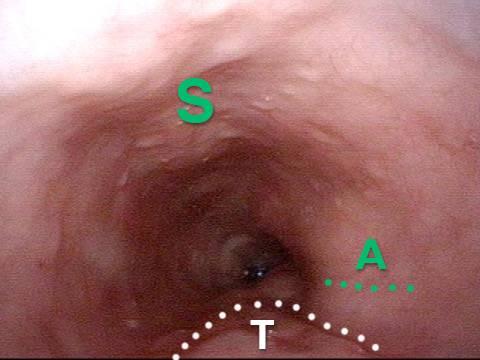
Risultati esofagei più interessanti di R-CPD (incapacità di ruttare)
Stretched Esophagus (1 of 4)
Tracheal Wall (2 of 4)
Over-dilation (3 of 4)
Bronchus (4 of 4)
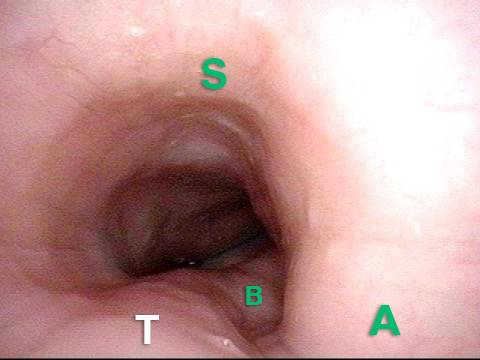
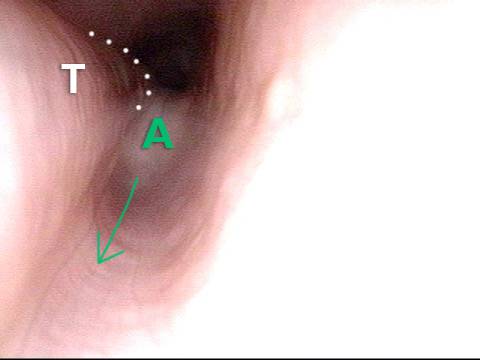
R-CPD e dilatazione esofagea
Posterior pharyngeal wall (1 of 3)
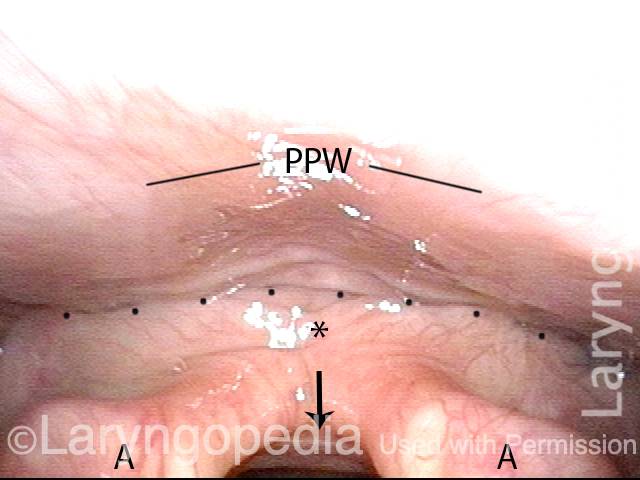
Is it R-CPD? (2 of 3)
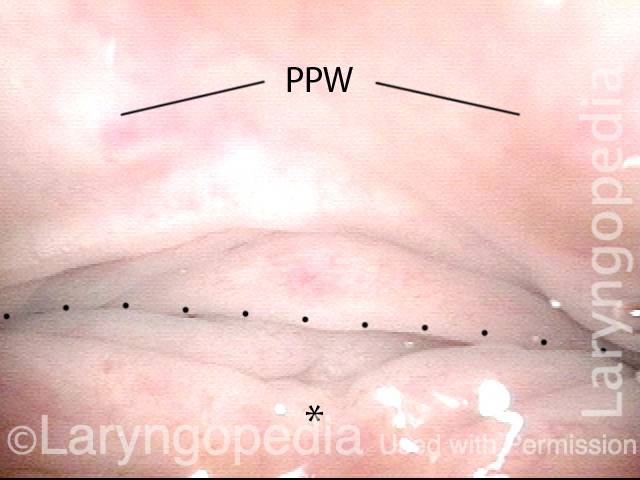
Stretched esophagus indicates R-CPD (3 of 3)
Come può apparire l’esofago “sotto un rutto”
Baseline (1 of 3)

Pre-burp (2 of 3)
Post-burp (3 of 3)

Video sull’R-CPD












(23,000+ no-burpers)

[2,200+ members]
@Lilamycox
@Brittcurls
Julie Anne Gay