![]()
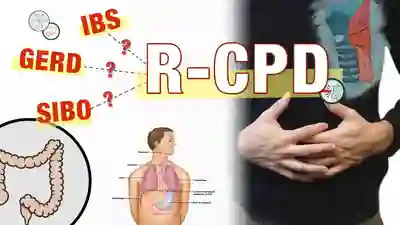
O que é DCF-R (incapacidade de arrotar, sem arrotar)?
Os 4 principais sintomas do DCF-R


![]()
Sintomas menos comuns de DCF-R
O que causa o DCF-R?
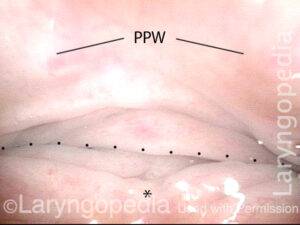
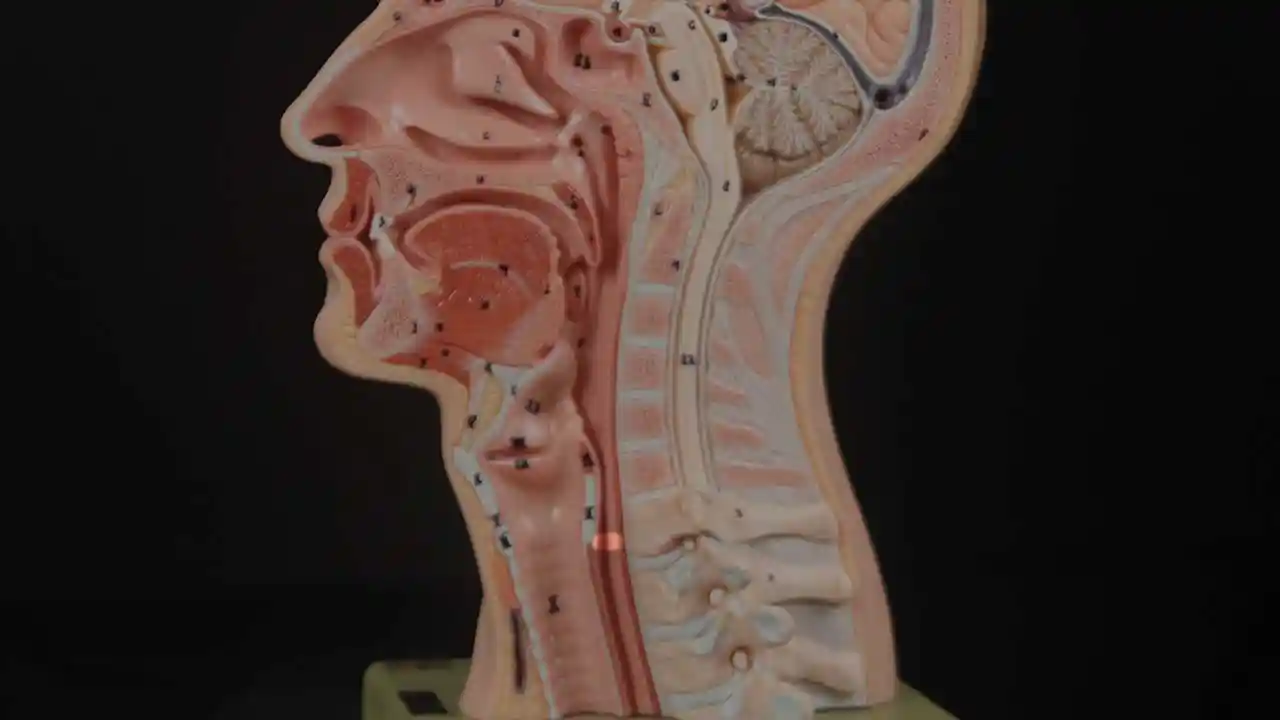
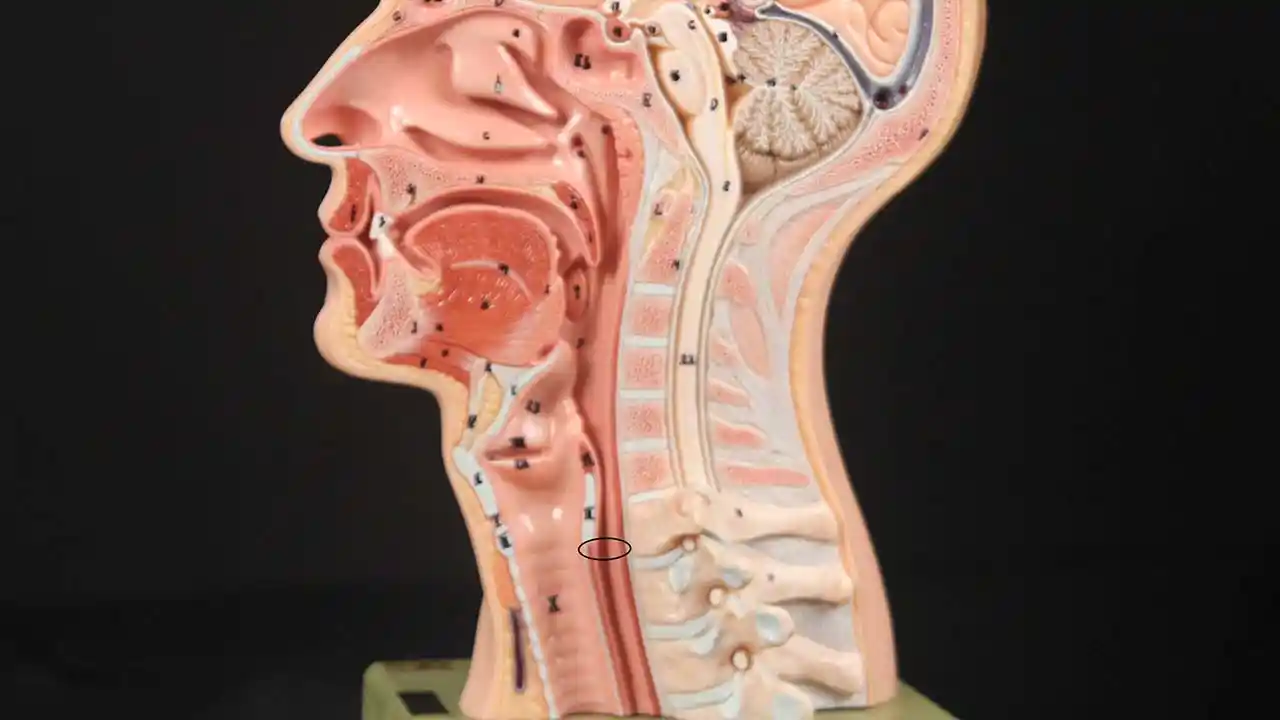
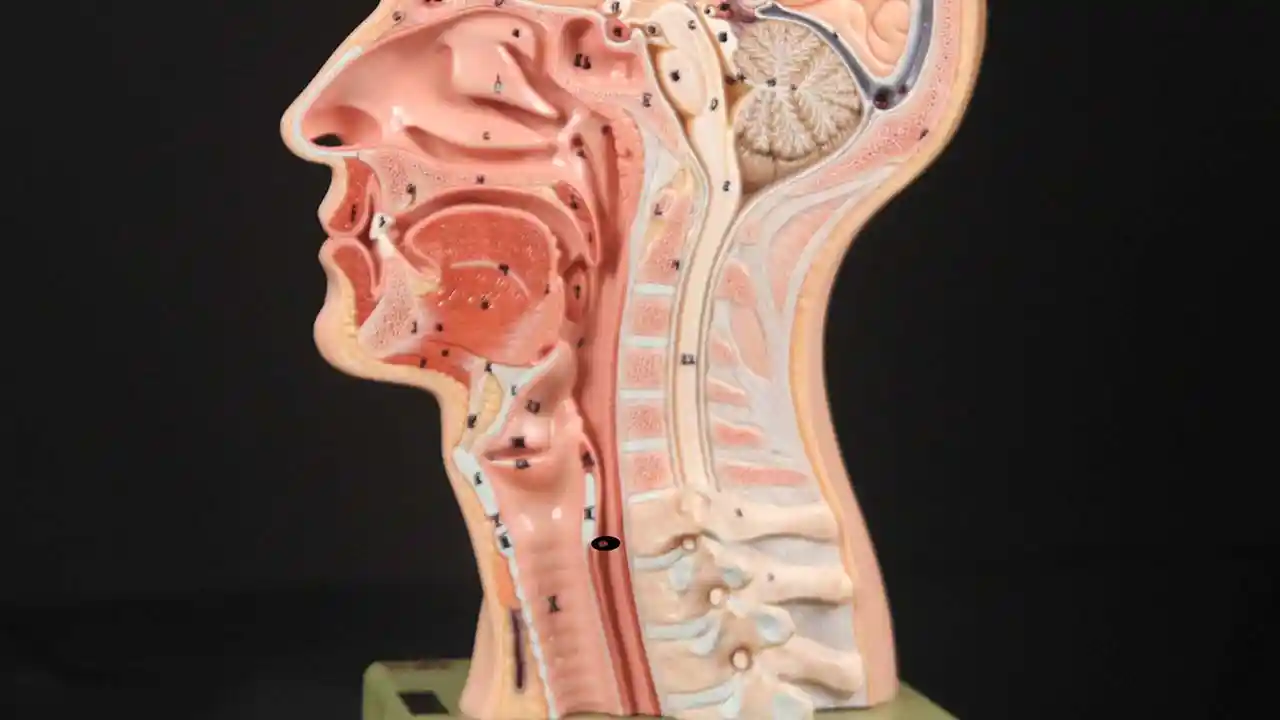
A incapacidade de arrotar ou arrotar ocorre quando o esfíncter esofágico superior (músculo cricofaríngeo) não consegue relaxar para liberar a “bolha” de ar. O esfíncter é uma válvula muscular que circunda a extremidade superior do esôfago, logo abaixo da extremidade inferior da passagem da garganta. Se olharmos de frente para o pescoço de uma pessoa, ele está logo abaixo do “pomo de Adão/Eva”, diretamente atrás da cartilagem cricóide.
Se você quiser ver isso em uma modelo, veja as fotos abaixo. O músculo esfincteriano relaxa por cerca de um segundo toda vez que engolimos saliva, comida ou bebida. Todo o resto do tempo é contratado. Sempre que uma pessoa arrota, o mesmo esfíncter precisa se soltar por uma fração de segundo para que o excesso de ar escape para cima.
Em outras palavras, assim como é necessário que o esfíncter “solte-se” para admitir comida e bebida para baixo no ato normal de engolir, também é necessário que o esfíncter seja capaz de “soltar-se” para liberar ar para cima para arrotar.
Cricopharyngeus Muscle (1 of 3)
Open Cricopharyngeus Muscle (2 of 3)
Closed (3 of 3)
![]()
Tratamento para DCF-R
Injeção de Botox no Bastian Voice Institute
Para pessoas que vivenciam esse problema a ponto de causar desconforto e redução da qualidade de vida, aqui está uma abordagem:
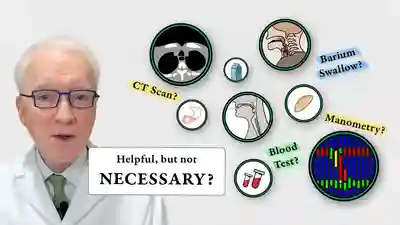
Primeiro, um estudo videofluoroscópico da deglutição, talvez com grânulos efervescentes. Isso estabelece que o esfíncter funciona normalmente na direção da deglutição para frente (anterógrada), mas não na direção reversa (retrógrada) de arrotos ou regurgitações. Juntamente com os sintomas descritos acima, isto estabelece o diagnóstico de disfunção cricofaríngea apenas retrógrada (não relaxamento).
Em segundo lugar, um ensaio de tratamento envolvendo a colocação de Botox no músculo esfincteriano com defeito. O efeito desejado do Botox no músculo é enfraquecê-lo durante pelo menos vários meses. A pessoa tem assim muitas semanas para verificar se o problema está resolvido ou pelo menos minimizado. (Veja o vídeo, Quais testes são necessários para DCF-R?)
A injeção de Botox poderia potencialmente ser feita em um consultório, mas recomendamos a primeira vez (pelo menos) aplicá-la durante uma breve anestesia geral em uma sala de cirurgia ambulatorial. Isso porque na primeira vez é importante responder à pergunta de forma definitiva, ou seja, que o problema é a incapacidade do esfíncter de relaxar quando se depara com uma bolha de ar vinda de baixo.
Aumentando o CPM para uma injeção DCF-R
Estas são fotos intraoperatórias de uma das quase 1.700 pessoas tratadas para DCF-R em março de 2024. Esta sequência mostra várias coisas:
- O esôfago dilatado e “sempre aberto” distal (abaixo) do músculo
- Como identificar o músculo cricofaríngeo
- Uma maneira de injetar o músculo.
Above the CPM (1 of 5)

Ridge of the CPM (2 of 5)

Exposed CPM ( 3 of 5)

CPM Palpated ( 4 of 5)

Botox injection ( 5 of 5)

O que esperar após o procedimento de Botox?
Revise a entrada publicada no Diário do Dr. Bastian para obter uma explicação completa, mas em poucas palavras:
- Não haverá alívio dos sintomas de DCF-R por 1 a 5 dias.
- Somente quando começam os microarrotos é que os pacientes começam a notar o início do alívio dos sintomas. Portanto, não experimente carbonatação no almoço no dia da injeção!
- Os efeitos colaterais iniciais do Botox podem ser “estranhos” por alguns dias ou semanas.
- Se você puder manipular seus gorgolejos antes do tratamento com Botox, para torná-los mais suaves ou mais altos, use essa técnica para ver se consegue apressar os arrotos ou torná-los maiores.
Durante alguns meses, pelo menos, os pacientes devem experimentar um alívio dramático dos sintomas. E a experiência inicial sugere que pode ser que esta única injeção de Botox permita que o sistema seja “reiniciado” e a pessoa nunca perca a capacidade de arrotar. É claro que, se o problema retornar, o indivíduo poderá optar por realizar tratamentos adicionais com Botox ou, em um caso realmente grave, poderá até mesmo optar por se submeter à miotomia endoscópica do cricofaríngeo a laser.
![]()
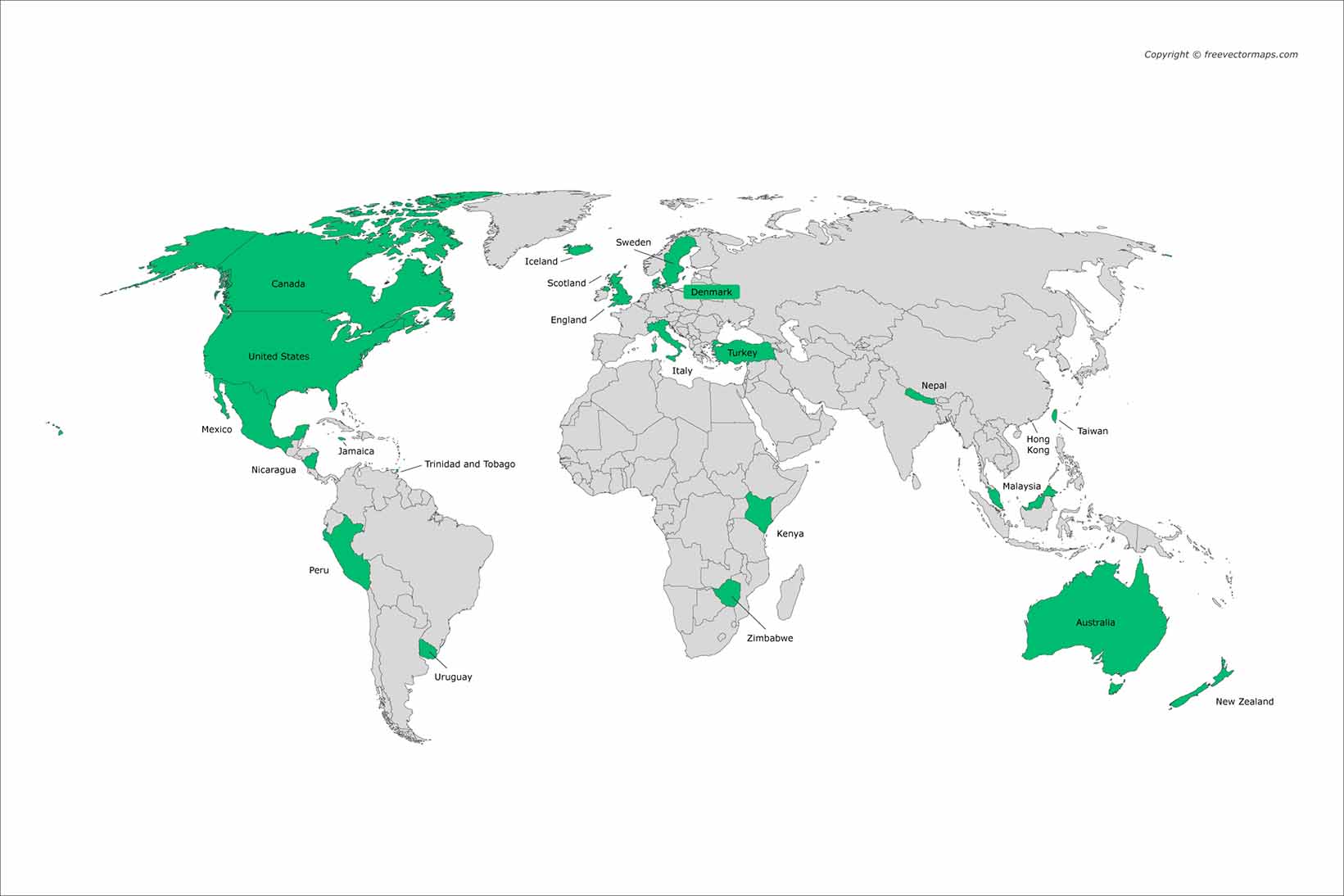
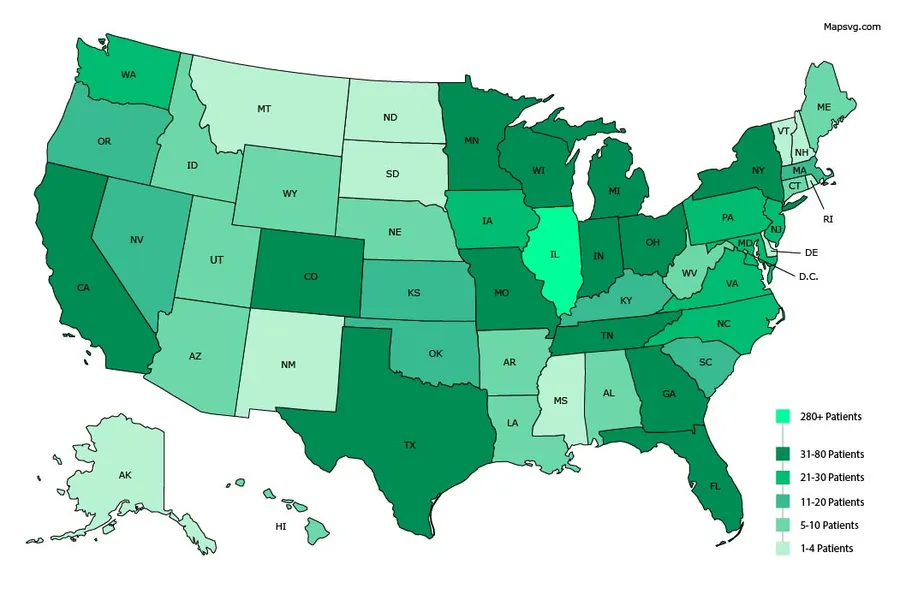
De onde vêm nossos pacientes DCF-R?
![]()
Ensaios fotográficos de pacientes DCF-R
DCF-R, Aerofagia e Arrotar
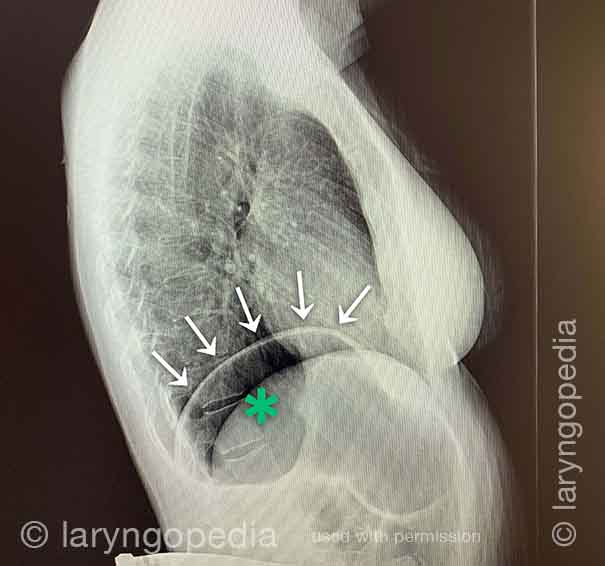
Esta radiografia lateral do pescoço faz parte de um estudo de deglutição e ilustra como o ar pode se acumular e precisar ser expelido. O foco desta postagem é o esôfago, ou “via alimentar”, que conecta a parte inferior da garganta ao estômago. O esôfago é um tubo muscular que permanece quase sempre colapsado – fechado – exceto quando alimentos, líquidos ou saliva o atravessam.
X-Ray of Larynx (1 of 6)
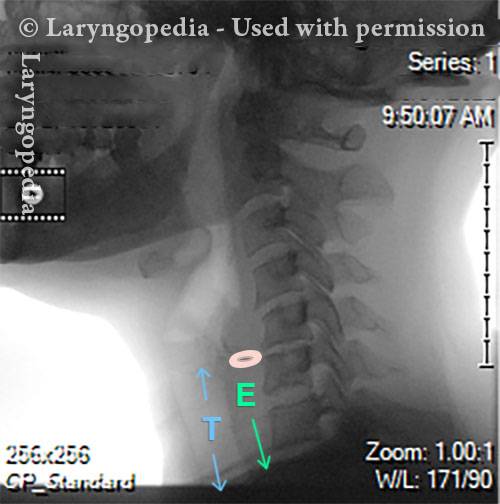
Barium swallow (2 of 6)

Collapsed esophagus (3 of 6)

Air is swallowed (4 of 6)
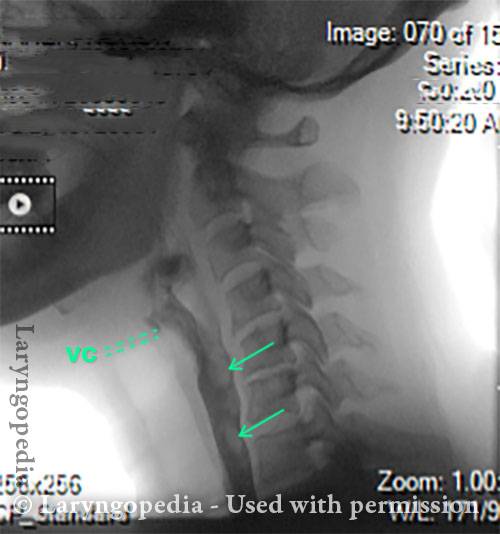
UES refuses to open for a burp (5 of 6)

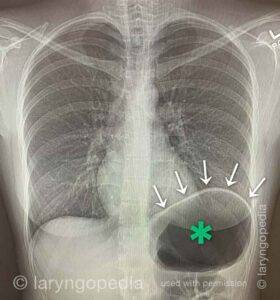
Abdominal Distention from R-CPD (6 of 6)
Distensão Abdominal de DCF-R
Gastric Air Bubble (1 of 3)
Bloated Abdomen (2 of 3)

Non-bloated Abdomen (3 of 3)

Distensão abdominal causada por DCF-R
Bloating and abdominal distention before botox injection for inability to burp (1 of 2)

Resolved, one month after botox, with burping restored (2 of 2)

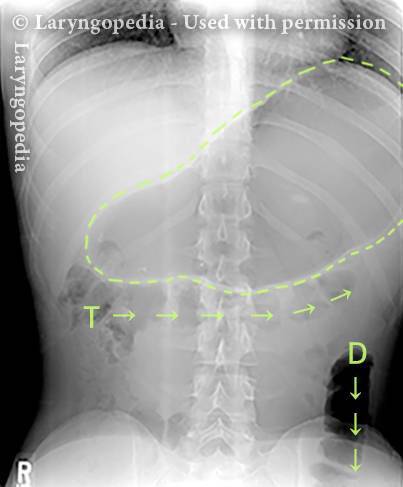
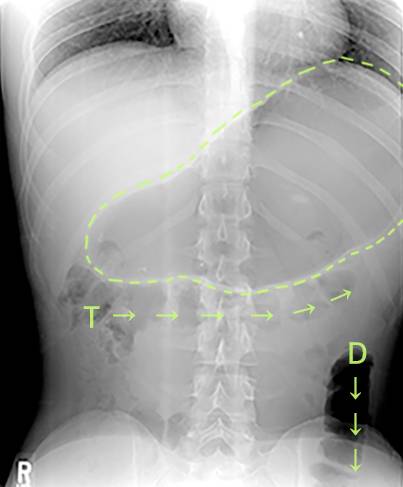
Não consigo arrotar: progressão do inchaço e distensão abdominal – um ciclo diário para muitos com DCF-R
Esta jovem tem sintomas clássicos de DCF-R – a síndrome de não conseguir arrotar. No início do dia, seus sintomas são menores e o abdômen está no “baseline” porque ela “esvaziou” por meio de flatulência durante a noite.
Nesta série você vê a diferença na distensão abdominal entre o início e o final do dia. As imagens de raios X mostram a notável quantidade de ar retido que explica seu inchaço e distensão. Sua progressão é bastante típica; alguns com DCF-R distendem ainda mais do que o mostrado aqui, especialmente depois de comer uma grande refeição ou consumir qualquer coisa gaseificada.
Side view of a bloated abdomen (1 of 6)

Front view (2 of 6)

Greater Distention (3 of 6)

Front view of bloating stomach (4 of 6)

X-ray of trapped air (5 of 6)
Side view (6 of 6)
O ciclo diário de inflação-deflação para DCF-R
Deflated Abdomen (1 of 4)

Bloated lateral view (2 of 4)
Deflated abdomen (3 of 4)

R-CPD distention (4 of 4)

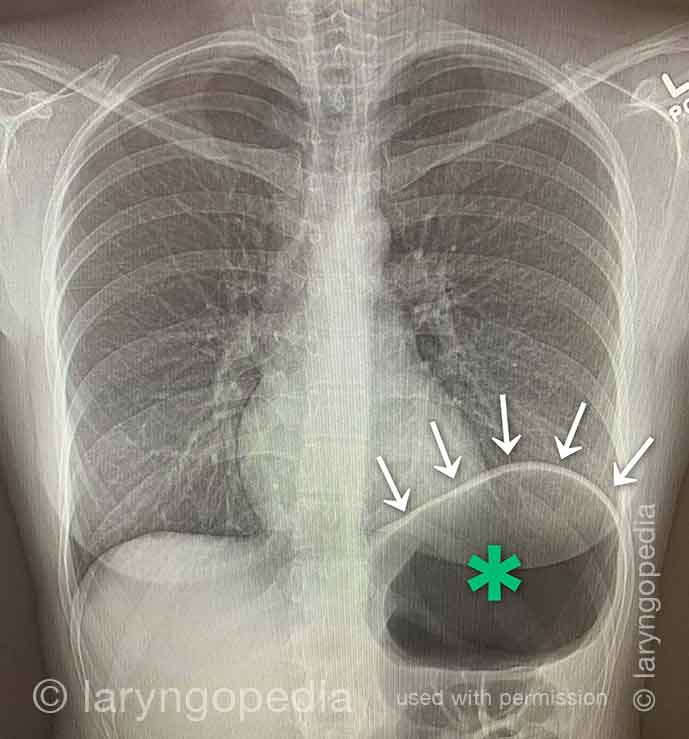
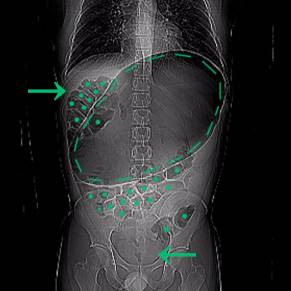
A Rare “abdominal crisis” Due to R-CPD (inability to burp)
This young man had an abdominal crisis related to R-CPD. He has had lifelong symptoms of classic R-CPD: inability to burp, gurgling, bloating, and flatulence. During a time of particular discomfort, he unfortunately took a “remedy” that was carbonated.
Here you see a massive stomach air bubble. A lot of his intestines are air-filled and pressed up and to his right (left of photo, at arrow). The internal pressure within his abdomen also shut off his ability to pass gas.
X-Ray of Abdominal Bloating (1 of 2)
Original X-Ray (2 of 2)

Shortness of Breath Caused by No-Burp
Persons who can’t burp and have the full-blown R-CPD syndrome often say that when the bloating and distention are particularly bad—and especially when they have a sense of chest pressure, they also have a feeling of shortness of breath.
They’ll say, for example, “I’m a [singer, or runner, or cyclist or _____], but my ability is so diminished by R-CPD. If I’m competing or performing I can’t eat or drink for 6 hours beforehand.” Some even say that they can’t complete a yawn when symptoms are particularly bad. The x-rays below explain how inability to burp can cause shortness of breath.
X-ray of trapped air (1 of 2)
Side view (2 of 2)
Achados Esofágicos
Aortic shelf (1 of 3)
Bony spur emerges due to stretched esophagus (2 of 3)

Stretched esophagus due to unburpable air (3 of 3)
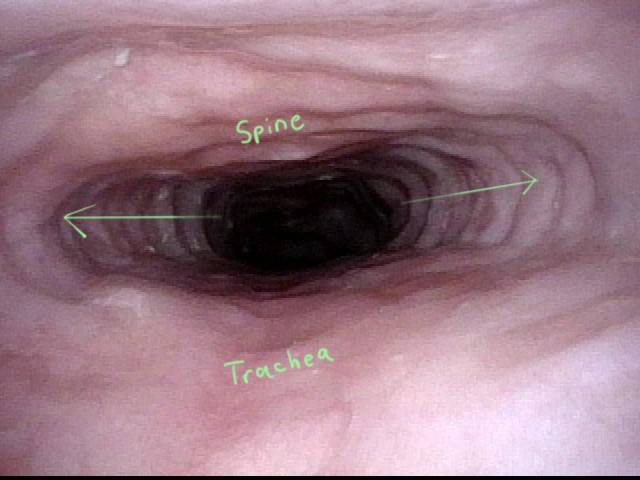
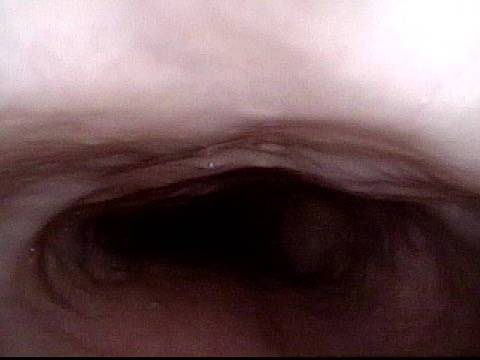
Alongamento Esofágico por Ar Não Burpável em DCF-R
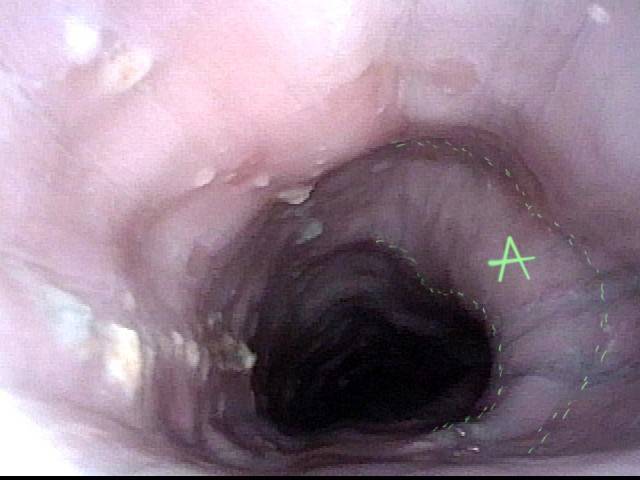
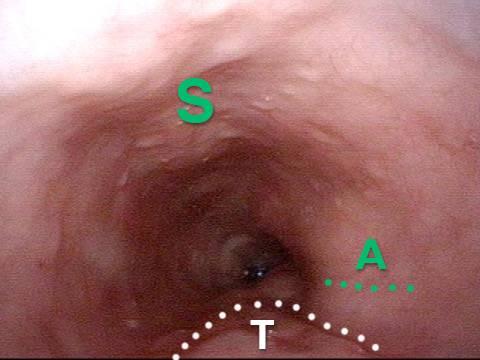
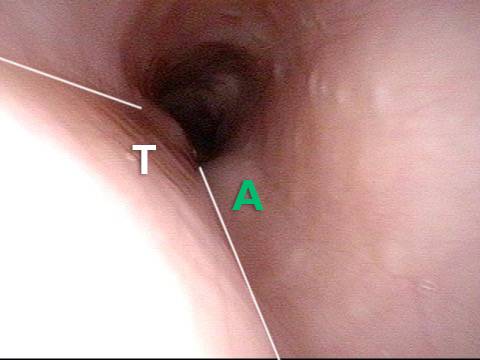
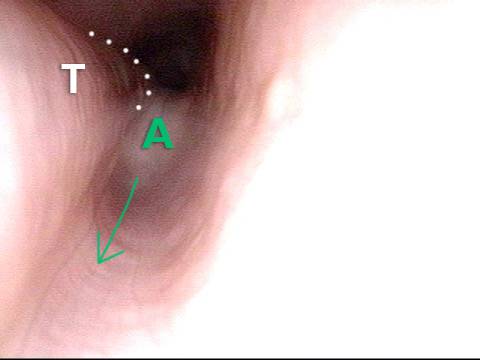
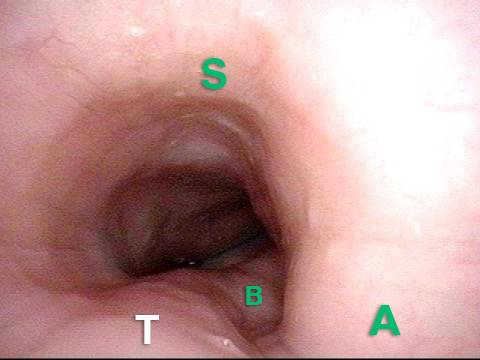
Este jovem teve a síndrome clássica de DCF-R ao longo da vida. Seus achados esofágicos ao final de um estudo videoendoscópico da deglutição são clássicos. O esôfago é principalmente um tubo muscular colapsado em pessoas jovens, mas seu esôfago está amplamente aberto de forma contínua devido ao ar engolido que ele não consegue arrotar.
Typical view of an esophagus (1 of 4)

Lower esophagus (2 of 4)
Stretched mid-esophagus (3 of 4)
Esophagus stretches laterally (4 of 4)
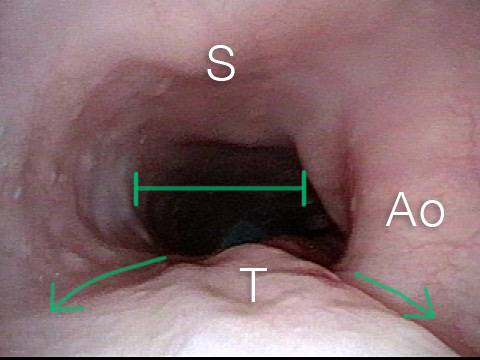
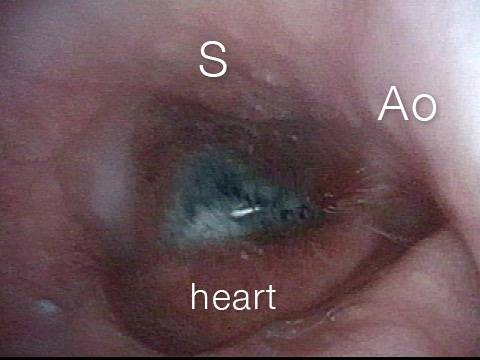
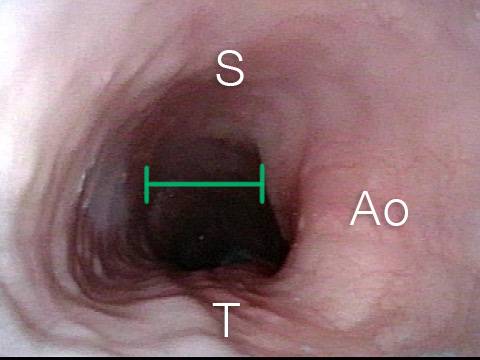
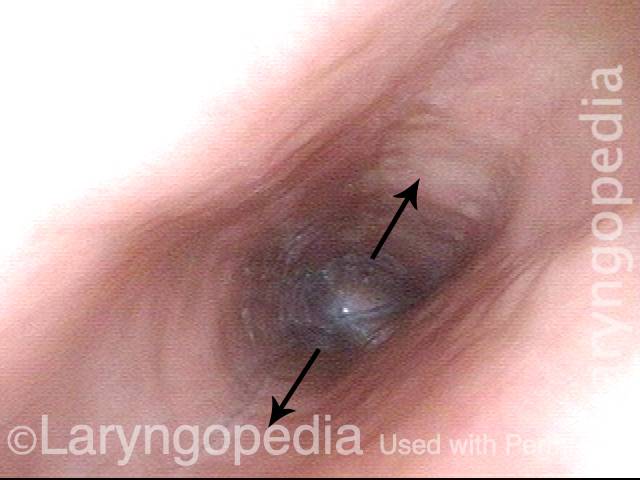
Achados esofágicos mais interessantes de DCF-R (incapacidade de arrotar)
Stretched Esophagus (1 of 4)
Tracheal Wall (2 of 4)
Over-dilation (3 of 4)
Bronchus (4 of 4)
DCF-R e dilatação esofágica
Posterior pharyngeal wall (1 of 3)
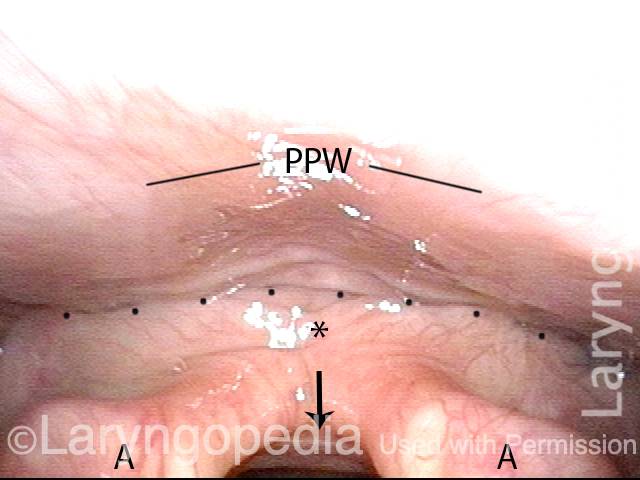
Is it R-CPD? (2 of 3)
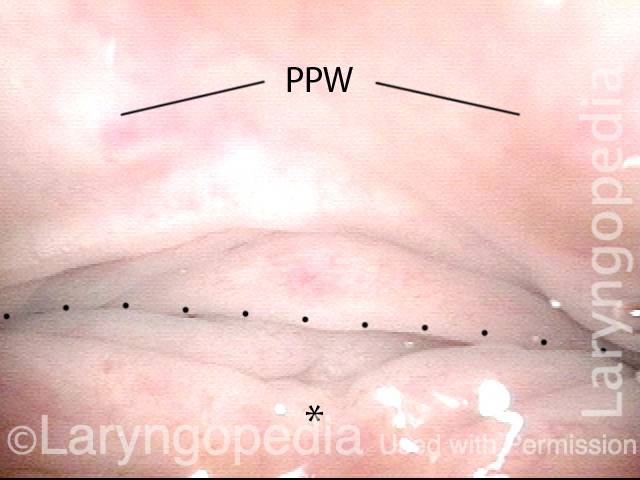
Stretched esophagus indicates R-CPD (3 of 3)
Como pode ser o esôfago “abaixo de um arroto”
Baseline (1 of 3)

Pre-burp (2 of 3)
Post-burp (3 of 3)

![]()
Vídeos sobre DCF-R


![]()
Artigos DCF-R publicados pelo Dr. Bastian
![]()
Recursos adicionais do DCF-R





Sphincters
Made of Stronger Stuff
Gleeks & Gurgles
Reply All


No-Burp: It's not just you
(26,000+ no-burpers)

Retrograde Cricopharyngeus Dysfunction (R-CPD)
[2,200+ membros]
I can now burp
@Lilamycox
My weird medical history
@Brittcurls
My R-CPD journey
Julie Anne Gay