La sifonía espasmódica (SD) es un trastorno neurológico que no pone en peligro la vida en el que los músculos de la laringe sufren espasmos involuntarios e interfieren con la voz. La SD es una distonía focal, que en este caso afecta a la laringe, es decir, distonía laríngea. La distonía laríngea generalmente afecta la voz, pero ocasionalmente también puede afectar la respiración (distonía respiratoria). El término disfonía espasmódica se refiere específicamente a la distonía laríngea que afecta la voz.
Adductor vs. Abductor SD
Existen dos variantes principales de disfonía espasmódica (SD). En la primera variante, adductor SD (AD-SD), las cuerdas vocales se presionan excesivamente, cortando palabras de forma intermitente o dando a la voz una cualidad estrangulada constante; esta variante comprende el 90% de los casos de SD.
En la segunda variante, abductor SD (AB-SD), las cuerdas vocales se separan abrupta y momentáneamente mientras se habla, lo que hace que la voz se apague por completo o se convierta en un susurro y un sonido entrecortado. Hay algunos casos en los que una persona tiene ambas variantes: esto se llama SD mixta AB-AD.
SD Clásica vs. Tónica
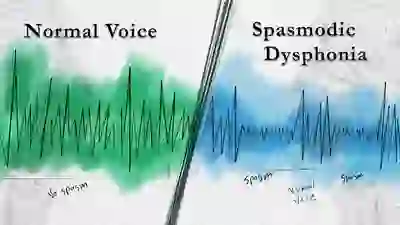
Otra distinción que se puede hacer es entre los casos de variante clásica y variante tónica de SD. En la variante clásica de SD, los espasmos provocan paradas fonatorias, es decir, mientras la persona habla, las palabras o sílabas intermitentes se ahogan (en AD-SD) o se abandonan (en AB-SD).
En la variante tónica SD, los espasmos son más continuos, de modo que la voz suena continuamente tensa (con AD-SD) o entrecortada (con AB-SD), pero sin ninguna parada fonatoria real. Debido a que la presencia de paradas fonatorias es el síntoma más frecuentemente asociado con la SD, la variante tónica de la SD no se diagnostica o se diagnostica erróneamente con mucha más frecuencia que la variante clásica de la SD.
Tratamiento para la Disfonía Espasmódica
No existe una “cura” definitiva para la SD, pero para la mayoría de los pacientes, las inyecciones periódicas de Botox™ en los músculos de la laringe son de gran ayuda, si existe una dosis y ubicación óptimas. Estas inyecciones relajan los músculos de la laringe que funcionan mal, minimizando así los espasmos y su impacto en la voz.
El efecto de una inyección suele durar unos meses y luego es necesaria otra inyección. Para aquellos que tienen dificultades para obtener buenos resultados con la terapia Botox™, vean nuestro video a continuación “Disfonía espasmódica: cuando el Botox decepciona”.
El tratamiento quirúrgico líder que se ofrece actualmente para la SD, la denervación-reinervación selectiva del aductor laríngeo (SLAD-R), puede ser una opción para personas con la variante AD-SD. Sin embargo, ningún tratamiento para la SD funciona satisfactoriamente para todos. La historia de cada uno de los distintos tratamientos quirúrgicos para la SD siempre incluye algunos fracasos.
La logopedia es otro tratamiento que a veces se sugiere para la SD. Si bien existen defensores individuales fuertes e incluso apasionados de la terapia del habla, la opinión generalizada es que no se espera que la terapia del habla mejore sustancialmente las capacidades de la voz o reduzca los espasmos excepto quizás en la sala de terapia.1.
Un curso breve de logopedia puede resultar muy útil para la educación del paciente y quizás para la búsqueda de trucos sensoriales. Hay mucha confusión en torno a este tema, porque a las personas que tienen un trastorno de la voz no orgánico se les puede diagnosticar erróneamente SD, y los trastornos de la voz no orgánicos se “curan” de manera rutinaria solo con terapia del habla.
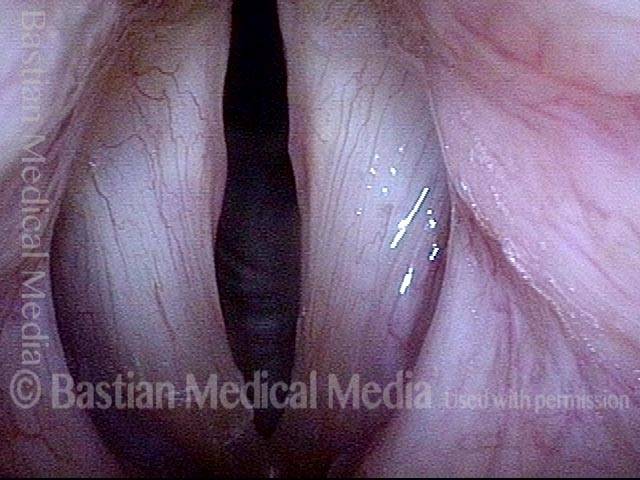
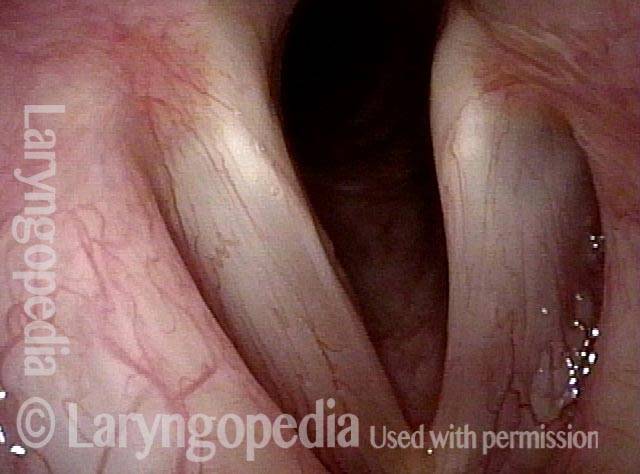
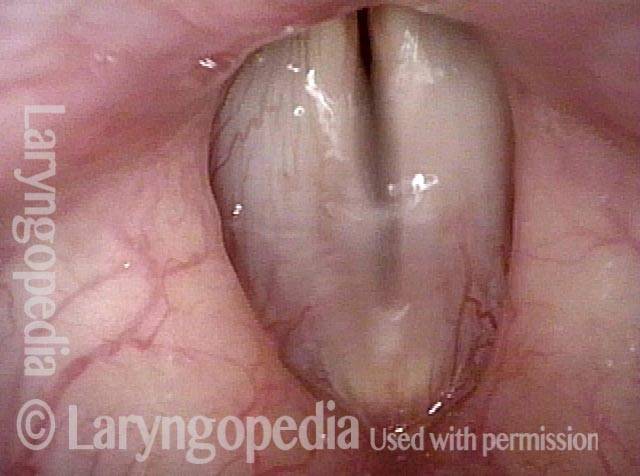
Disfonía Espasmódica Adductora
AD-SD (1 of 2)

AD-SD (2 of 2)
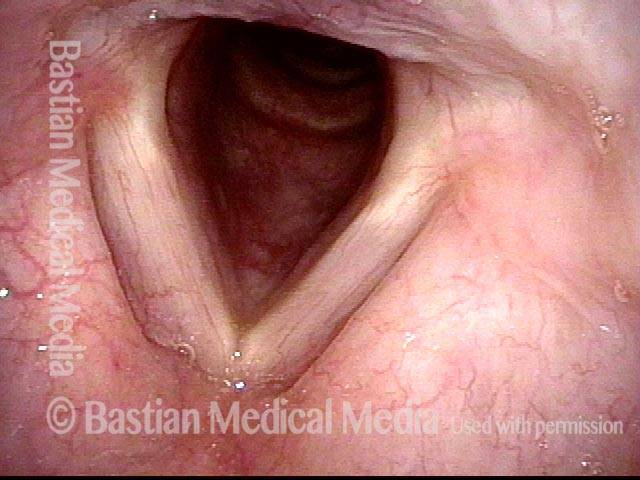
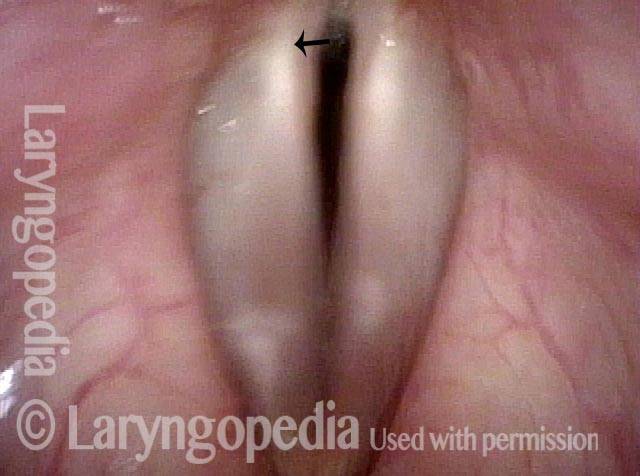
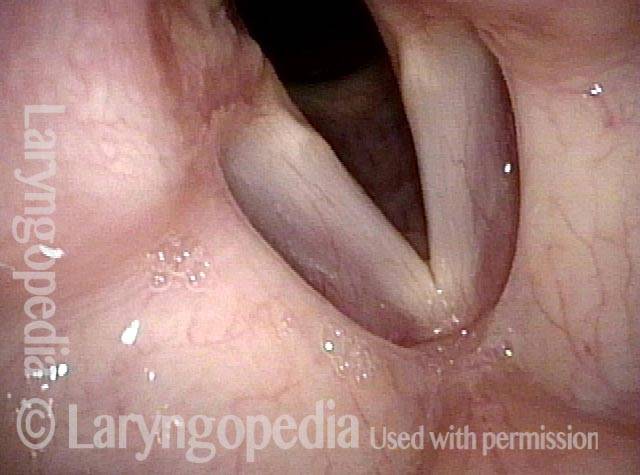
Disfonía Espasmódica Abductora
AB-SD (1 of 4)
AB-SD (2 of 4)
AB-SD (3 of 4)
AB-SD (4 of 4)
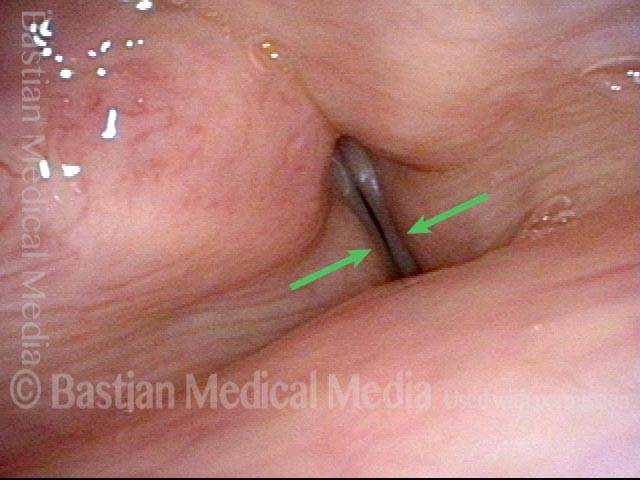
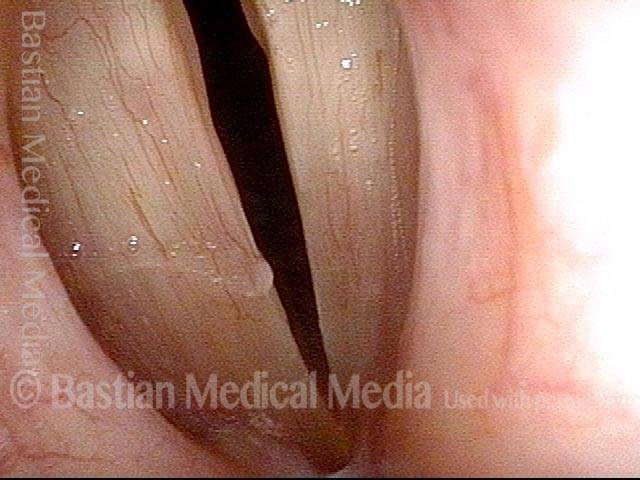
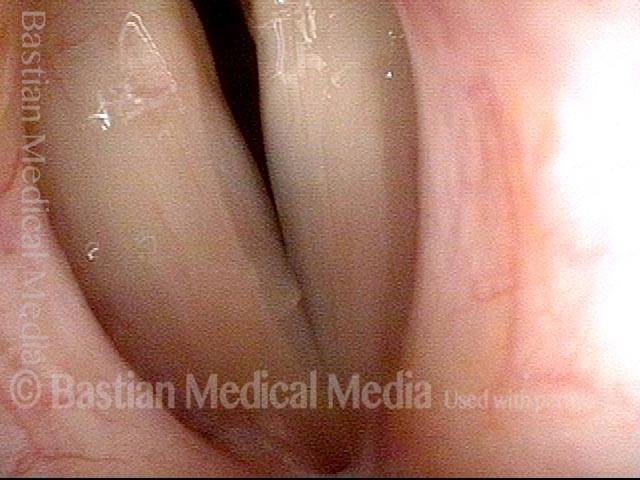
Espasmos Abductores, Empeorados por la Carga Cognitiva
Abductor spasmodic dysphonia patient (1 of 4)
Limited abductor spasms (2 of 4)

Increased abductor spasms (3 of 4)
Even greater abductor spasms (4 of 4)

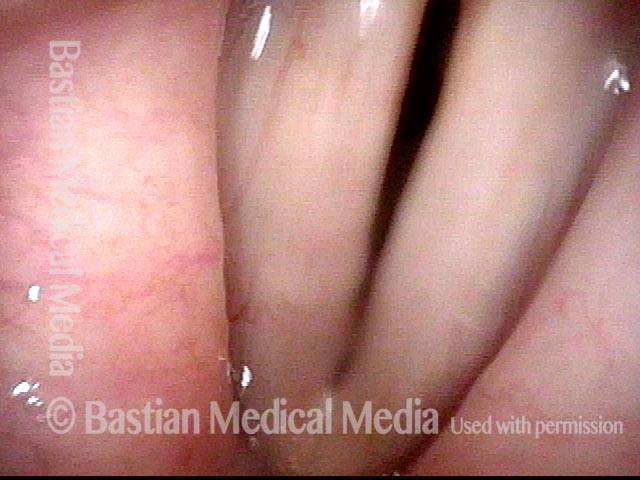
Espasmo Adductor
Adductory spasm (1 of 2)
Adductory spasm (2 of 2)

Laryngology 401: Paresia Solo con PCA, Pero el Problema Real de la voz es la Disfonía Espasmódica
Sense of instability (1 of 3)
Vibratory amplitude (2 of 3)
Spasm (3 of 3)
Notable Especificidad de Tareas de la Disfonía Espasmódica
Young singer (1 of 4)
Phonation (2 of 4)

Closed phase (3 of 4)

Sudden spasm (4 of 4)
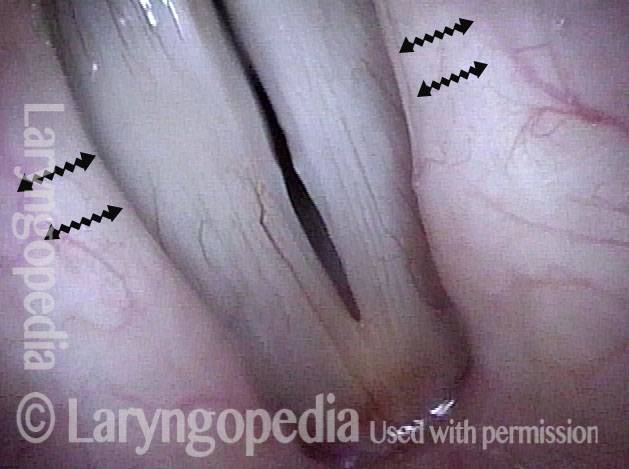
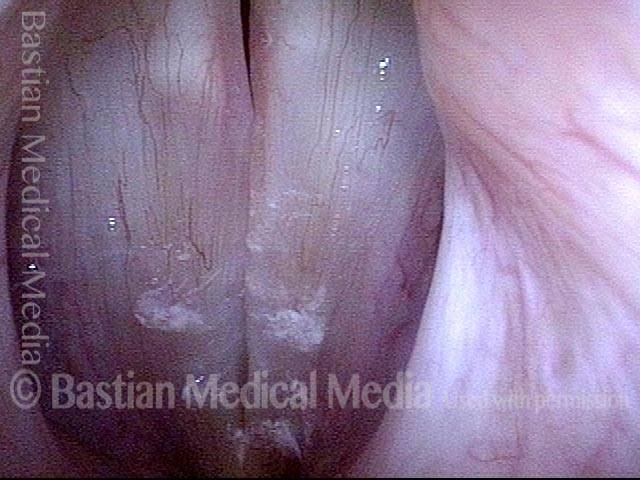
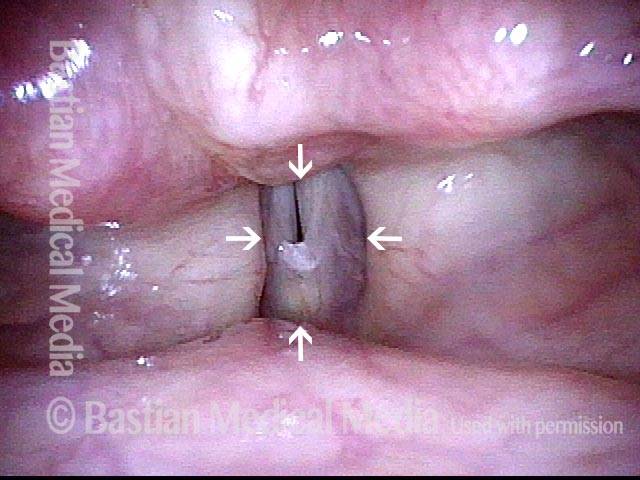
La Evaluación de la Fenomenología Vocal Protege de las Pistas Falsas Visuales
Swelling? (1 of 2)

Spasmodic dysphonia (2 of 2)