Toward the midline of a person’s body, along the left-right axis. For example: the medial end of each eyebrow is the end that approaches the bridge of the nose. The opposite of lateral.
Medial Examples in Relation to Laryngology:
Medialization, before and after
Before medialization (1 of 4)
Right vocal cord (left of photo) paralysis. During breathing as shown here, the right cord (left of photo) is paramedian, while the left cord (right of photo) is widely abducted. Note also the bowing (curvature) of the right cord (left of photo), and the prominent ventricle, both of which are indications of atrophy/ reduced bulk of the muscle within that cord.
Before medialization (2 of 4)
Phonation, with vibratory blurring under standard light. Right cord (left of photo) remains paramedian, and the left cord (right of photo) has swung to the midline. Even so, large gap between the cords shows that closure is incomplete, and this explains the weak, air-wasting voice; the patient can only say a few words before running out of air and having to take another breath.
After medialization (3 of 4)
After medialization and placement of a silastic implant, the right cord (left of photo) is less atrophied and the bowing much diminished. The cord has also been shifted slightly to the midline.

After medialization (4 of 4)
Phonation, again with vibratory blurring, but notice the much better approximation of the cords. The voice is stronger, and less air-wasting.

Classic Findings Again of PCA-only Paresis
Post thyroidectomy (1 of 4)
After thyroidectomy, this individual’s voice was breathy for several months postoperatively, but then recovered fully. Yet, her right vocal cord appears to be paralyzed, rather than paretic. Here note that PCA on the left (right of photo) pulls that (normal) cord fully laterally, while the right cord (left of photo) remains midline and with slight medial turning of the vocal process to suggest right LCA muscle is intact.
Phonatory view (2 of 4)
Making voice under standard light, the cords appear to close at the midline, consistent with intact IA and bilaterally intact LCA muscles. Equal vibratory blur between the two sides suggests that the both TA muscles are also intact.

LCA and TA muscles working (3 of 4)
Under strobe light, closed phase of vibration: Medial compression appears equal and the vocal processes (indicated by lines) point straight anteriorly, again confirming that both LCA muscles are working, and suggesting that both TA’s are also working.
PCA-only paresis (4 of 4)
Open phase with equal amplitude (lateral excursion) of vibration of both cords, indicating that the TA muscle is not atrophic or flaccid. Put all of the above findings together, and this is classic PCA-only paresis of the right vocal cord.

TA-only Paresis before and after Voice Gel Injection
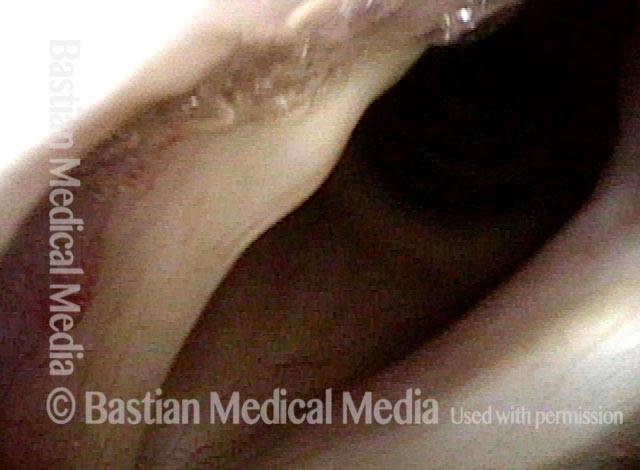
TA weakness, intact LCA + PCA (1 of 5)
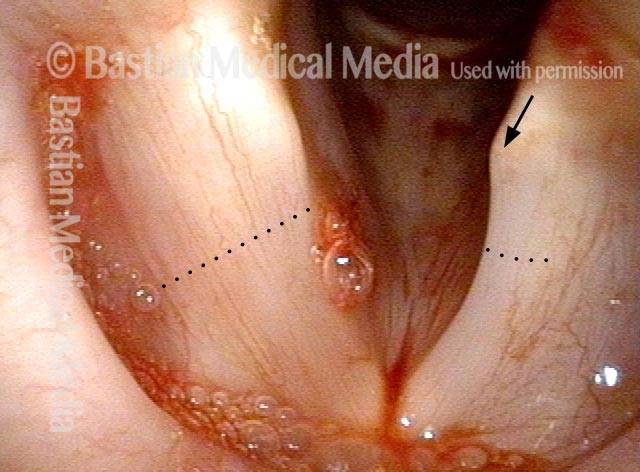
TA weakness indicated by bowed margin and “spaghetti-linguini” difference between the cords. Medial turning of vocal process (arrow) suggests intact LCA; abducted position suggests intact PCA function. Blood is from cricothyroid membrane puncture to instill topical anesthesia.
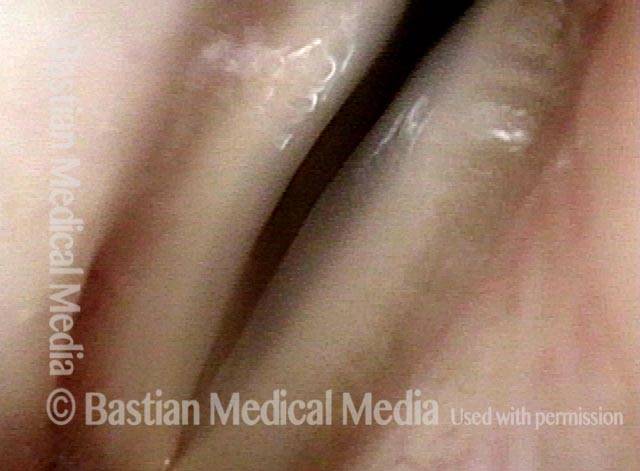
Prephonatory instant (2 of 5)
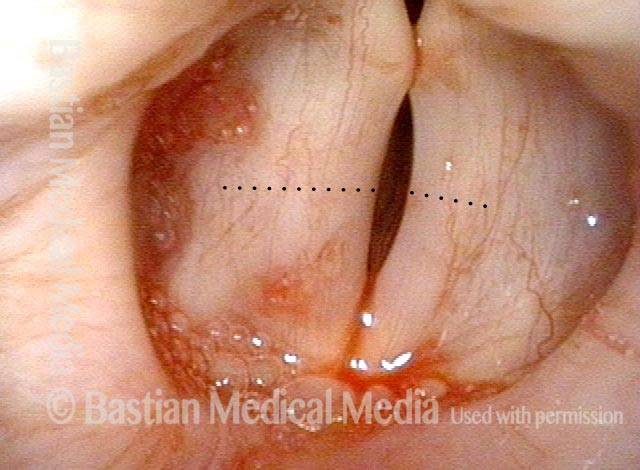
Before voice gel injection at prephonatory instant. Wasting of left cord (right of photo), and capacious ventricle on the left (right of photo) clearly evident.
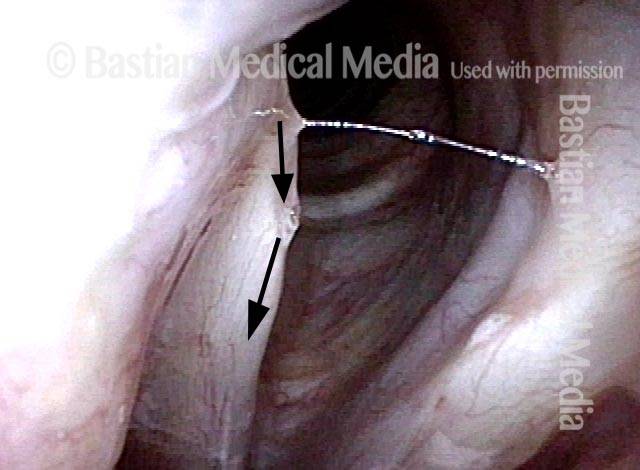
Gel injection (3 of 5)
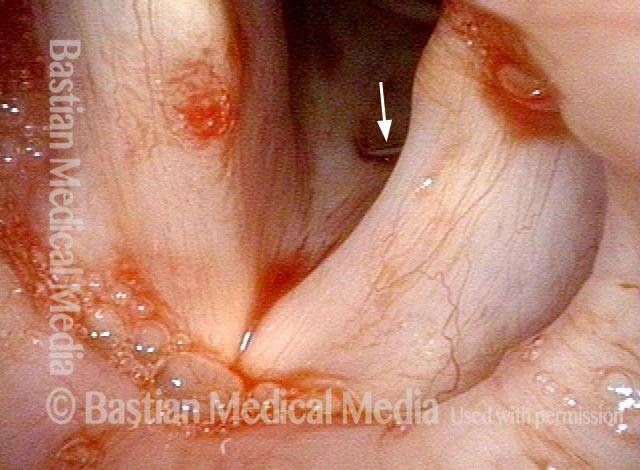
At beginning of voice gel injection (needle at white arrow).
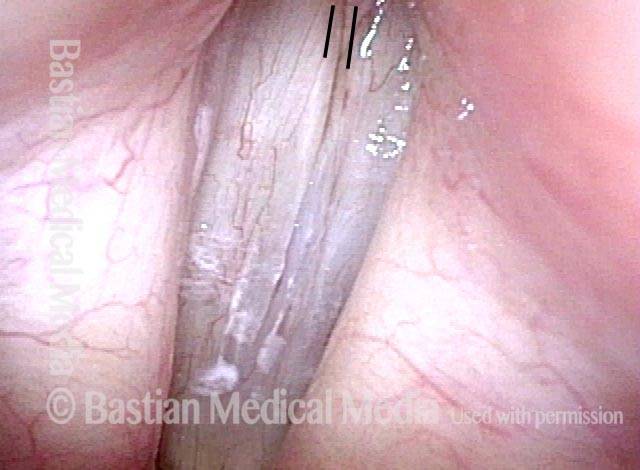
Straight vocal cord margin (4 of 5)
At conclusion of voice gel, note straight left cord margin (right of photo). Compare with photos 1 and 3.

Phonation (5 of 5)
Phonation after injection complete. Voice dramatically strengthened. Compare with photo 2.
