Idiopathic (unknown cause) inflammatory subglottic stenosis is a frustrating breathing problem seen mostly in women. It appears to be an autoimmune disorder that we have thought for many years to be an incomplete expression (forme fruste) of Wegener’s Granulomatosis, aka granulomatosis with polyangiitis (GPA). In a caseload of perhaps 125 patients, it appears that standard of care remains occasional outpatient dilation, steroid injection, and mitomycin C application. Most patients go a year or more between dilations. The rub: occasionally, dilations need to be done more frequently in an “active” case, or there may be reasons to avoid the brief general anesthesia required for dilation such as: morbid obesity, difficult jaw/tooth/neck anatomy, or even a phobia of general anesthesia.
Podcast:
“Office” Treatment Option for Inflammatory Subglottic Stenosis
In such situations, one naturally casts about for alternatives. Low dose methotrexate has not been very effective in our experience. And we work with a motivated rheumatologist open to considering rituximab, even with a negative ANCA study. Or the laryngologist might consider an office-based airway procedure as illustrated in the photos below. This particular person only requires dilation every 18 months or so, but it represents a major stressor for her given her fears, her size, and somewhat challenging anatomy. She is one of several offered the treatment shown below: steroid injection in the voice laboratory, followed by laser treatment.
Our thought is that in some, it may be the ridges and air turbulence that creates the feeling of airway restriction, or that these rings of stenosis “catch” mucus. In the case below, the clinician was almost dubious that what was accomplished would make that much difference to the person’s breathing. But upon calling her a week after the procedure below, and asking if the improvement was nil, subtle, small, medium, or large, she replied “large…a huge improvement.”
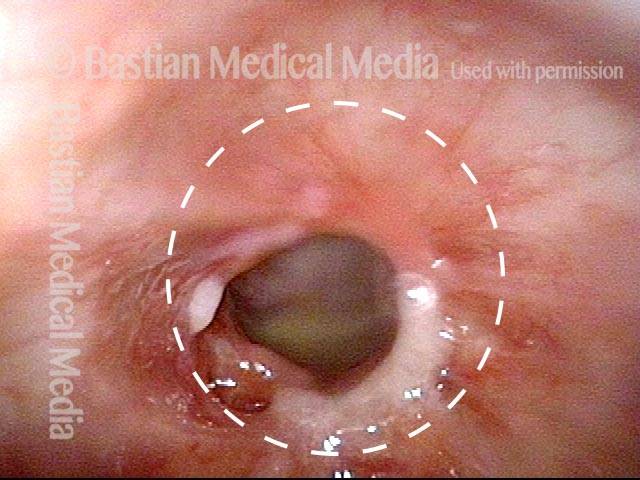
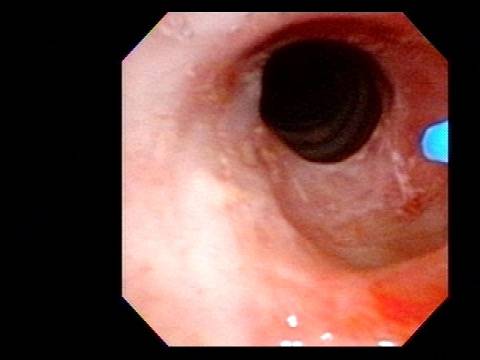
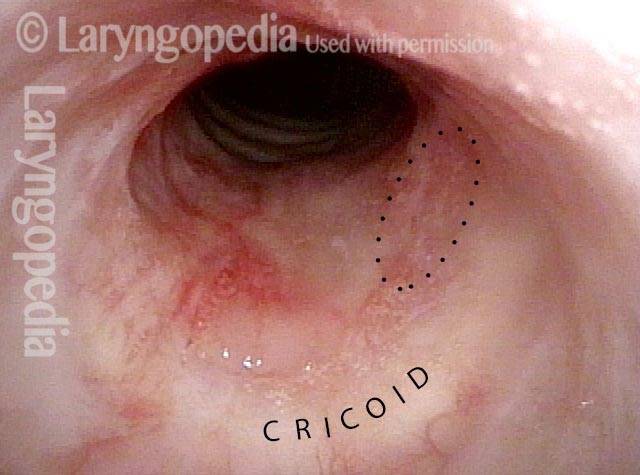
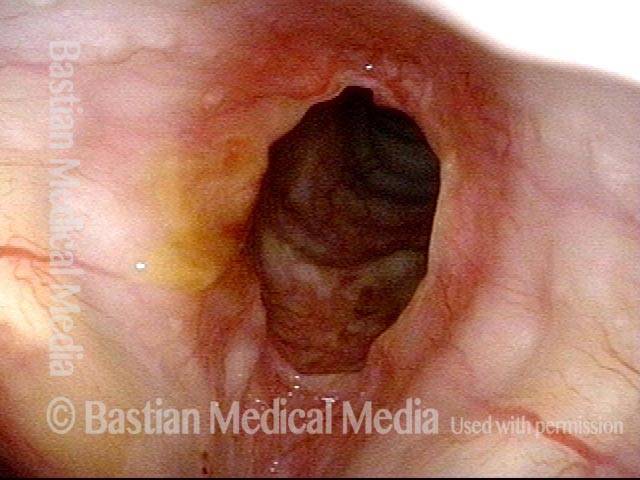
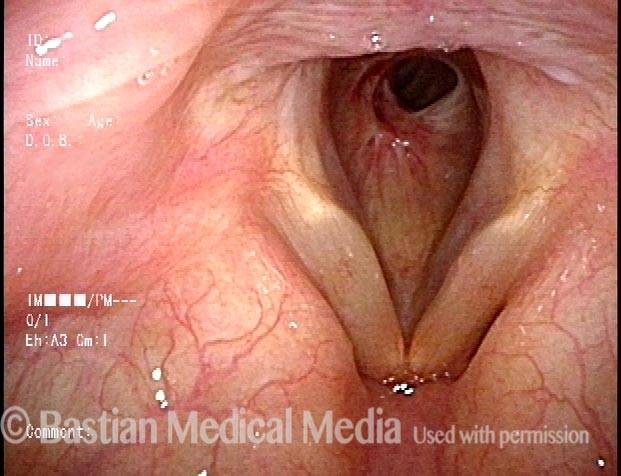
60% Stenosis (1 of 5)
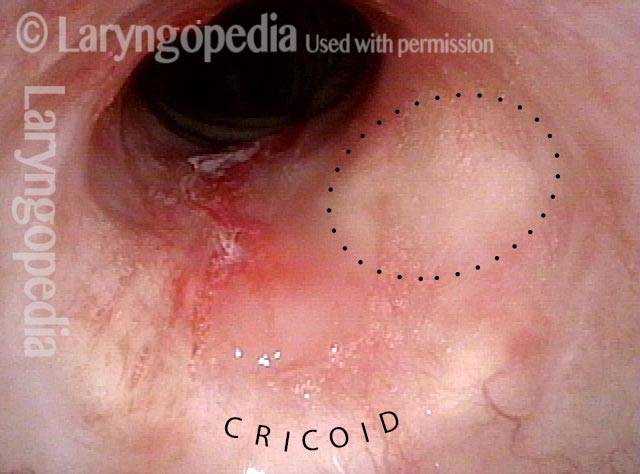
Narrowing & erythema (2 of 5)
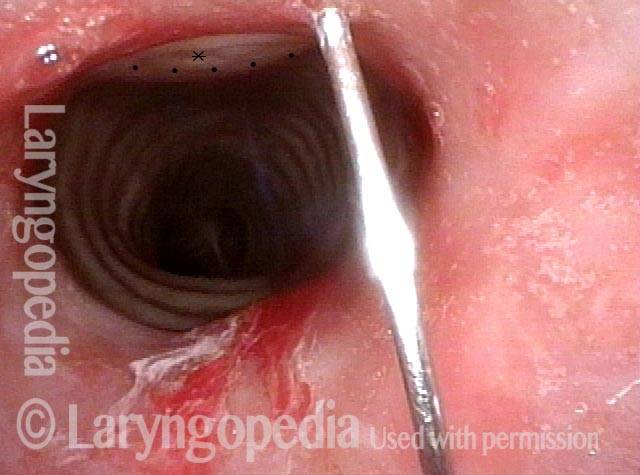
Triamcinolone is injected (3 of 5)
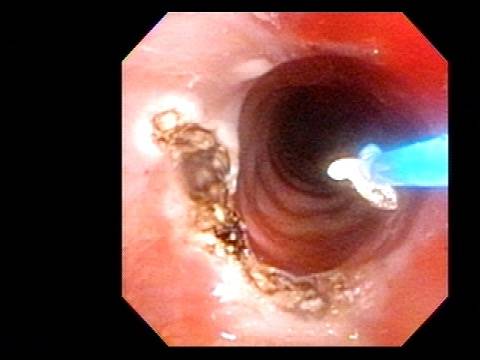
Laser ablation (4 of 5)
Stenosis is coagulated (5 of 5)
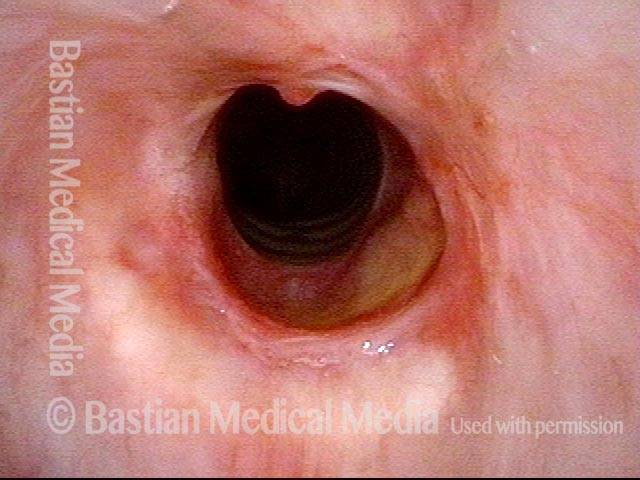
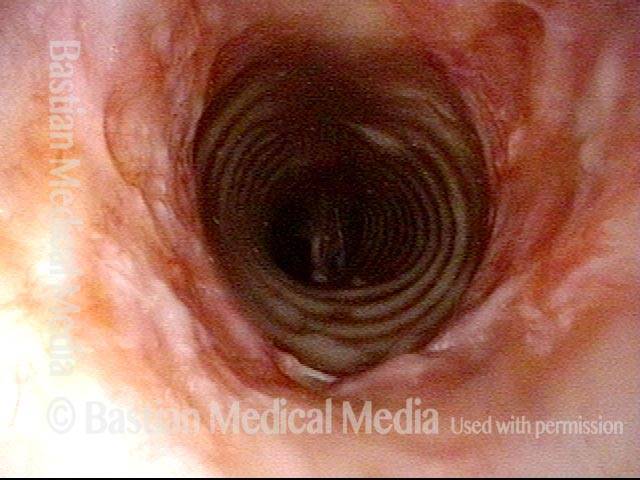
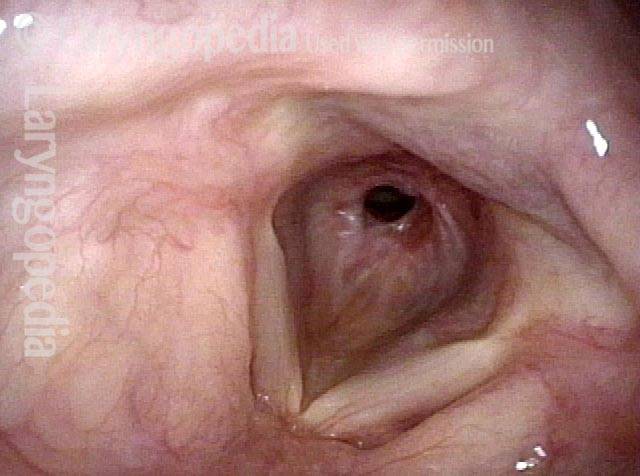
Idiopathic Subglottic Stenosis Has Different Levels
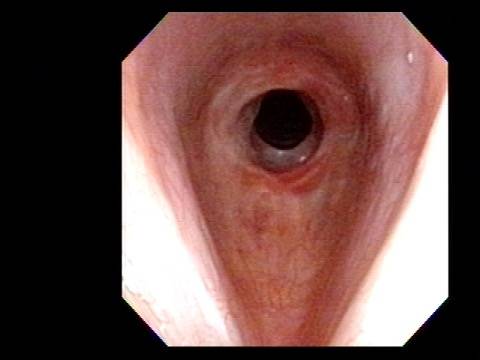
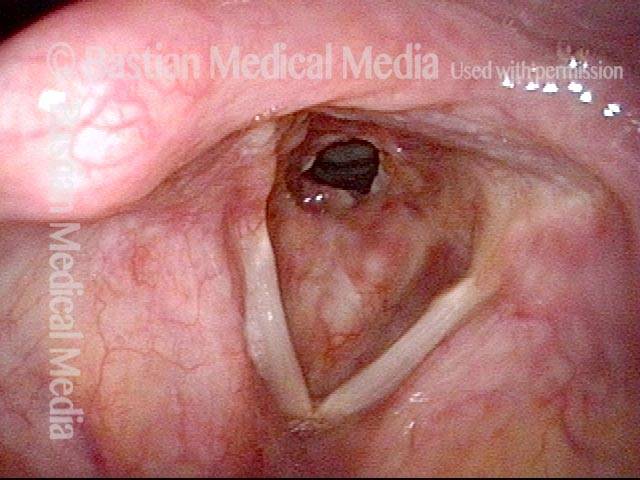
Post dilation (1 of 4)
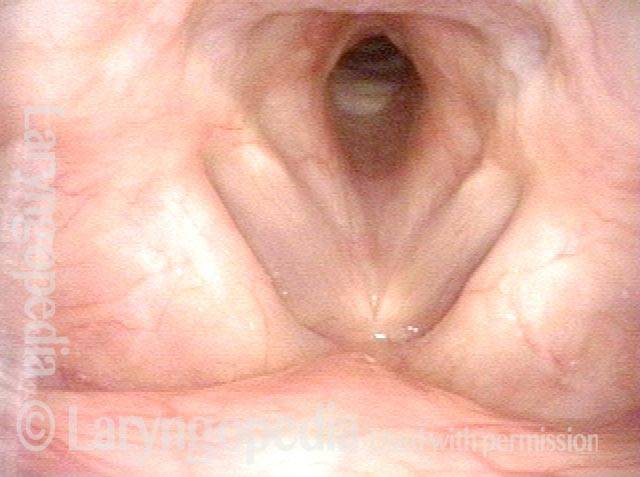
Closer view (2 of 4)

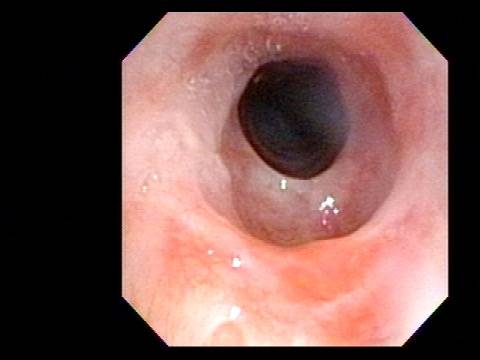
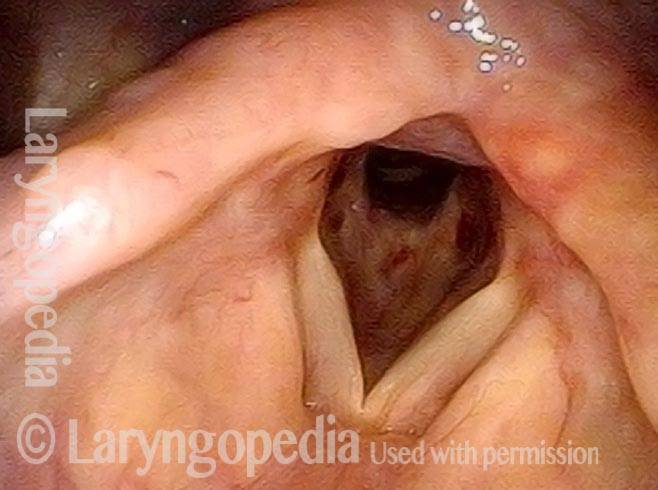
Rich vascular pattern (3 of 4)
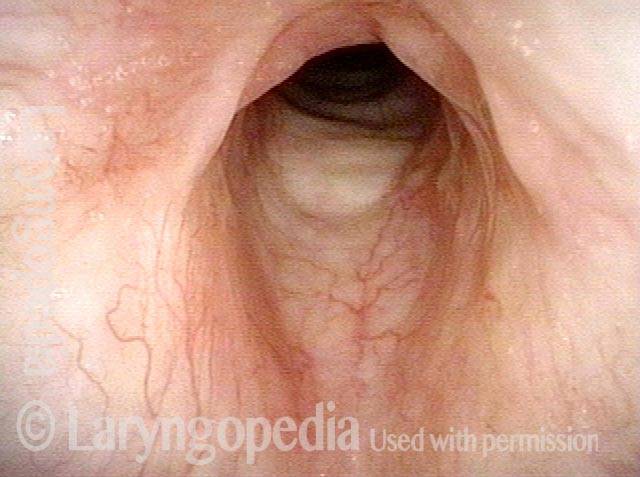
"Sharing" the airway (4 of 4)

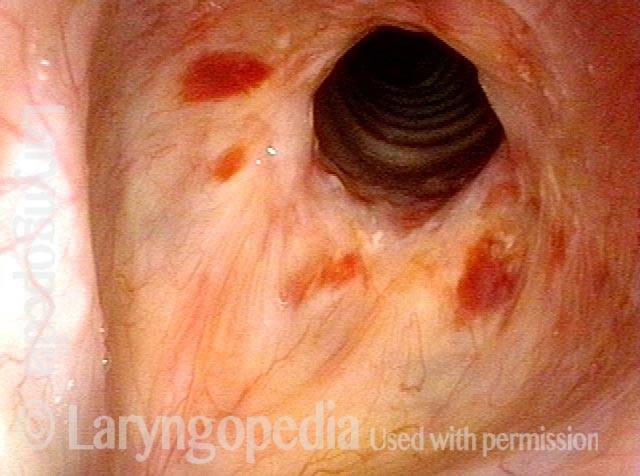
Another way to Inject Idiopathic Subglottic Stenosis
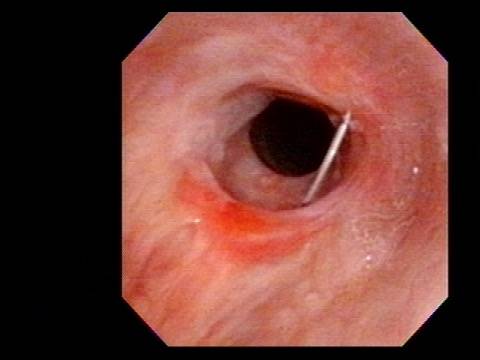
Idiopathic inflammatory subglottic stenosis (1 of 3)
Priot to injection (2 of 3)
Injection (3 of 3)
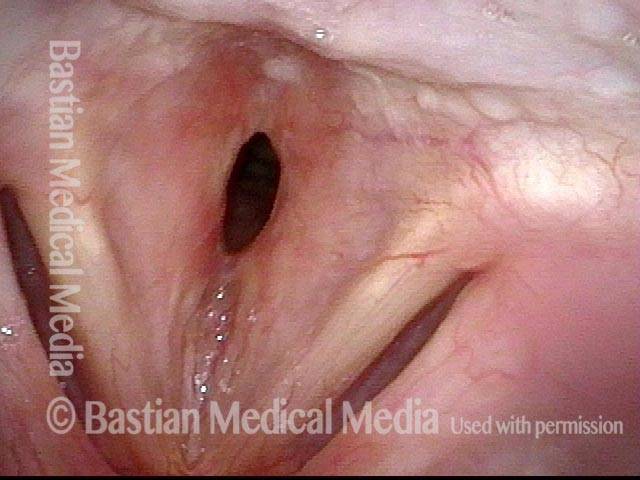
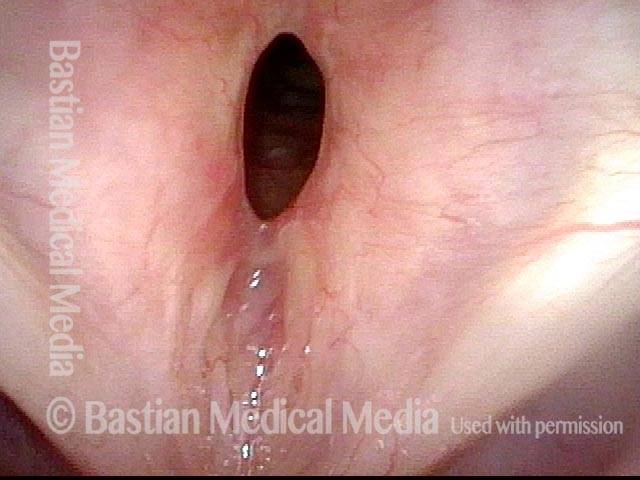
Subglottic Stenosis, after Treatment
Subglottic stenosis, before treatment (1 of 2)

Subglottic stenosis, after treatment (2 of 2)

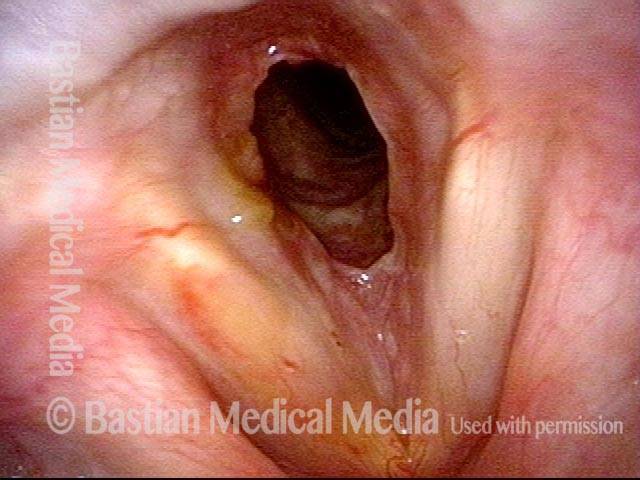
Subglottic Stenosis, before and after Dilation
Subglottic stenosis, before dilation (1 of 2)
Subglottic stenosis, after dilation (2 of 2)
Example 2
Subglottic stenosis (1 of 5)

Subglottic stenosis, worsened (2 of 5)
Subglottic stenosis, worsened (3 of 5)
Subglottic stenosis, after dilation (4 of 5)
Subglottic stenosis, after dilation (5 of 5)
Stenosis Before and After Dilation for Forme Fruste Wegener’s
Subglottic stenosis (1 of 5)
Inflammation (2 of 5)

Flexible scope (3 of 5)

Post-dilation (4 of 5)
Post-operative bruising (5 of 5)
Subglottic / Tracheal Stenosis
Wegener's granulomatosis (1 of 4)
Subglottic / Tracheal stenosis (2 of 4)

Subglottic / Tracheal stenosis (3 of 4)

Inflammed Stenosis (4 of 4)

Subglottic Stenosis, Due to Wegener’s Granulomatosis
Subglottic stenosis, due to Wegener's (1 of 2)
Subglottic stenosis, due to Wegener's (2 of 2)