Bronchoscopy is a procedure during which the examiner looks inside the trachea and bronchial tubes, typically using a slender, flexible fiberoptic or videoscope. At our practice, this procedure is usually performed using topical anesthesia with or without sedation, “in the chair” rather than in a hospital setting.
Wheezing, Induced by Bronchial Abnormality
Wheezing, induced by bronchial abnormality (1 of 5)
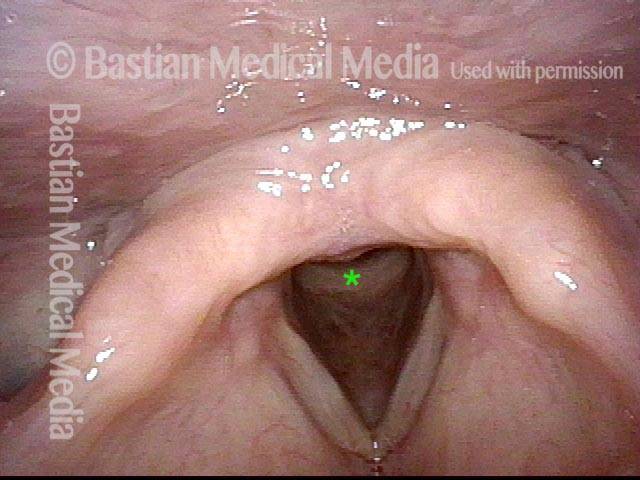
This patient has noticed faint wheezing for most of her life. Here is a panorama of the entrance to her larynx, which is normal—wide open and unobstructed—and does not yet explain her wheezing. For reference, an asterisk marks the upper surface of the cricoid ring.
Wheezing, induced by bronchial abnormality (2 of 5)
Further down, now just below the vocal cords; an asterisk again indicates the anterior cricoid ring. The upper tracheal rings here are normal. Still no explanation for her wheezing.
Wheezing, induced by bronchial abnormality (3 of 5)
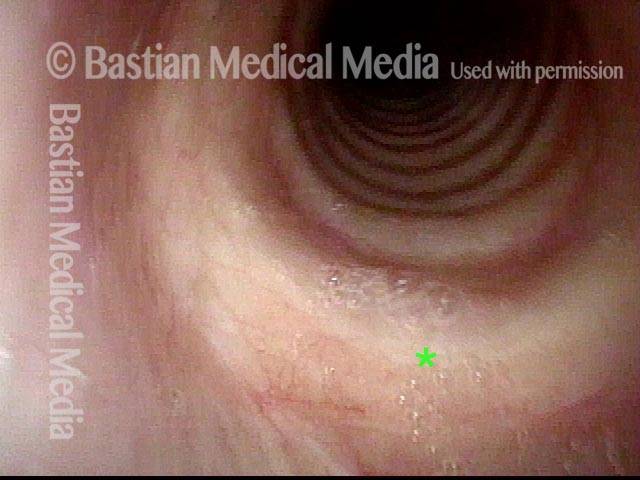
Further down yet, now into the mid-trachea. Still no sign of any anatomical cause for the wheezing.

Wheezing, induced by bronchial abnormality (4 of 5)
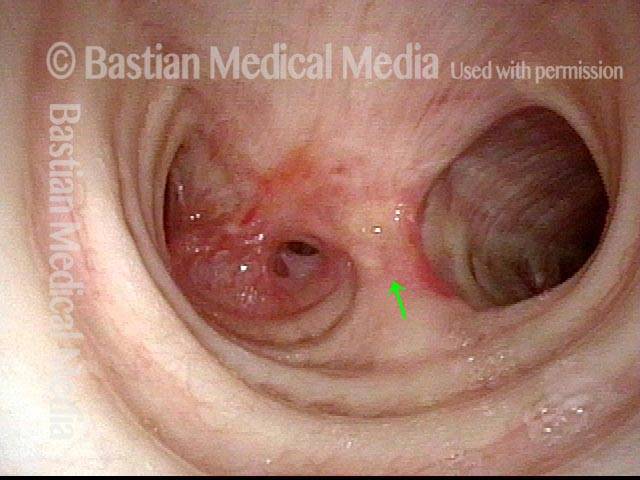
Further down still, viewing the distal trachea; an arrow marks the carina. The source of the wheezing now becomes evident: the take-off of the right main stem bronchus (left of image) is extremely abnormal and narrowed. The left main stem bronchus appears to have a subtle stenosis, which is a red herring.
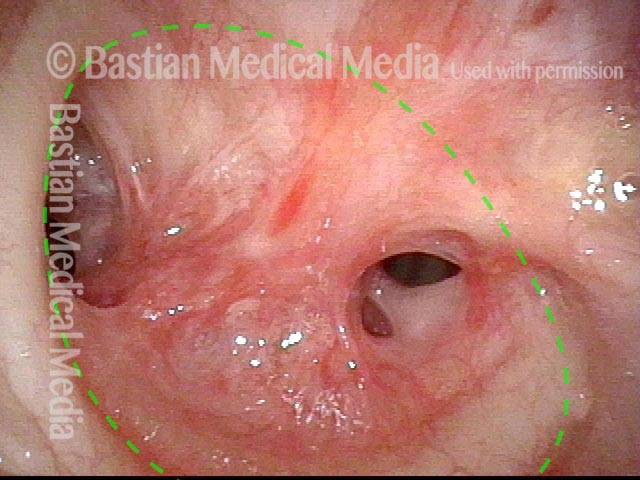
Wheezing, induced by bronchial abnormality (5 of 5)
Close-up on the abnormal take-off for the right main stem bronchus, which should be wide open. Instead, there are accessory bronchi exiting what is probably a congenital malformation. A dotted line indicates the expected size of this passageway, were it not malformed.
Tracheoesophageal Party Wall with Wheezing
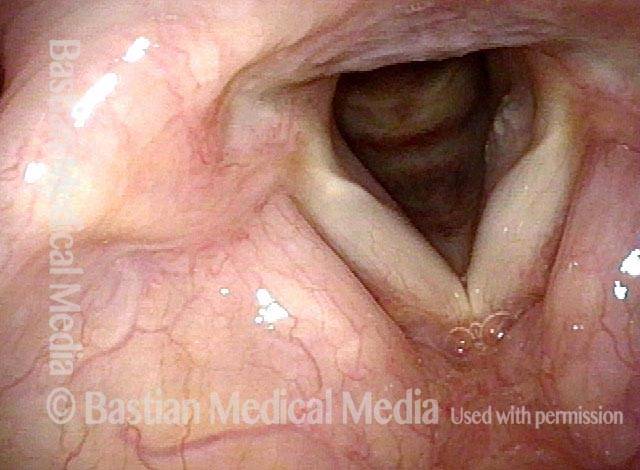
Abducted breathing position (1 of 5)
Normal laryngeal entrance, with vocal cords in abducted (breathing) position.
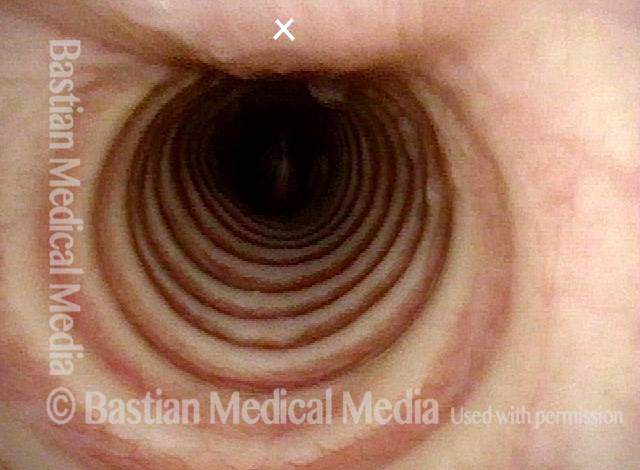
View of mid-trachea (2 of 5)
View in normal mid-trachea. Note that the cartilaginous rings make up approximately 2/3 of the circumference and that the membranous trachea (upper photo at 'X') is more flat.
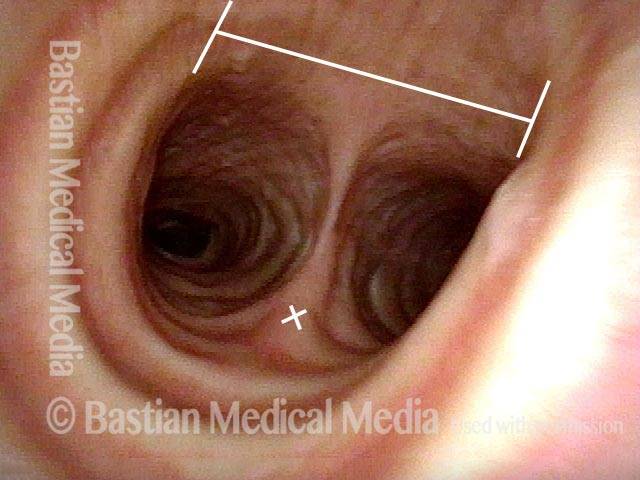
View just above the carina (3 of 5)
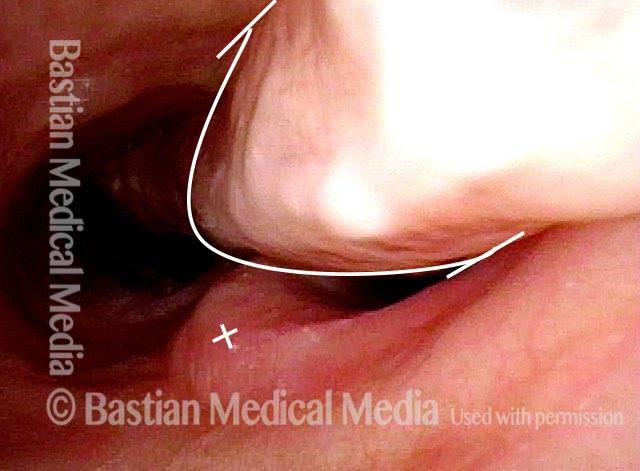
View just above the carina, where the distal trachea splits into left and right mainstem bronchi. Anterior take-off of carina at the 'X'. The straight line delimits the membranous (flexible) tracheal wall.
Wheezing begins (4 of 5)
With Valsalva maneuver to accentuate patient’s functional expiratory wheezing. Note that the membranous tracheal and bronchial walls bulge inward on a functional basis to narrow the airway. Wheezing begins to be heard. The 'X' again marks the anterior take-off of the carina. Compare with Photo 3.
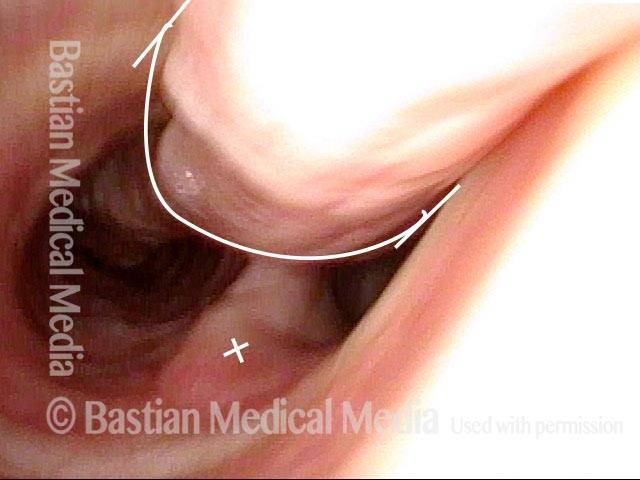
Left bronchus blocked (5 of 5)
As bulging inward continues, the left mainstem bronchus is particularly blocked. This explains why, on auscultation of the chest, wheezing sounds louder on the left than the right. Compare with photos 3 and 4.