Unilateral vocal cord paralysis is the neurogenic inability of one vocal cord to move. It is associated with weak voice of a degree that can vary between individuals. Symptoms may include one or more of the following:
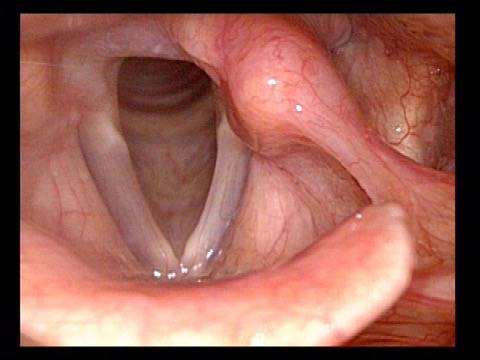
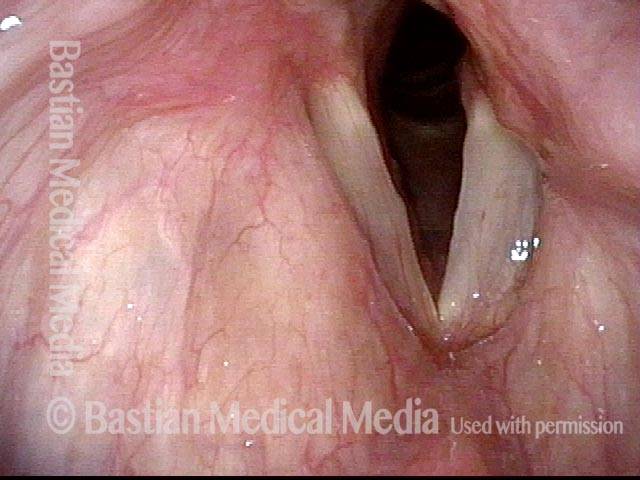
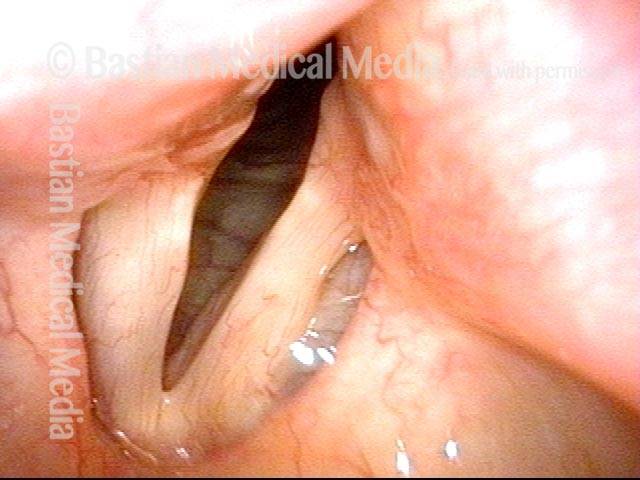
This person awakened with a weak, whispery voice after emergency abdominal surgery. Now 3+ months later, voice is returning by degrees but is still very weak. In this photo, the patient is breathing quietly. The weak left vocal cord is more bowed than the right.
This person awakened with a weak, whispery voice after emergency abdominal surgery. Now 3+ months later, voice is returning by degrees but is still very weak. In this photo, the patient is breathing quietly. The weak left vocal cord is more bowed than the right.
Reason for air-wasting (2 of 4)
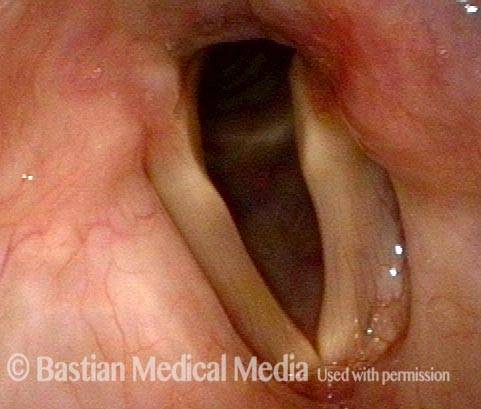
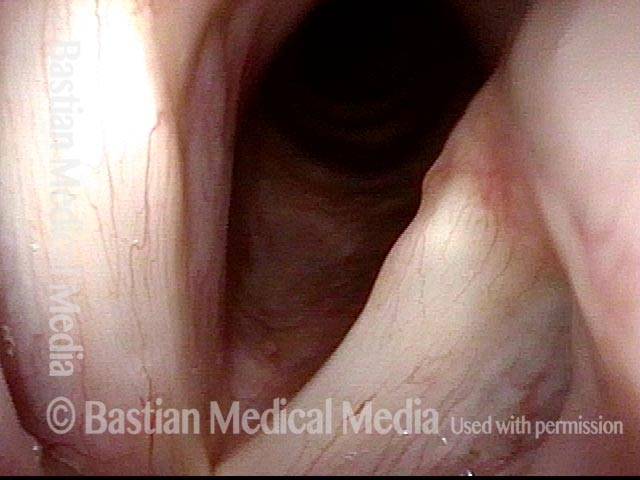
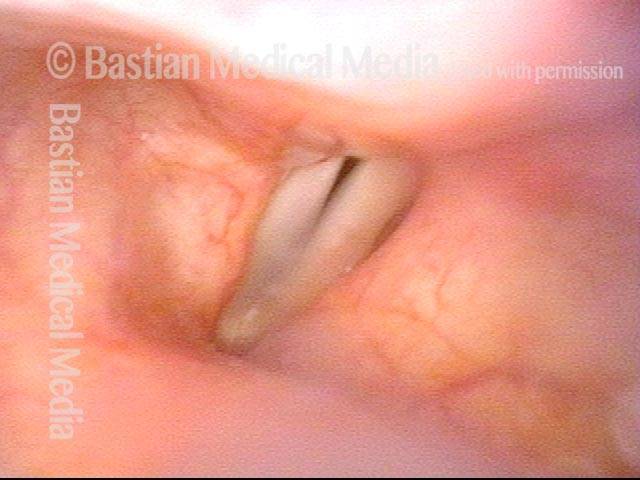
When she tries to produce voice, the left vocal cord comes only part of the way to the midline, leaving a large gap, and explaining her whispery air-wasting voice quality.
When she tries to produce voice, the left vocal cord comes only part of the way to the midline, leaving a large gap, and explaining her whispery air-wasting voice quality.
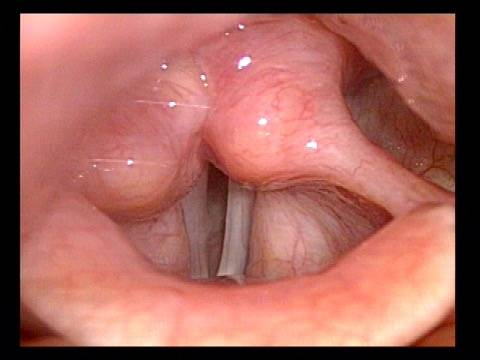
Voice gel injected into vocal cord (3 of 4)
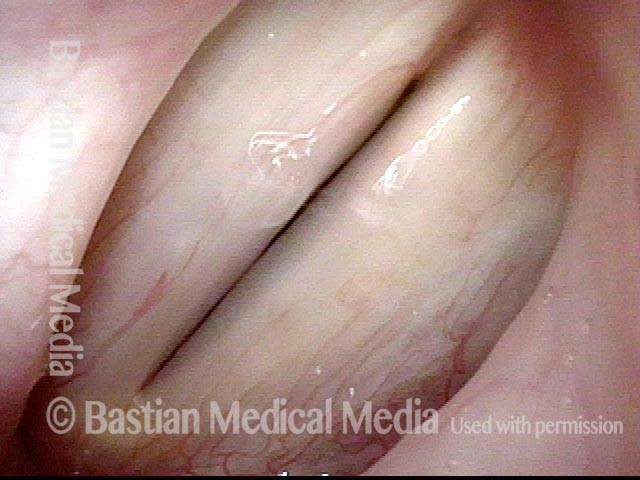
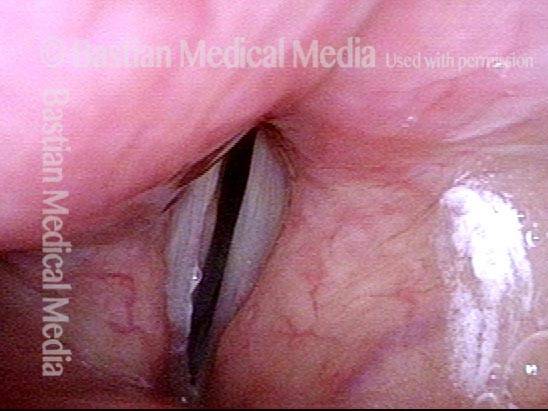
On the same day, due to pressing patient need, the left vocal cord was “plumped” with voice gel. That material typically provides temporary benefit of 6 to 12 weeks, gradually absorbing during that time.
On the same day, due to pressing patient need, the left vocal cord was “plumped” with voice gel. That material typically provides temporary benefit of 6 to 12 weeks, gradually absorbing during that time.
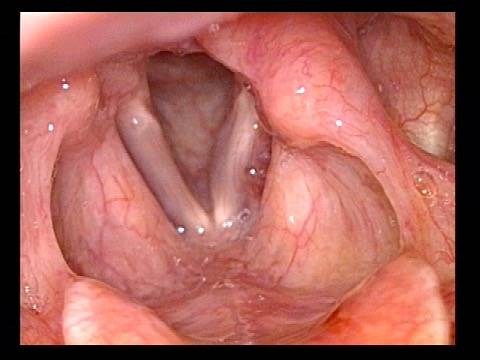
Vocal cords close completely (4 of 4)
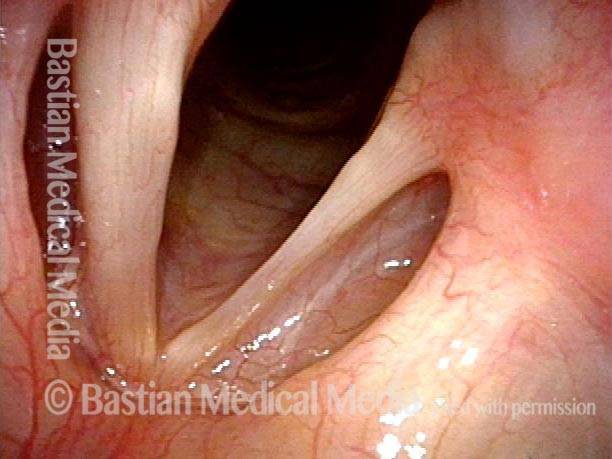
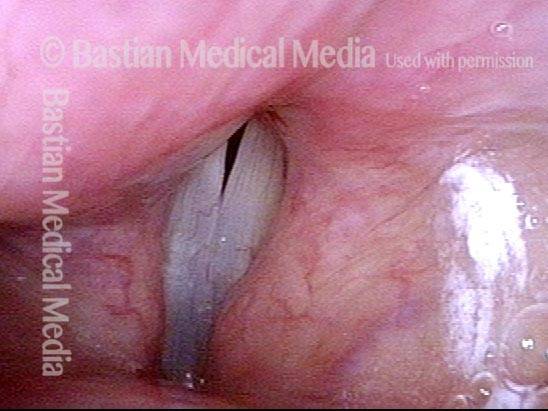
Voice is dramatically improved, now that her vocal cords can more fully close to reduce the air-wasting and transform the voice from whispery to strong. Compare with photo 2.
Voice is dramatically improved, now that her vocal cords can more fully close to reduce the air-wasting and transform the voice from whispery to strong. Compare with photo 2.
Vocal Cord Paralysis
Vocal cord paralysis (1 of 2)
Paralysis of left vocal cord (right of image), breathing position. Note that the left cord is bowed and atrophied as compared with the right.
Same patient during phonation, showing that the cords do not approximate; this correlates with a weak, breathy, air-wasting voice quality.
Example 2
Vocal cord paralysis (1 of 5)
This person has an extremely weak and air-wasting voice. Here, with the vocal cords in breathing position, the cause of this voice problem is not yet evident.
This person has an extremely weak and air-wasting voice. Here, with the vocal cords in breathing position, the cause of this voice problem is not yet evident.
The explanation becomes more apparent. As will ultimately be seen, this patient has paralysis of the left vocal cord (right of image); that is, the TA, LCA, and PCA muscles on that side are all affected. Best seen here is evidence of TA weakness (bowing of free margin, loss of left cord bulk especially in the area of the “conus”, and enlarged ventricle). The cord is paramedian, suggesting that the PCA muscle is not working, too. The LCA muscle is hard to evaluate in this view, however.
The explanation becomes more apparent. As will ultimately be seen, this patient has paralysis of the left vocal cord (right of image); that is, the TA, LCA, and PCA muscles on that side are all affected. Best seen here is evidence of TA weakness (bowing of free margin, loss of left cord bulk especially in the area of the “conus”, and enlarged ventricle). The cord is paramedian, suggesting that the PCA muscle is not working, too. The LCA muscle is hard to evaluate in this view, however.
Evidence of LCA weakness (4 of 5)
Phonation in the low chest register (note the wide zone of blurring of the vocal cord’s free margin). Here, the vocal process is clearly seen to turn laterally ( arrow), indicating LCA weakness, in addition to the TA and PCA weakness seen in photo 3.
Phonation in the low chest register (note the wide zone of blurring of the vocal cord’s free margin). Here, the vocal process is clearly seen to turn laterally ( arrow), indicating LCA weakness, in addition to the TA and PCA weakness seen in photo 3.
Phonation at very high pitch (5 of 5)
Phonation at very high pitch (thus, the vibratory blur narrows). The antero-posterior lengthening of the left cord at this high pitch turns the left vocal process back towards the midline (compare with photo 2), masking the LCA weakness. This low voice/high voice difference in the posterior commissure is routinely but not universally seen with LCA weakness.
Phonation at very high pitch (thus, the vibratory blur narrows). The antero-posterior lengthening of the left cord at this high pitch turns the left vocal process back towards the midline (compare with photo 2), masking the LCA weakness. This low voice/high voice difference in the posterior commissure is routinely but not universally seen with LCA weakness.
Vocal Cord Paralysis, Before and After Medialization
Vocal cord paralysis: before medialization (1 of 12)
A classic example of “spaghetti-linguine” vocal cords, here in breathing position. The “linguine” cord (left of image) is normal; the “spaghetti” cord (right of image) is paralyzed, likely since birth. On the paralyzed side, notice the deep and broad ventricle, mild bowing of the margin of the cord, and reduced width of the upper surface of the cord (“spaghetti”-like), as compared with the non-paralyzed side.
A classic example of “spaghetti-linguine” vocal cords, here in breathing position. The “linguine” cord (left of image) is normal; the “spaghetti” cord (right of image) is paralyzed, likely since birth. On the paralyzed side, notice the deep and broad ventricle, mild bowing of the margin of the cord, and reduced width of the upper surface of the cord (“spaghetti”-like), as compared with the non-paralyzed side.
Vocal cord paralysis: before medialization (2 of 12)
Phonation, more distant view, under standard light. Notice the considerable gap between the vocal cords. This gap correlates with the patient’s weak and air-wasting voice quality.
Phonation, more distant view, under standard light. Notice the considerable gap between the vocal cords. This gap correlates with the patient’s weak and air-wasting voice quality.
Vocal cord paralysis: before medialization (3 of 12)
Open phase of vibration, under strobe light. The paralyzed cord (right of image) has a much increased amplitude (lateral or outward excursion) and exaggerated bowing, due to its flaccidity.
Open phase of vibration, under strobe light. The paralyzed cord (right of image) has a much increased amplitude (lateral or outward excursion) and exaggerated bowing, due to its flaccidity.
Vocal cord paralysis: before medialization (4 of 12)
“Closed” phase of vibration, which is of course not closed at all, because the paralyzed cord (right of image) cannot come fully to the midline.
“Closed” phase of vibration, which is of course not closed at all, because the paralyzed cord (right of image) cannot come fully to the midline.
Vocal cord paralysis: 1 week after medialization (5 of 12)
One week after surgical medialization of the paralyzed cord (right of image), using a silastic implant buried deeply within the cord. Notice that the ventricle is no longer capacious, and the free margin is no longer bowed. Furthermore, in contrast with photo 1 of this series, the “spaghetti-linguine” description of these vocal cords is no longer apt.
One week after surgical medialization of the paralyzed cord (right of image), using a silastic implant buried deeply within the cord. Notice that the ventricle is no longer capacious, and the free margin is no longer bowed. Furthermore, in contrast with photo 1 of this series, the “spaghetti-linguine” description of these vocal cords is no longer apt.
Vocal cord paralysis: 1 week after medialization (6 of 12)
Phonation, under standard light. The gap between the cords is no longer seen (compare with photo 2), and the patient’s spontaneous speaking voice sounds normal. She can recruit loudness effectively without any luffing or observable weakness.
Phonation, under standard light. The gap between the cords is no longer seen (compare with photo 2), and the patient’s spontaneous speaking voice sounds normal. She can recruit loudness effectively without any luffing or observable weakness.
Vocal cord paralysis: 1 week after medialization (7 of 12)
Open phase of vibration, under strobe light. The lateral or outward excursion of the paralyzed cord (right of image) is now similar to that of the non-paralyzed cord. Compare with photo 3.
Open phase of vibration, under strobe light. The lateral or outward excursion of the paralyzed cord (right of image) is now similar to that of the non-paralyzed cord. Compare with photo 3.
Vocal cord paralysis: 1 week after medialization (8 of 12)
The closed phase of vibration is much more closed than preoperatively. Compare with photo 4.
Phonation, under standard light, showing vibratory blur. Compare with photos 2 and 6 of this series.
Vocal cord paralysis: 5 months after medialization (11 of 12)
Open phase of vibration, under strobe light. As in photo 7 of this series, and in contrast to photo 3, the implant does not permit the paralyzed cord (right of image) to “buckle” laterally, or outward. If anything, the vibratory excursion of the non-paralyzed (and un-implanted) cord is greater than that of the paralyzed, implanted cord.
Open phase of vibration, under strobe light. As in photo 7 of this series, and in contrast to photo 3, the implant does not permit the paralyzed cord (right of image) to “buckle” laterally, or outward. If anything, the vibratory excursion of the non-paralyzed (and un-implanted) cord is greater than that of the paralyzed, implanted cord.
Vocal cord paralysis: 5 months after medialization (12 of 12
The closed phase of vibration is now virtually normal, similar to photo 8 and in contrast with photo 4.
The closed phase of vibration is now virtually normal, similar to photo 8 and in contrast with photo 4.
Extrusion of Vocal Cord Implant
Extrusion of vocal cord implant (1 of 3)
Patient with a paralyzed left vocal cord (right of image), who several years ago had successful medialization of that cord with a silastic wedge. More recently, several months ago, she noticed pain and swelling during some intense aerobic activity and then a persistently roughened voice quality. This view shows that the left cord is inflamed.
Patient with a paralyzed left vocal cord (right of image), who several years ago had successful medialization of that cord with a silastic wedge. More recently, several months ago, she noticed pain and swelling during some intense aerobic activity and then a persistently roughened voice quality. This view shows that the left cord is inflamed.
Extrusion of vocal cord implant (2 of 3)
Strobe lighting. Note the convex shape of the left cord’s anterior end (the lower end, in this photo). This convexity is not caused by over-medialization, but instead by the inflammatory reaction.
Strobe lighting. Note the convex shape of the left cord’s anterior end (the lower end, in this photo). This convexity is not caused by over-medialization, but instead by the inflammatory reaction.
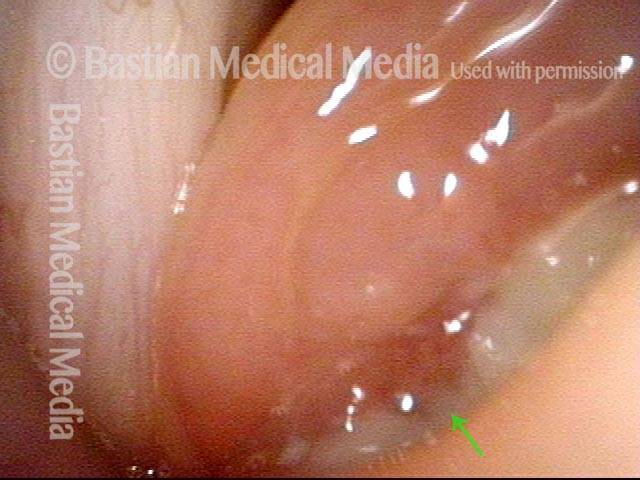
Extrusion of vocal cord implant (3 of 3)
Closer view shows that the problem is exposure of the silastic implant. The actual silastic is bare at the arrow. Whitish exudate covers the remaining exposed implant. This is a rare event after medialization with a silastic implant.
Closer view shows that the problem is exposure of the silastic implant. The actual silastic is bare at the arrow. Whitish exudate covers the remaining exposed implant. This is a rare event after medialization with a silastic implant.
Voice Gel for Immediate Help
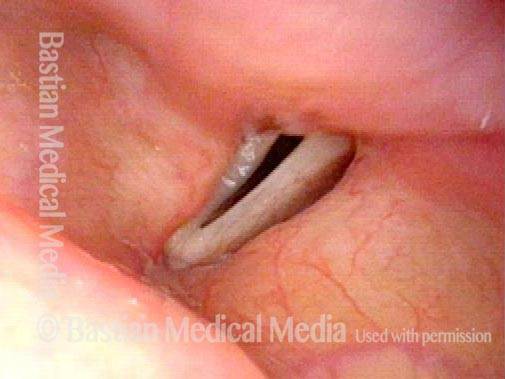
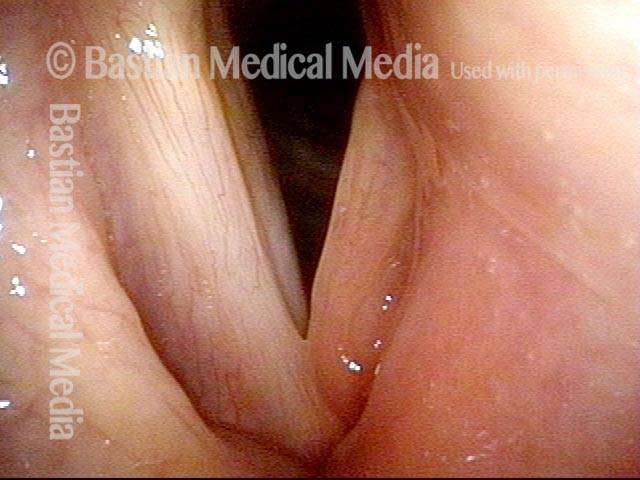
Paralysis of left vocal cord (1 of 4)
An older man with left vocal cord paralysis (right of photo) after chest surgery involving the upper mediastinum. This is maximum adduction at the prephonatory instant showing bowing and atrophy of the left cord (right of photo). Voice is exceedingly weak and air-wasting.
An older man with left vocal cord paralysis (right of photo) after chest surgery involving the upper mediastinum. This is maximum adduction at the prephonatory instant showing bowing and atrophy of the left cord (right of photo). Voice is exceedingly weak and air-wasting.
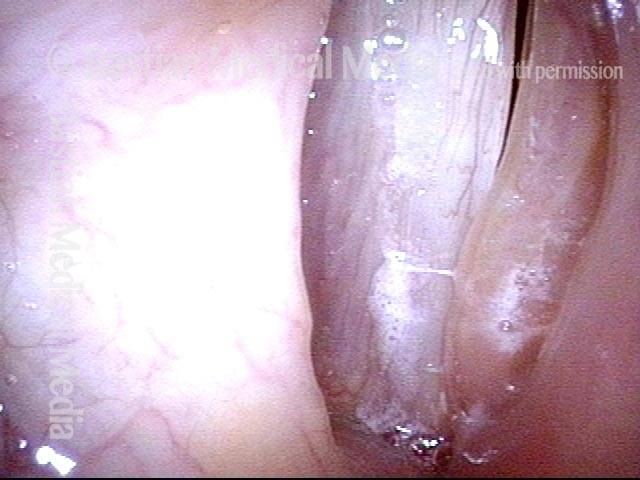
Vocal gel injection (2 of 4)
At the beginning of voice gel injection in a voice lab, with the patient sitting in an examination chair. The trajectory of the 27-gauge needle is indicated with the dotted line. A second bolus of gel will be injected farther posteriorly.
At the beginning of voice gel injection in a voice lab, with the patient sitting in an examination chair. The trajectory of the 27-gauge needle is indicated with the dotted line. A second bolus of gel will be injected farther posteriorly.
Cord closer to midline (3 of 4)
At the conclusion of the injection, the left cord has been plumped up and also shifted towards the midline.
At the conclusion of the injection, the left cord has been plumped up and also shifted towards the midline.
Complete adduction of cords (4 of 4)
The vocal cords can close completely now for voice production. Voice is dramatically stronger and the patient can say many more words on a breath before running out of air.
The vocal cords can close completely now for voice production. Voice is dramatically stronger and the patient can say many more words on a breath before running out of air.
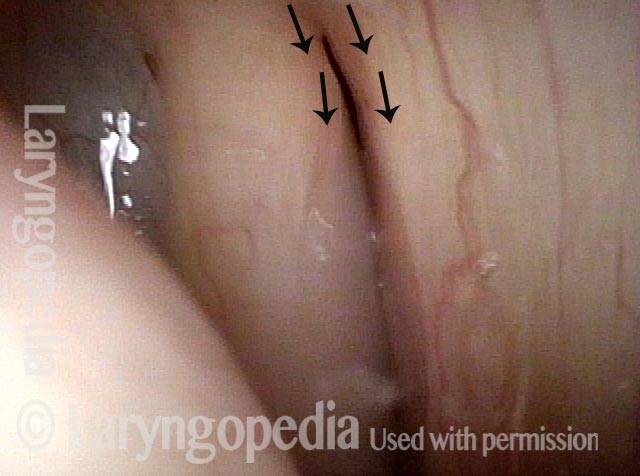
TA + PCA-only Paresis
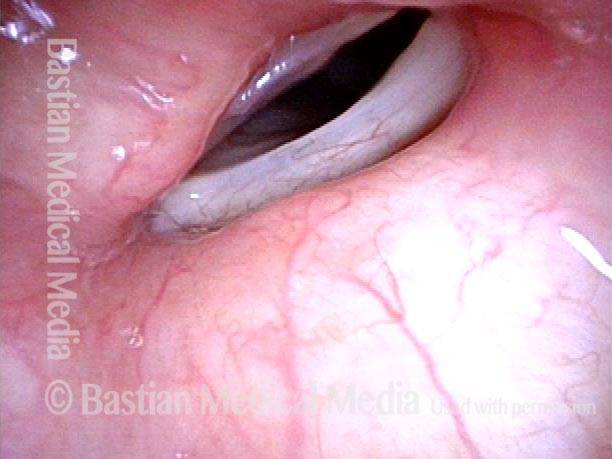
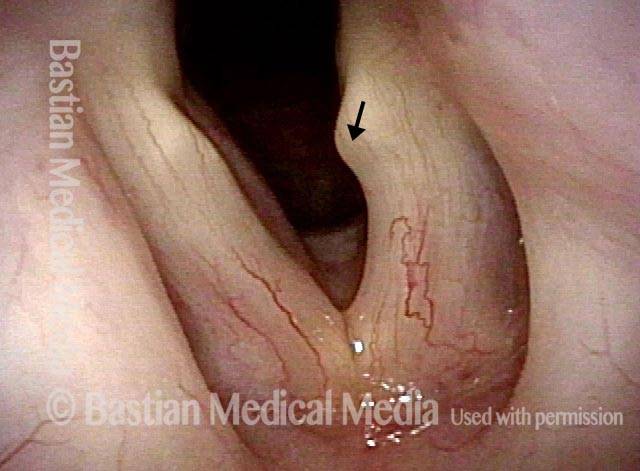
Breathing position (1 of 5)
Abducted (breathing) position, shows the bowed contour of the left cord (right of photo), and loss of mass due to wasting of muscle within the cord. The left vocal process points medially ( see arrow), suggesting that the LCA muscle is still active.
Abducted (breathing) position, shows the bowed contour of the left cord (right of photo), and loss of mass due to wasting of muscle within the cord. The left vocal process points medially ( see arrow), suggesting that the LCA muscle is still active.
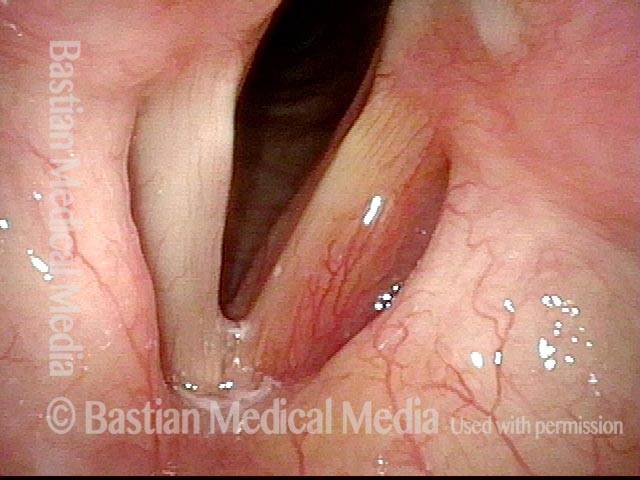
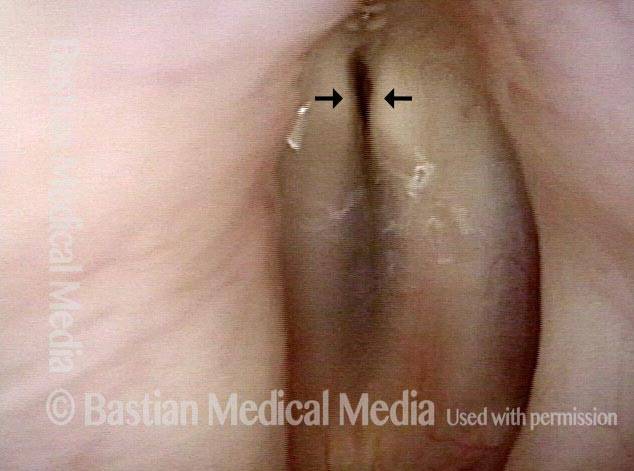
Phonatory position (2 of 5)
During attempted phonation, note the gap (see arrows) that remains between the cords, accounting for her breathiness. In this view, vocal processes are reasonably antero-posterior in orientation, again suggesting good LCA function. In addition, note the lateral buckling of the left cord (right of photo), due to its flaccidity.
During attempted phonation, note the gap (see arrows) that remains between the cords, accounting for her breathiness. In this view, vocal processes are reasonably antero-posterior in orientation, again suggesting good LCA function. In addition, note the lateral buckling of the left cord (right of photo), due to its flaccidity.
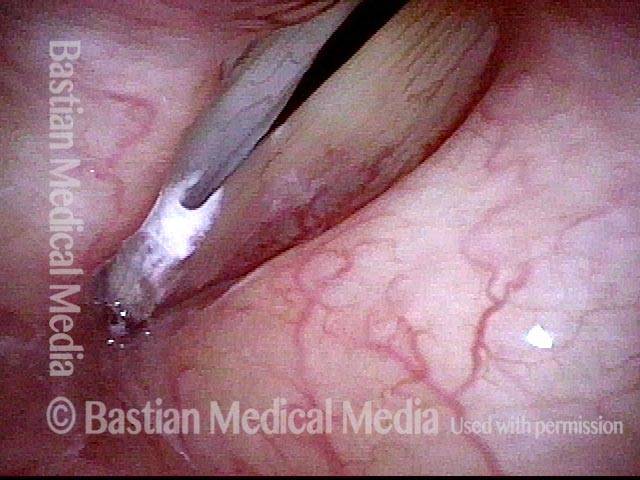
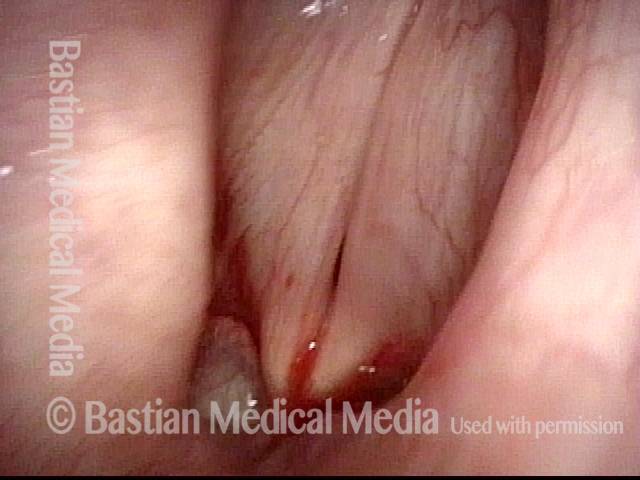
Voice gel injection (3 of 5)
At the moment just before voice gel injection into this flaccid cord. Blood is due to the cricothyroid membrane puncture moments before, for the purpose of providing topical anesthesia.
At the moment just before voice gel injection into this flaccid cord. Blood is due to the cricothyroid membrane puncture moments before, for the purpose of providing topical anesthesia.
Plumped vocal cord (4 of 5)
Needle hub pulls the false cord laterally and true vocal cord is noticeably plumped up by the gel.
Needle hub pulls the false cord laterally and true vocal cord is noticeably plumped up by the gel.
After voice gel injection (5 of 5)
Phonation, immediately after voice gel injection. Notice that the vocal cords come into much better contact. Voice is correspondingly dramatically improved.
Phonation, immediately after voice gel injection. Notice that the vocal cords come into much better contact. Voice is correspondingly dramatically improved.
55 Years of Paralysis with Every Classic Finding
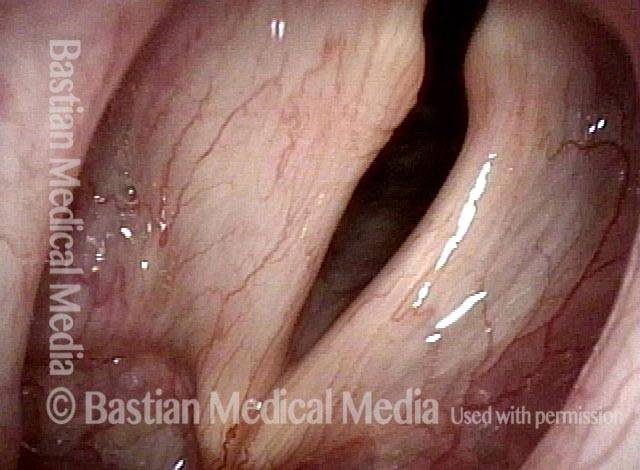
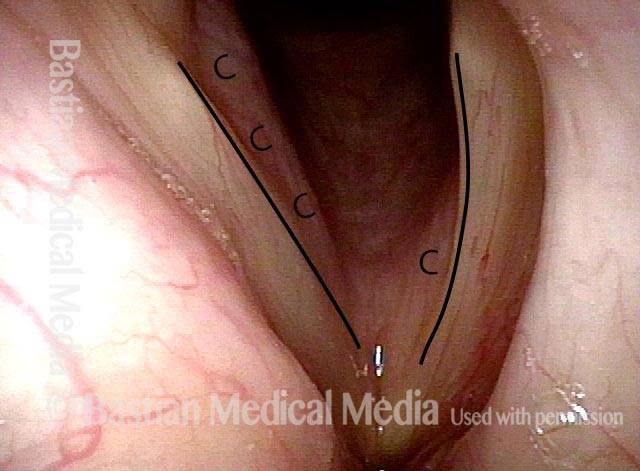
Breathing position, bowed left cord (1 of 4)
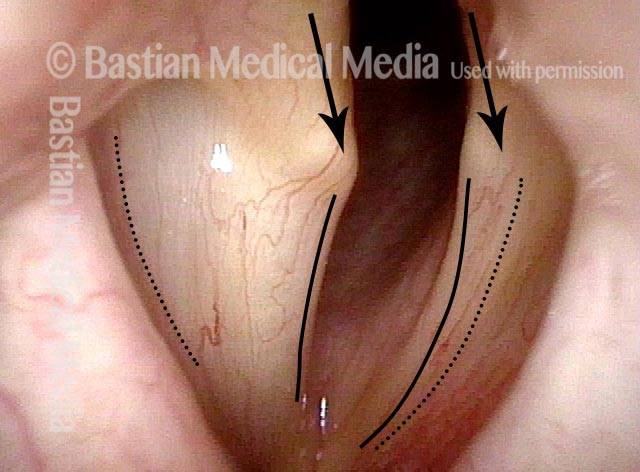
Drastically weak voice since age 21 in a man now in his upper seventies. Breathing position. The normal right cord (left of photo) is fully lateralized, has a relatively straight margin (see line) and conus muscle bulge (pinker undersurface of cord marked by “C”) is fairly full. The abnormal left cord (right of photo) is paramedian (slightly lateral to midline), bowed (see line), and its conus muscle bulge practically nonexistent (marked by “C”).
Drastically weak voice since age 21 in a man now in his upper seventies. Breathing position. The normal right cord (left of photo) is fully lateralized, has a relatively straight margin (see line) and conus muscle bulge (pinker undersurface of cord marked by “C”) is fairly full. The abnormal left cord (right of photo) is paramedian (slightly lateral to midline), bowed (see line), and its conus muscle bulge practically nonexistent (marked by “C”).
Approaching voicing position (2 of 4)
Approaching voicing position under standard light. Right cord (left of photo) has come almost to midline. Vocal process points slightly medially (arrow). Left cord (right of photo) shows lateral pointing of vocal process (arrow), bowed margin (see line), and its ventricle is capacious. Ventricle extends laterally from dotted line on each cord.
Approaching voicing position under standard light. Right cord (left of photo) has come almost to midline. Vocal process points slightly medially (arrow). Left cord (right of photo) shows lateral pointing of vocal process (arrow), bowed margin (see line), and its ventricle is capacious. Ventricle extends laterally from dotted line on each cord.
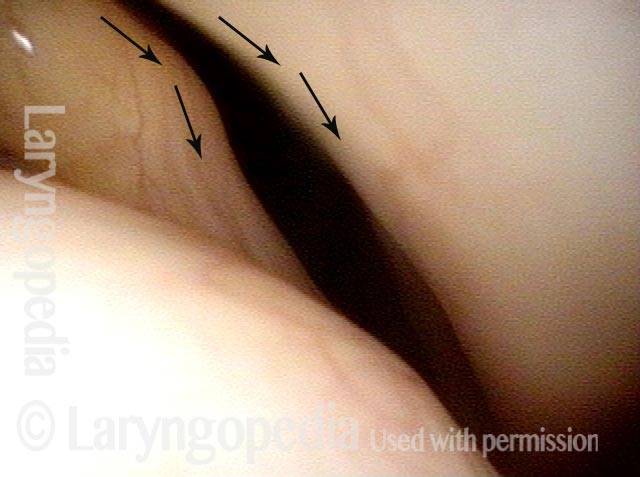
Vocal cord closure, large gap (3 of 4)
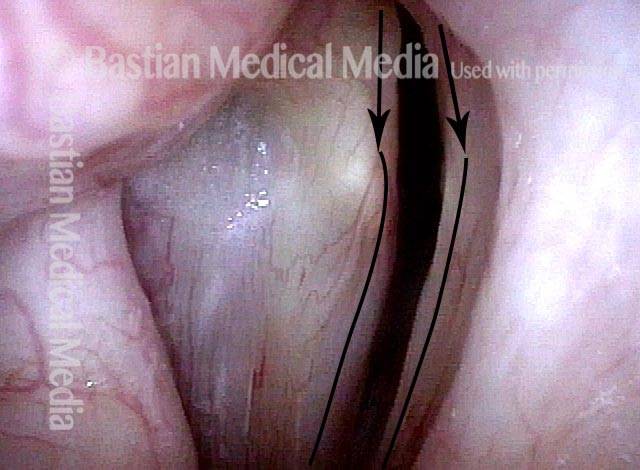
Voicing under strobe light, at maximum vibratory closure. Large gap explains major air-wasting dysphonia. Note directionality of vocal processes that appear to indicate LCA is working on the right (left of photo), and is not on the left (right of photo); note also the bowing of the left cord (right of photo).
Voicing under strobe light, at maximum vibratory closure. Large gap explains major air-wasting dysphonia. Note directionality of vocal processes that appear to indicate LCA is working on the right (left of photo), and is not on the left (right of photo); note also the bowing of the left cord (right of photo).
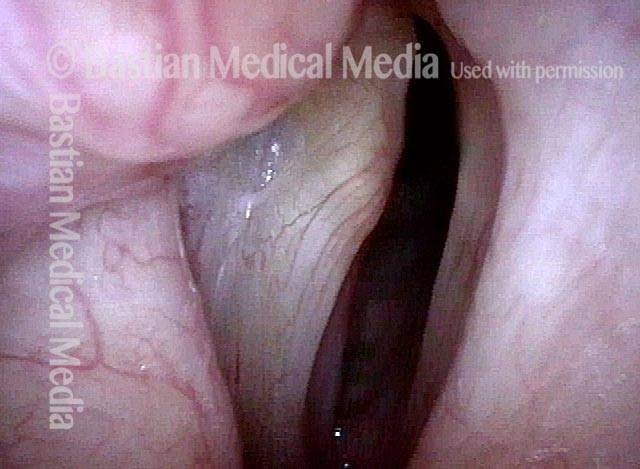
Open phase of vibration, flaccidity of right cord (4 of 4)
Open phase of vibration shows what appears to be flaccidity (very large lateral excursion) of the right (neurologically intact) cord (left of photo). Flaccidity in working cord is often seen: the question is whether that is functionally “necessary” to allow vibration. I.E. would a normally tensed cord fail to oscillate with so little “grip” of the airstream? Or is it flaccid due to age and lack of a working partner to help keep it strong?
Open phase of vibration shows what appears to be flaccidity (very large lateral excursion) of the right (neurologically intact) cord (left of photo). Flaccidity in working cord is often seen: the question is whether that is functionally “necessary” to allow vibration. I.E. would a normally tensed cord fail to oscillate with so little “grip” of the airstream? Or is it flaccid due to age and lack of a working partner to help keep it strong?
Medialization Laryngoplasty Typically Doesn’t Fix the LCA “Finding.”
Left vocal cord paralysis (1 of 4)
Many years after treatment for lung cancer, this man’s voice has abruptly weakened. Here we see left vocal cord paralysis (right of photo). The most striking finding (of several) in this view is the margin bowing of the left cord (compare dotted lines, right of photo).
Many years after treatment for lung cancer, this man’s voice has abruptly weakened. Here we see left vocal cord paralysis (right of photo). The most striking finding (of several) in this view is the margin bowing of the left cord (compare dotted lines, right of photo).
Bowing during phonation (2 of 4)
During phonation, the right vocal process (left of photo) turns medially due to intact LCA; on the left (right of photo), with LCA paralyzed, the vocal process turns laterally (compare posterior arrows).
During phonation, the right vocal process (left of photo) turns medially due to intact LCA; on the left (right of photo), with LCA paralyzed, the vocal process turns laterally (compare posterior arrows).
After medialization (3 of 4)
A few months after medialization (an implant placed deep inside the left vocal cord), the left vocal cord margin is now straight rather than bowed (compare with photo 1).
A few months after medialization (an implant placed deep inside the left vocal cord), the left vocal cord margin is now straight rather than bowed (compare with photo 1).
Lateral turning remains unchanged (4 of 4)
During phonation, a striking change is the diminished gap between the cords, and this explains his much stronger voice. The lateral turning of the left vocal process (right of photo) is still seen, however. Medialization tends to “fix” the flaccidity and lateralization of the paralyzed vocal cord, and to reduce the gap between the cord. Compare with photo 2. As seen here, the lateral turning of the vocal process is still seen to some degree. If the voice were not so good and satisfying to the patient, this visual finding would be an argument for arytenoid adduction.
During phonation, a striking change is the diminished gap between the cords, and this explains his much stronger voice. The lateral turning of the left vocal process (right of photo) is still seen, however. Medialization tends to “fix” the flaccidity and lateralization of the paralyzed vocal cord, and to reduce the gap between the cord. Compare with photo 2. As seen here, the lateral turning of the vocal process is still seen to some degree. If the voice were not so good and satisfying to the patient, this visual finding would be an argument for arytenoid adduction.
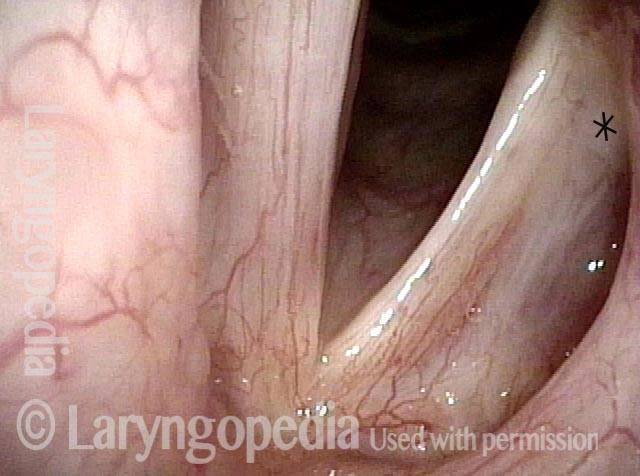
Voice Gel Injection for Vocal Cord Paralysis
Left vocal cord paralysis (1 of 4)
This photo shows left vocal cord paralysis in the breathing position. Note the margin bowing, “spaghetti-linguini” difference in bulk, and capacious ventricle. Note: the * is for comparison with photo 3.
This photo shows left vocal cord paralysis in the breathing position. Note the margin bowing, “spaghetti-linguini” difference in bulk, and capacious ventricle. Note: the * is for comparison with photo 3.
Voice-making position (2 of 4)
Here the paralysis is shown in the voice-making position. Note the lateral buckling of the left vocal cord (right of photo). This flaccidity and the gap between the vocal cords explain the patient’s breathy (air-wasting) voice quality.
Here the paralysis is shown in the voice-making position. Note the lateral buckling of the left vocal cord (right of photo). This flaccidity and the gap between the vocal cords explain the patient’s breathy (air-wasting) voice quality.
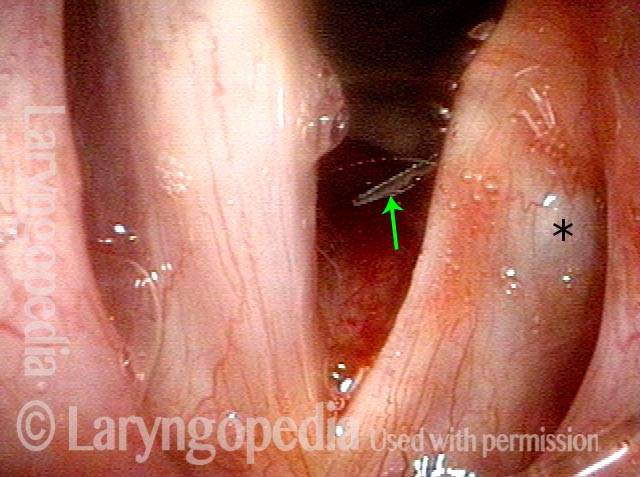
Voice gel injection (3 of 4)
This is the same patient at the beginning of voice gel injection. Needle at arrow coming from subglottis upwards and laterally. At * one can see the beginning of bulging in the posterior ventricle. The vocal cord also looks slightly shifted towards the midline. Compare with photo 1.
This is the same patient at the beginning of voice gel injection. Needle at arrow coming from subglottis upwards and laterally. At * one can see the beginning of bulging in the posterior ventricle. The vocal cord also looks slightly shifted towards the midline. Compare with photo 1.
After voice gel injection (4 of 4)
Voice-making position after voice gel injection is complete and bulge in ventricle at * is more evident. Closure is much better; the voice is dramatically stronger and the air-wasting quality much less. Compare with photo 2.
Voice-making position after voice gel injection is complete and bulge in ventricle at * is more evident. Closure is much better; the voice is dramatically stronger and the air-wasting quality much less. Compare with photo 2.
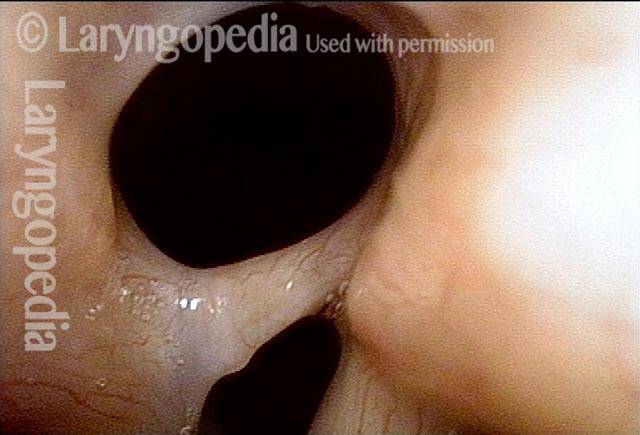
Posterior Commissure Synechiae
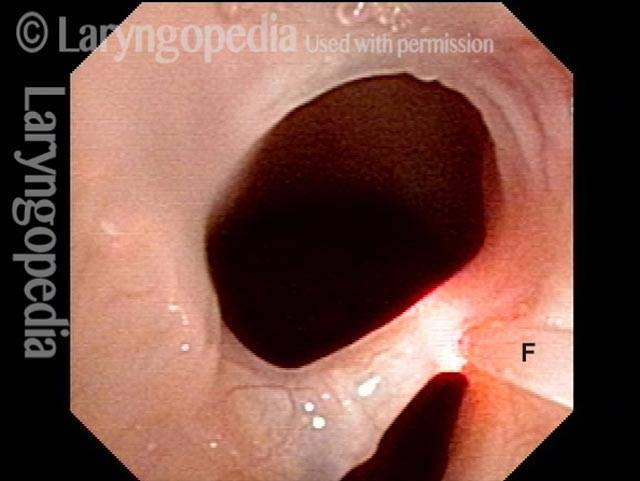
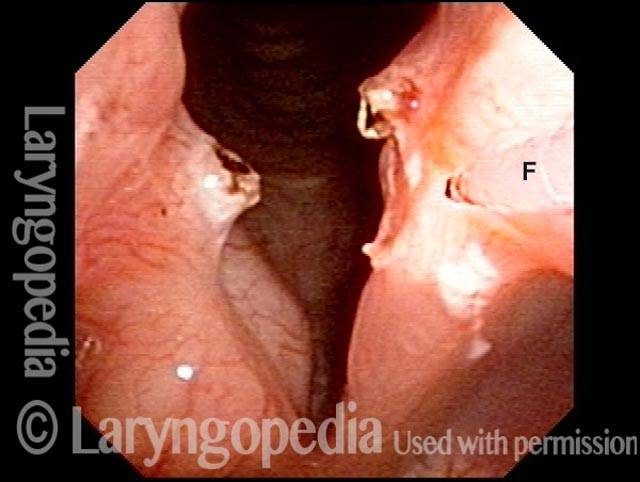
Tethered vocal cords (1 of 5)
This man has right vocal cord paralysis and a history decades ago of Teflon injection into the right vocal cord, resulting in posterior commissure synechiae. He is short of breath, partly due to the tissue band and partly because it tethers the vocal cords closer together than they would otherwise need to be as seen in photo 4 after the band is removed. See also photo 5.
This man has right vocal cord paralysis and a history decades ago of Teflon injection into the right vocal cord, resulting in posterior commissure synechiae. He is short of breath, partly due to the tissue band and partly because it tethers the vocal cords closer together than they would otherwise need to be as seen in photo 4 after the band is removed. See also photo 5.
A month later, no residue of the synechiae is seen, and the vocal cords can spring farther apart than in photo 1.
Play Video
Injection Medialization for Vocal Fold Paresis
See an example of one variant of vocal fold paresis and how it limits the voice. Then watch a medialization procedure in which voice gel is injected into the vocal fold affected by paresis, and hear how the voice thereafter improves.