Bilateral vocal cord paralysis is a neurological disorder in which the nerve supply to both vocal cords is absent. This may be as the result of injury through external trauma, thyroid surgery, or blunt or penetrating trauma to the neck. Sometimes vocal cord immobility due to scarring—from an endotracheal tube, for instance—is mistaken for vocal cord paralysis, though the distinction is usually easy to determine, provided that an appropriately intense and directed workup is done. In particular, this workup must include topical anesthesia to the larynx so as to enable an extremely close visualization of the posterior commissure and subglottis, which may uncover evidence of scarring.
See also: intubation injury, stenosis, vocal cord synechia, and vocal cord paralysis, unilateral.
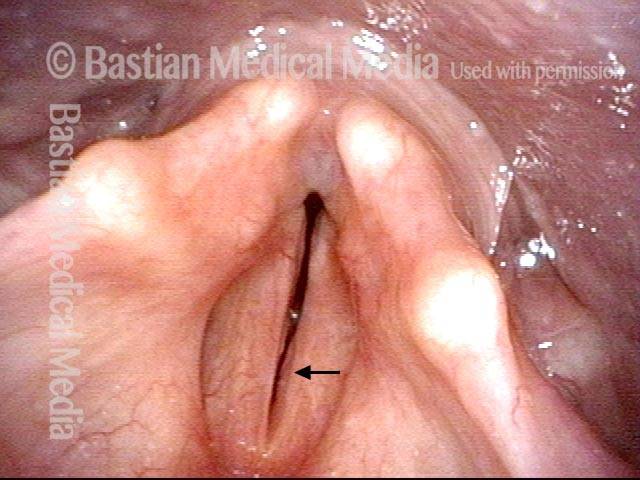
Bilateral Vocal Cord Paralysis
Maximum space between cords (1 of 2)

View during inhalation (2 of 2)
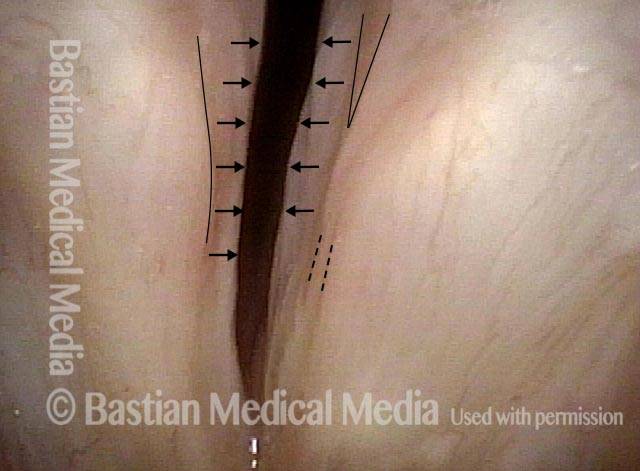
Mucosal Indrawing with Inspiration
Paralyzed vocal cord (1 of 2)

Indrawing with inspiration (2 of 2)