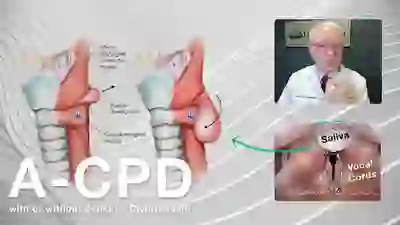
Antegrade cricopharyngeal dysfunction (A-CPD) is the failure of the tonically contracted upper esophageal sphincter to relax and open when one swallows. It is also known as cricopharyngeal achalasia. The cause is usually unknown.
The upper esophageal sphincter is also known as the cricopharyngeus muscle and is located at the lower level of the voicebox or larynx. This muscle is always contracted except at the moment of swallowing, when it relaxes briefly to let food or liquid pass through.
Symptoms and treatment for A-CPD
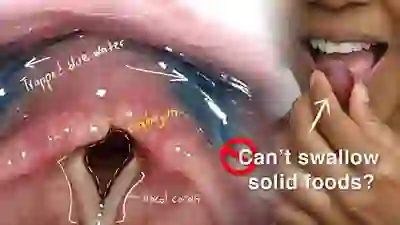
Typically, individuals with A-CPD first notice that pills or solid food begin to lodge at the level of the lower part of the larynx. The problem tends to progress inexorably, though often slowly, as the years pass, until the individual must limit himself or herself to liquid and soft foods.
Cricopharyngeal dysfunction is fully resolved through a straightforward surgical procedure (cricopharyngeal myotomy), performed through the mouth with the laser or, only occasionally, through a neck incision.
See also: Zenker’s diverticulum.
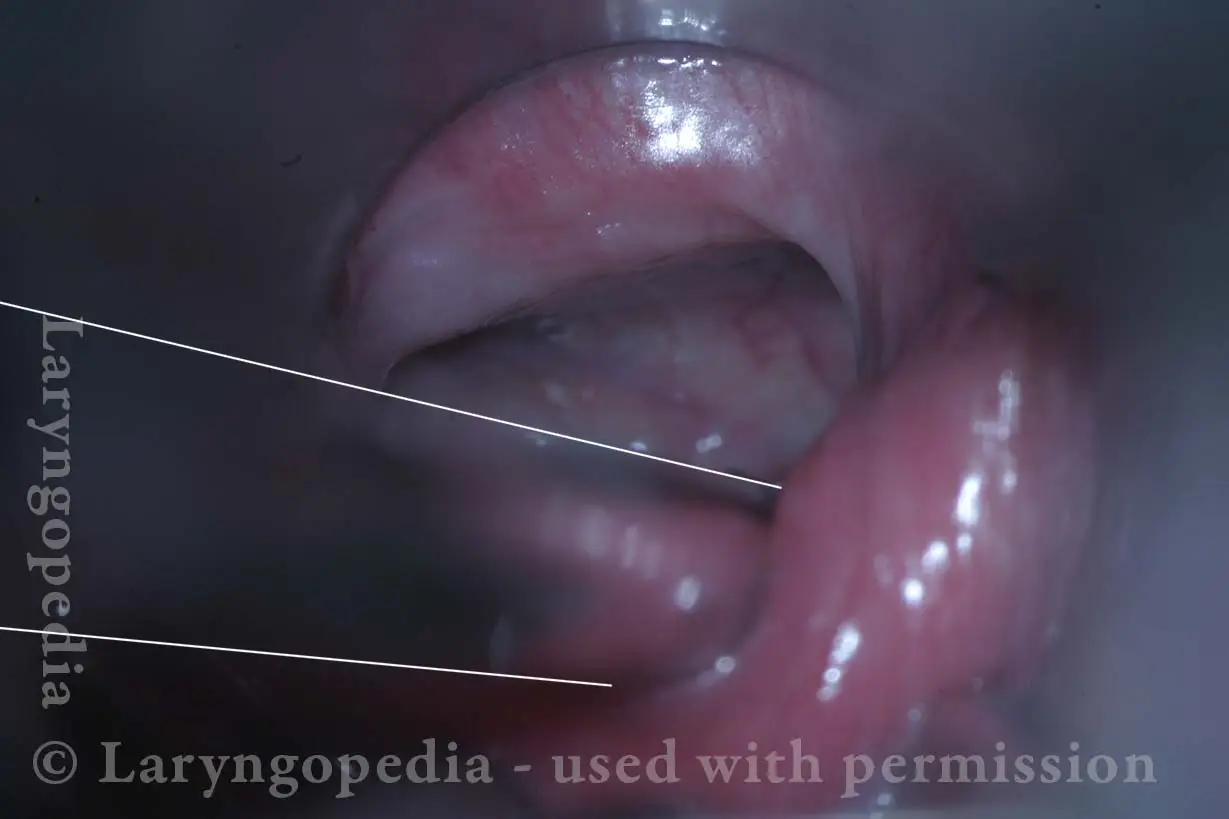
A-CPD, before, during, and after Myotomy.
Non-relaxing cricopharyngeus muscle (1 of 4)

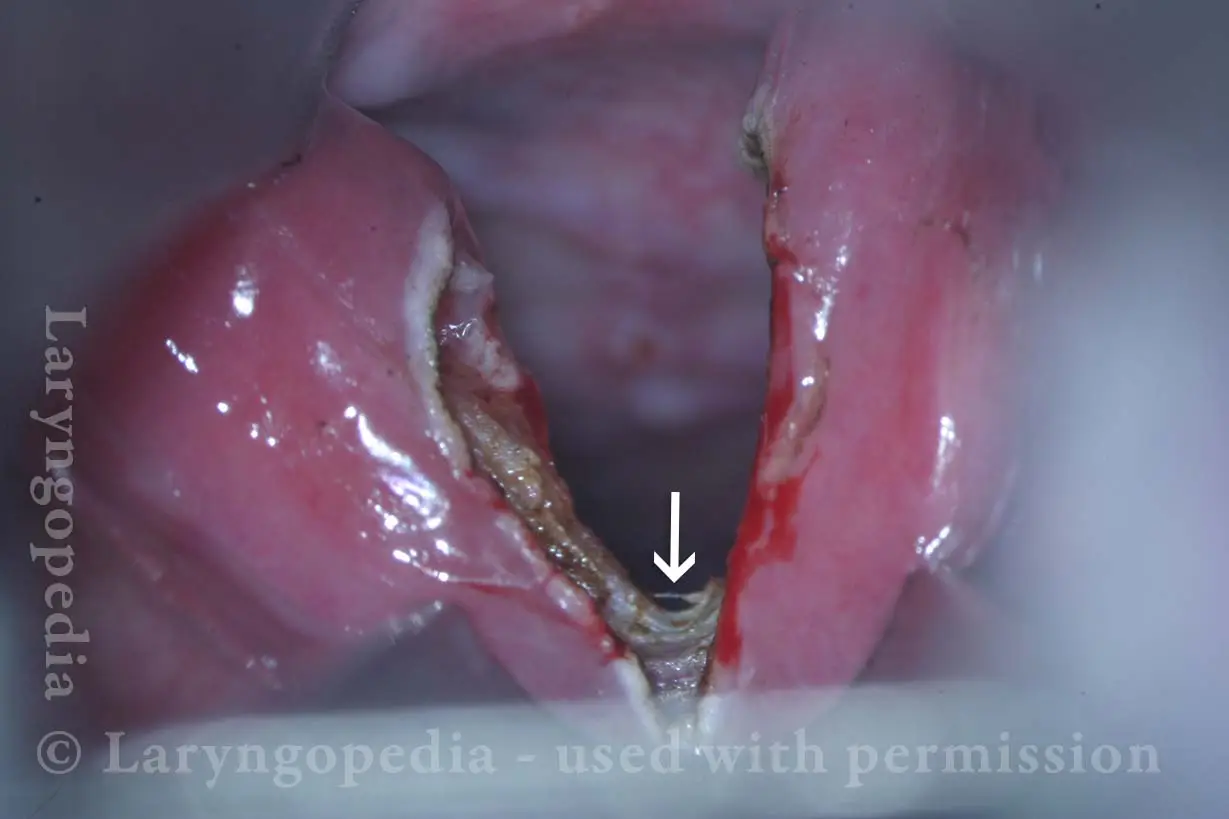
Opening the esophageal orifice (2 of 4)
Laser cricopharyngeus myotomy (3 of 4)

Cricopharyngeus myotomy nearly complete (4 of 4)
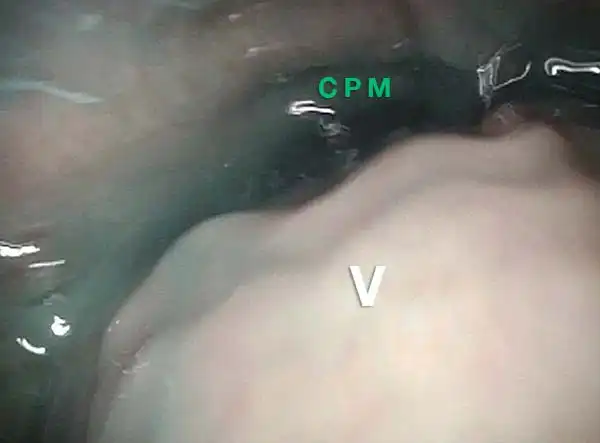
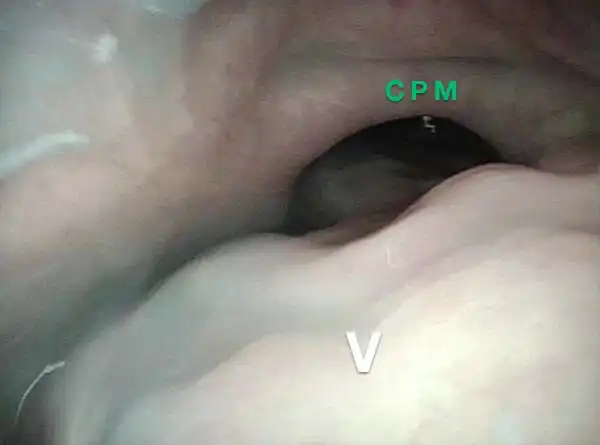
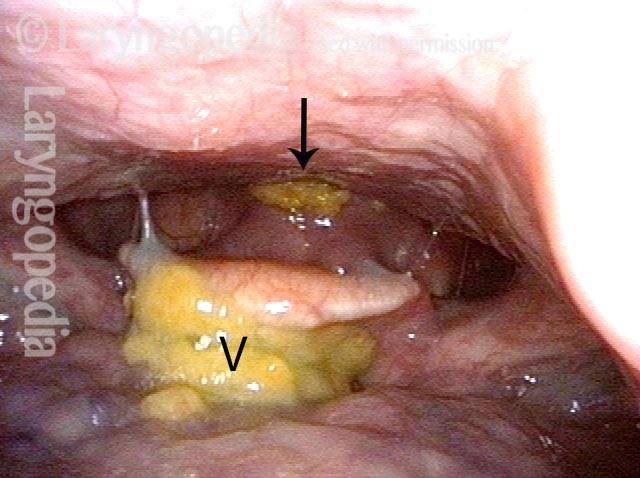
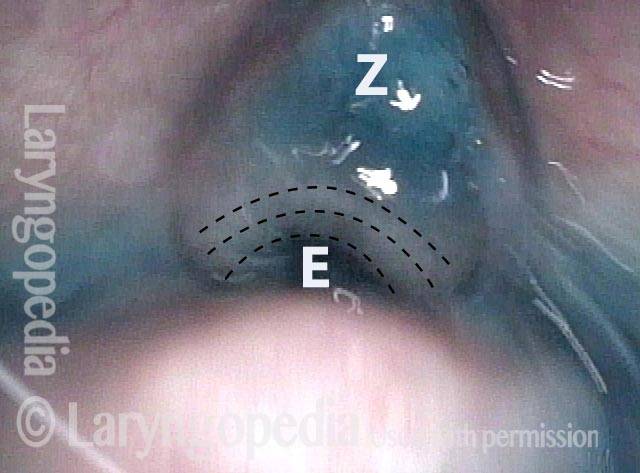
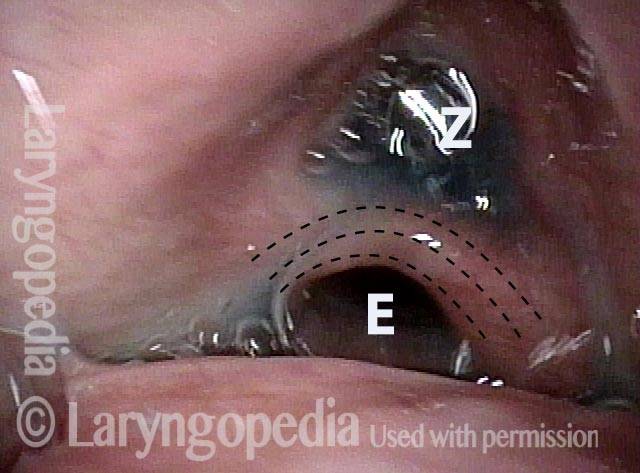
The Cricopharyngeus Muscle Seen During Swallowing
This person struggles to swallow due to a combination of prior tongue cancer surgery decades ago, and longterm radiation effects. Solid foods are the most problematic, and so this sequence shows an attempt to swallow water stained with blue food coloring.
Swallowing crescent (1 of 5)
Swallowing water (2 of 5)
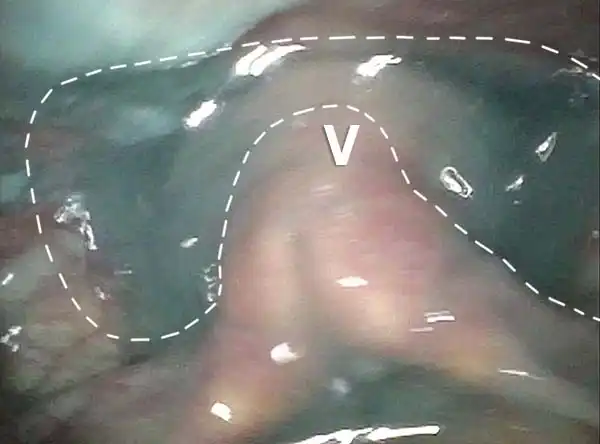
Cricopharyngeus muscle (3 of 5)
Relaxed CPM (4 of 5)

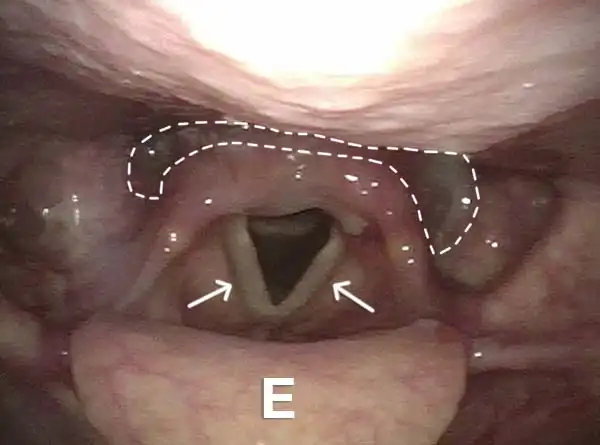
Partially open esophagus due to A-CPD (5 of 5)
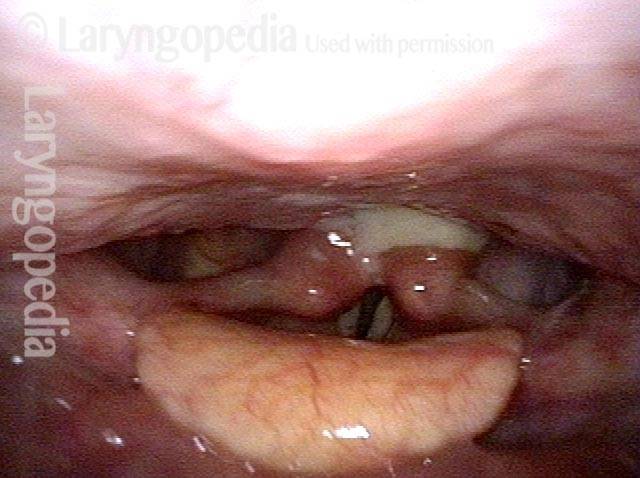
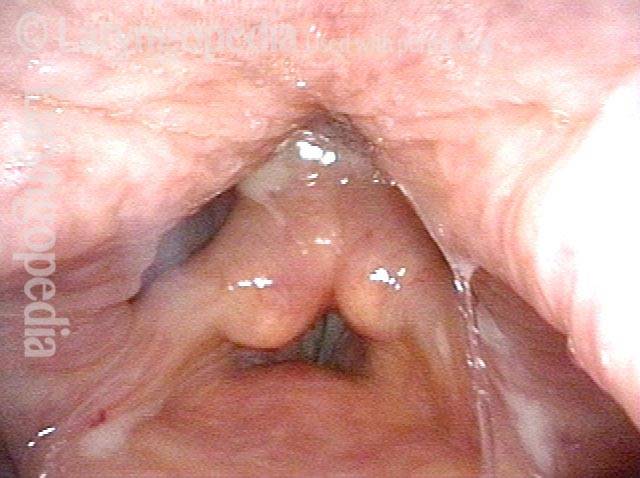
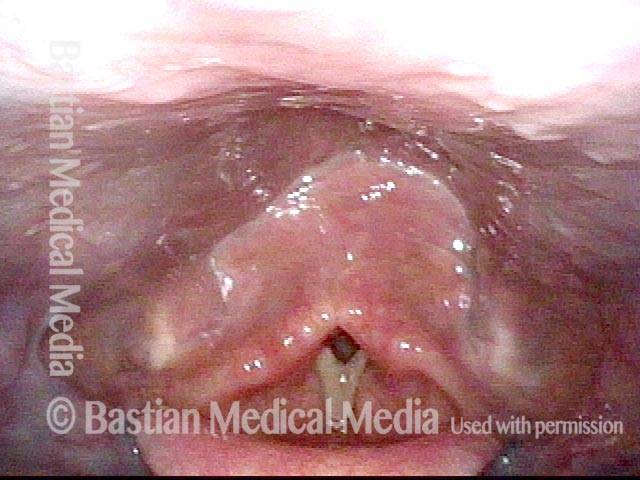
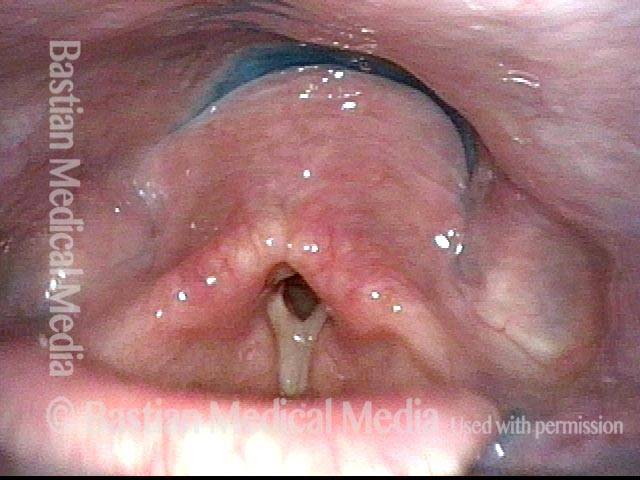
Antegrade Cricopharyngeal Dysfunction, Before and After Myotomy
Cricopharyngeal dysfunction: before myotomy (1 of 2)

Cricopharyngeal dysfunction: after myotomy, resolved (2 of 2)

Example 2
Cricopharyngeal dysfunction: before myotomy (1 of 2)

Cricopharyngeal dysfunction: after myotomy, resolved (1 of 2)

Very High-pitched Voice Elicits the Same Pharynx Contraction as Swallowing
Secretions (1 of 4)
Contracted pharynx (2 of 4)
Cracker residue (3 of 4)
Pharyngeal walls (4 of 4)
Reflux Into Hypopharynx, Characteristic of Antegrade Cricopharyngeal Dysfunction
Reflux into hypopharynx (1 of 3)
Water flows into the swallowing crescent (2 of 3)
Larynx opens up (3 of 3)

Cricopharyngeus Non-Relaxation and Zenker’s Sac Seen During VESS
Immediately after swallow (1 of 4)

One second later (2 of 4

Un-relaxed cricopharyngeus muscle (3 of 4)
More water (4 of 4)
{kind=link}