Food lodgment refers to when food gets stuck somewhere along its path from lips to stomach. Lodgment is more of a “full stop” of the food’s digestive journey, as compared with pooling. Lodgment usually occurs at one of these points: in the vallecula (usually in cases of presbyphagia); at the level of the cricopharyngeus muscle (in cases of cricopharyngeal dysfunction, which is one kind of achalasia); somewhere in the esophagus (in cases of esophageal stenosis); or at the lower esophageal sphincter (in cases of lower esophageal sphincter achalasia).
VESS Assesses Equipment, Secretions, then Swallowing Ability
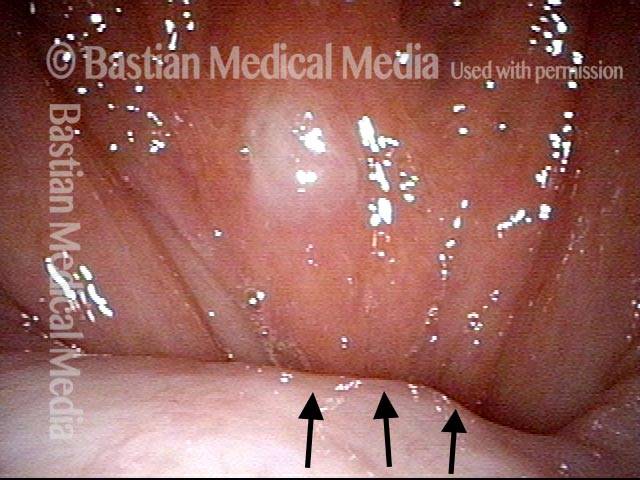
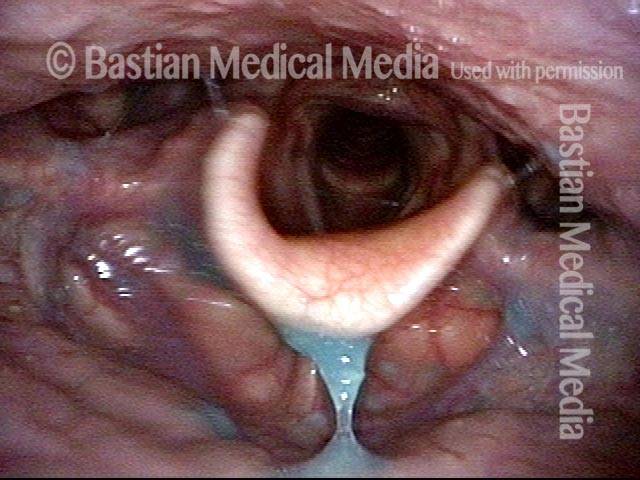
Part Ia: Palate elevates normally (1 of 7)
This man has symptoms of cricopharyngeus muscle dysfunction (CPD), with frequent lodgment of solid food (never soft or liquid material) at the level of mid-to-low neck. This VESS sequence demonstrates his propulsive or “pitcher” ability. Here in VESS part Ia, palate elevates normally (arrows). Left palate is not drooping and there is no deviation.
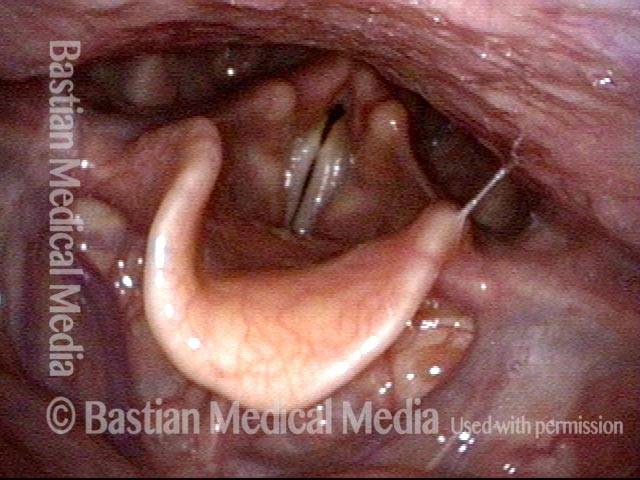
Part Ib: phonation (2 of 7)
In Part Ib of VESS, the patient makes voice, to prove normal movement and good closure of the vocal cords. In addition, no secretional pooling is seen in vallecula or pyriform sinuses.
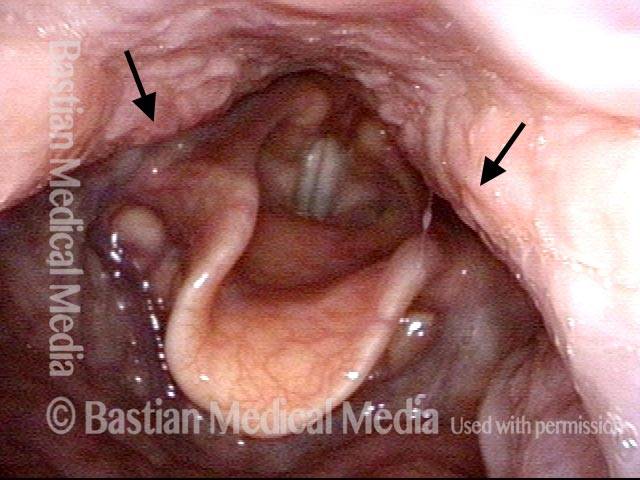
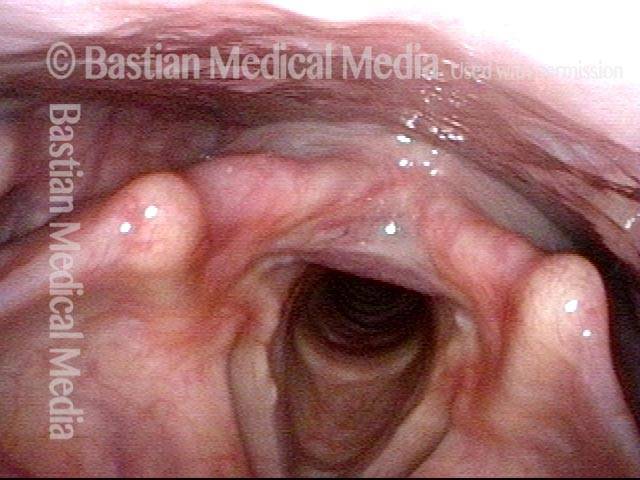
Part Ic: High pitch elicited (3 of 7)
Part Ic: Very high pitch is elicited. Pharyngeal walls contract inward (arrows), closing the pyriform sinuses. Part Ia,b, and c (Photos 1, 2, and 3) verify that there is good function of swallowing equipment, i.e. palate, pharynx, and larynx (and tongue).
Part IIa: applesauce (4 of 7)
Part IIa: Blue-stained applesauce is first, because puree is the “easiest” material for the majority of patients, whatever their diagnosis. Here, one sees only minimal residue after several boluses are swallowed.
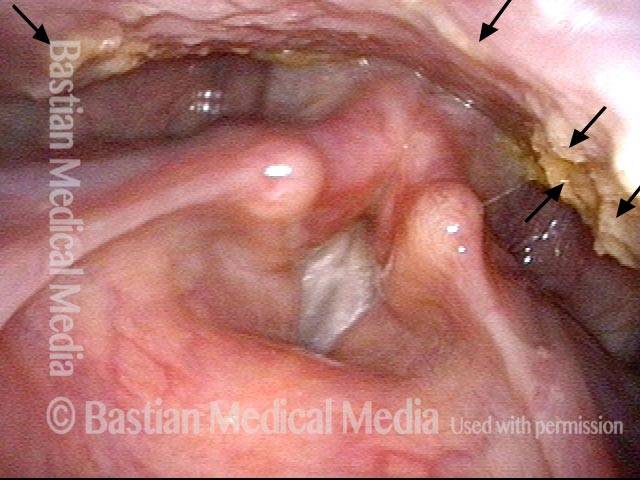
Part IIb: cracker (5 of 7)
Part IIb: After an orange (cheese) cracker, lodgment in the vallecula, and…

Part IIb: continued (6 of 7)
...on the pharyngeal walls (arrows).
Part IIc: water (7 of 7)
Part IIc: After several boluses of blue-stained water, all cracker is washed away and there is no blue staining or residue within the laryngeal vestibule, subglottis, or high trachea. Given this man’s CPD symptoms, VFSS may show a cricopharyngeus muscle bar, indicating incomplete relaxation of the upper esophageal sphincter.
Cricopharyngeal Dysfunction, before and after Myotomy
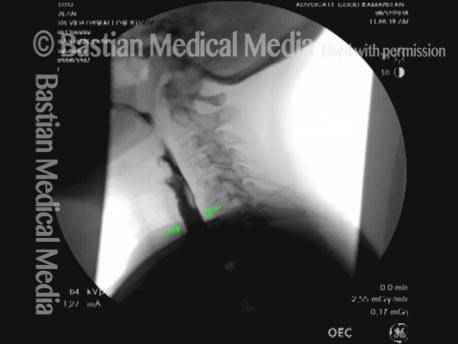
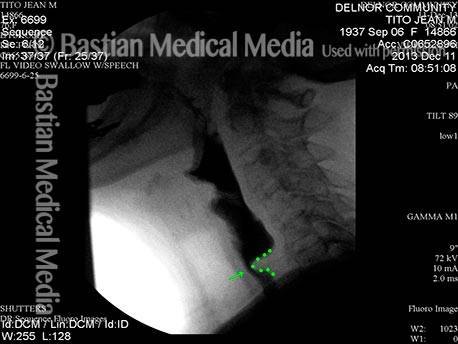
Cricopharyngeal dysfunction: before myotomy (1 of 2)
Elderly patient with nearly a year’s duration of frequent lodgment of solid food at the level of the cricoid cartilage (at the mid-neck level). Note here the cricopharyngeus muscle “bar” which narrows the barium stream (indicated by green dotted line). This narrowing is due to incomplete relaxation of the muscle (aka upper esophageal sphincter) causing a smaller entrance to the esophagus. Liquids and very soft foods can still get through, but solid foods tend to get stuck or to require repeated swallows.
Cricopharyngeal dysfunction: after myotomy (2 of 2)
A month after endoscopic (through the mouth) cricopharyngeus myotomy (division of the muscle with a laser). The patient’s initial swallowing symptoms are completely resolved and the barium stream no longer shows narrowing and the cricopharyngeus bar is no longer seen (see green arrows).