Come è la voce dopo il trattamento?
Effetto dei noduli corde vocali sulla voce, PRIMA della rimozione chirurgica (vedere le foto di questo paziente appena sotto):
Stesso paziente, sette settimane DOPO la rimozione chirurgica dei noduli corde vocali:
Noduli corde vocali, prima e dopo l’intervento chirurgico
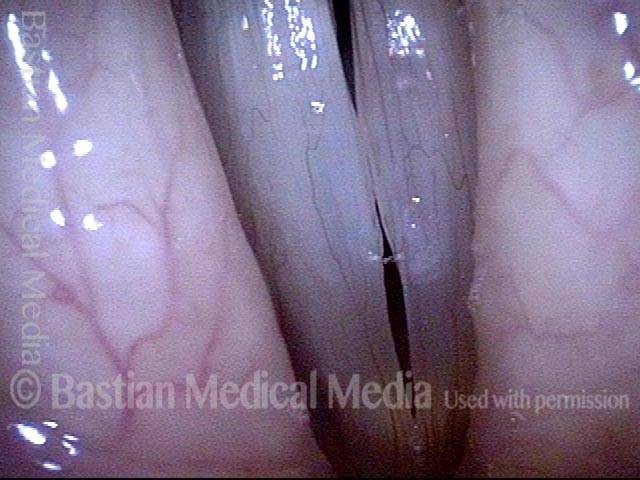
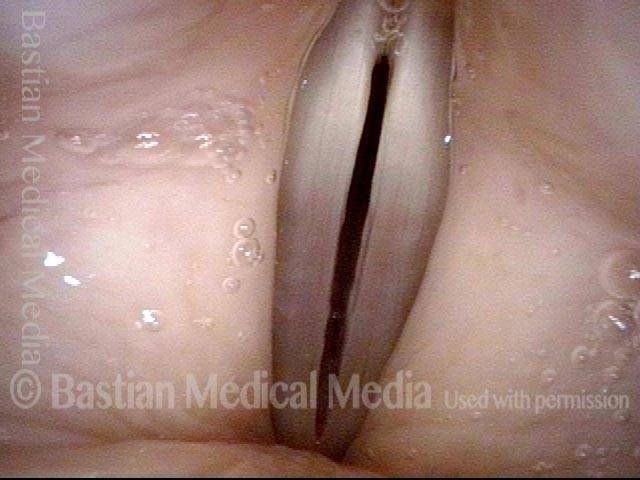
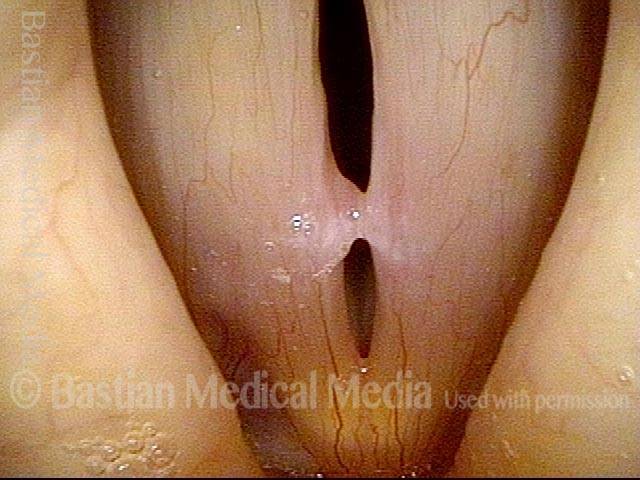
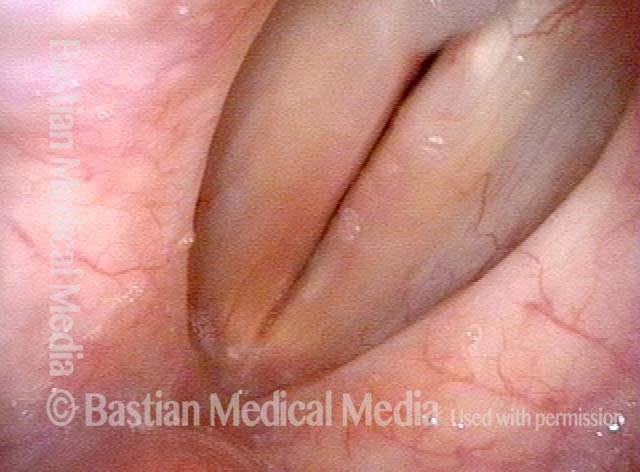
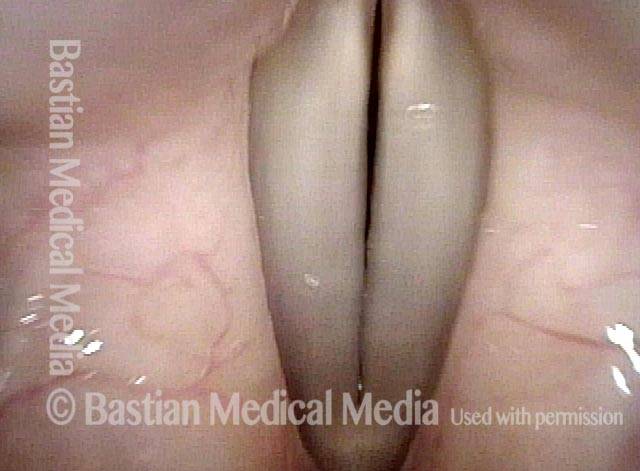
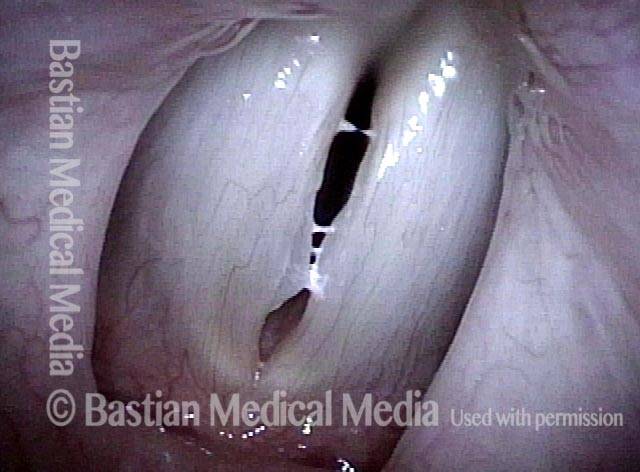
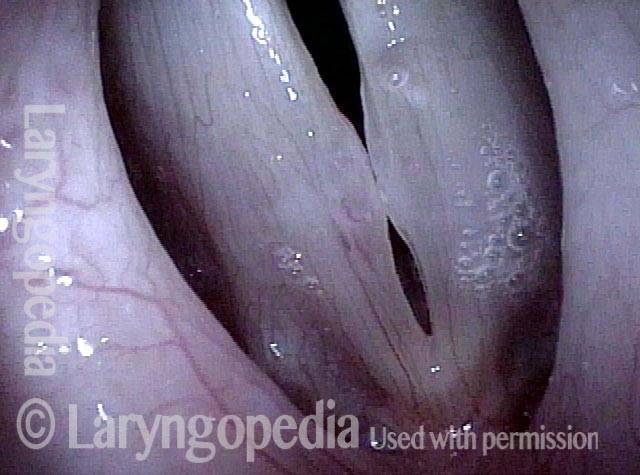
Vocal nodules (1 of 6)
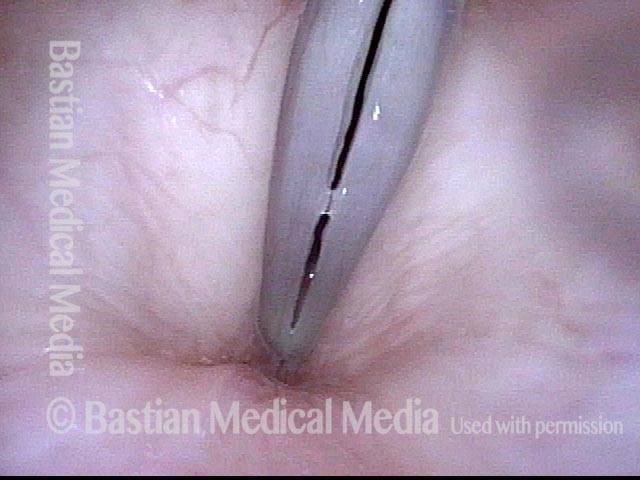
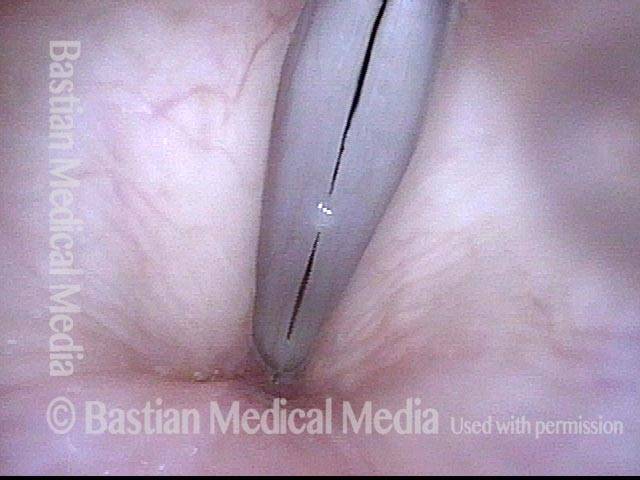
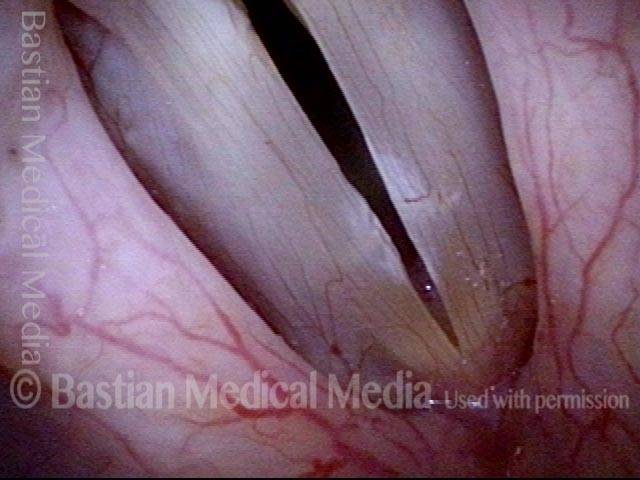
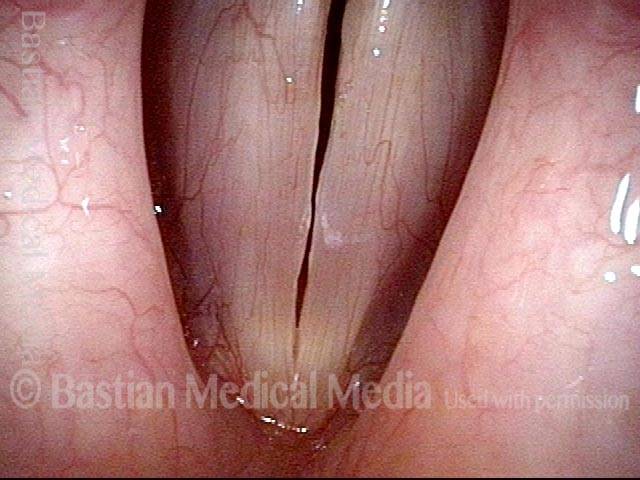
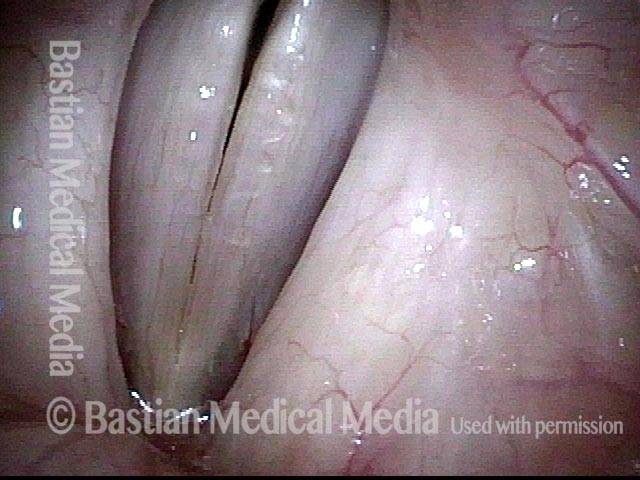
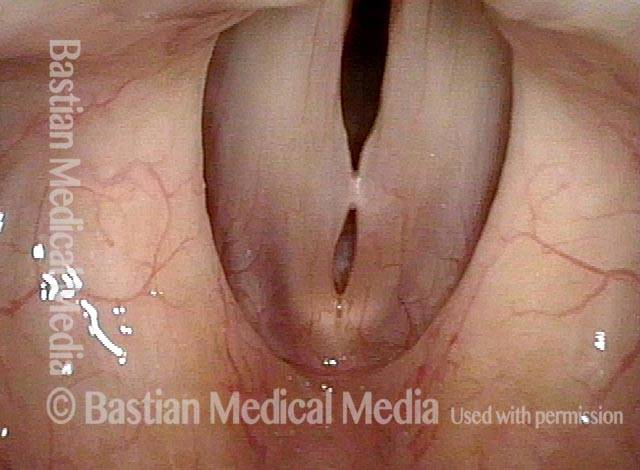
Strobe light, phonation, open phase of vibration, at the pitch D5 (~587 Hz). There are vocal nodules on both vocal cords, of very long duration, even after voice rest and speech therapy. Compare with photos 3 and 5.

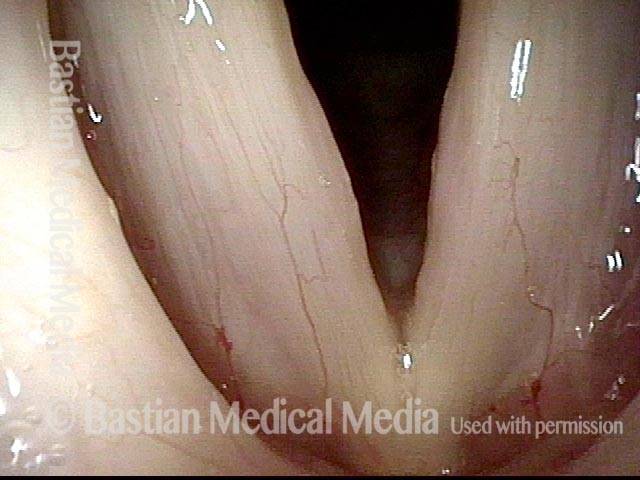
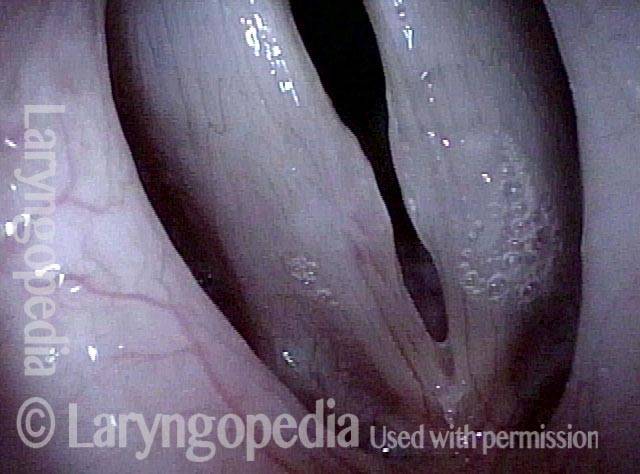
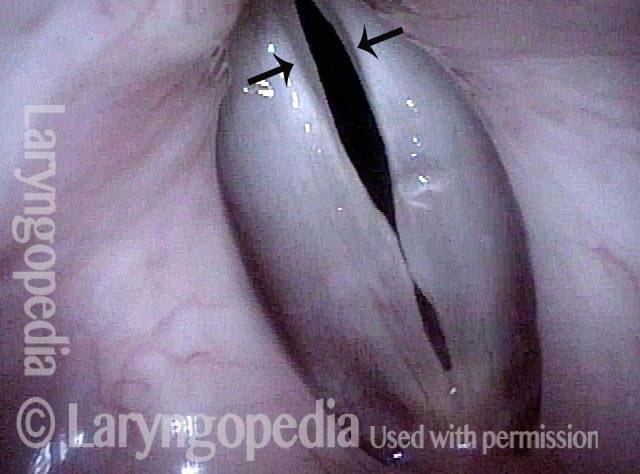
Breathy voice (2 of 6)
Same as photo 1, but during the closed phase of vibration. The nodules keep the vocal cords from coming together completely (as seen here), making the patient’s voice breathy. Compare with photos 4 and 6.

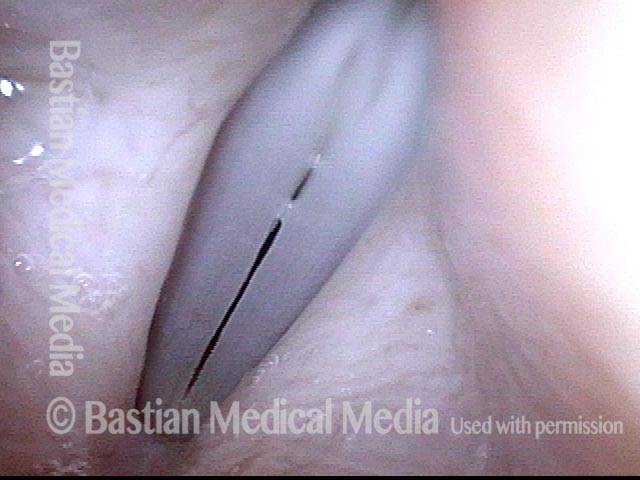
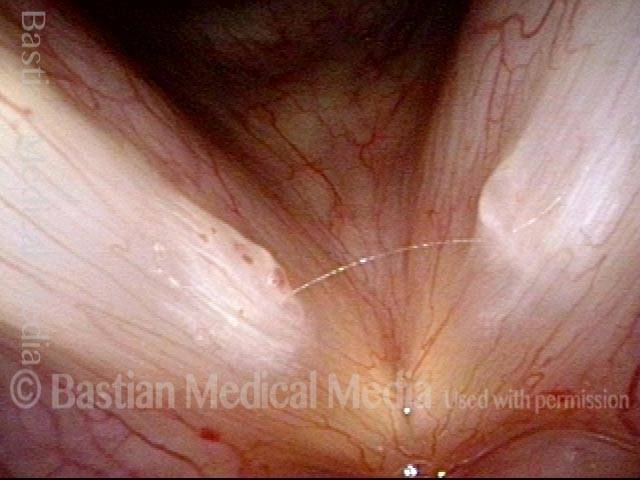
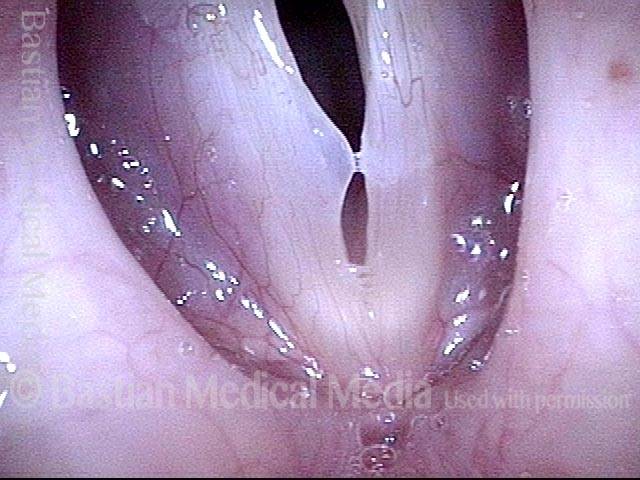
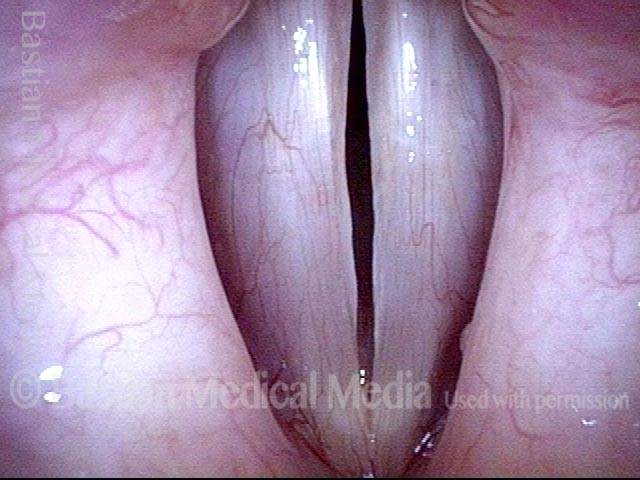
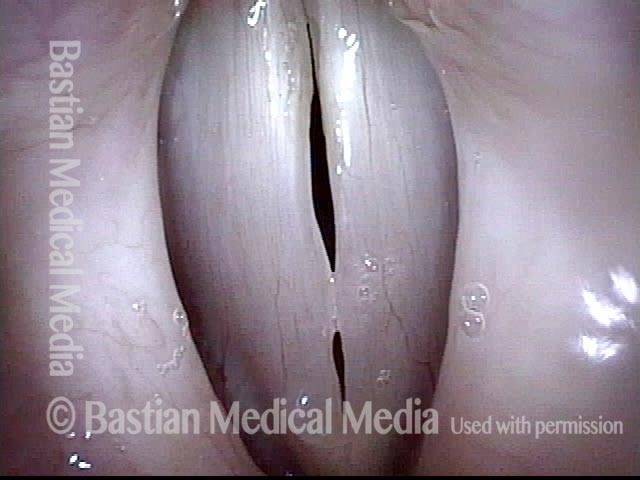
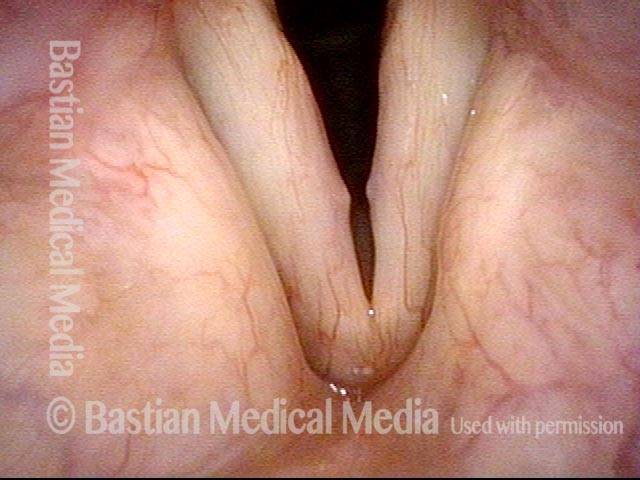
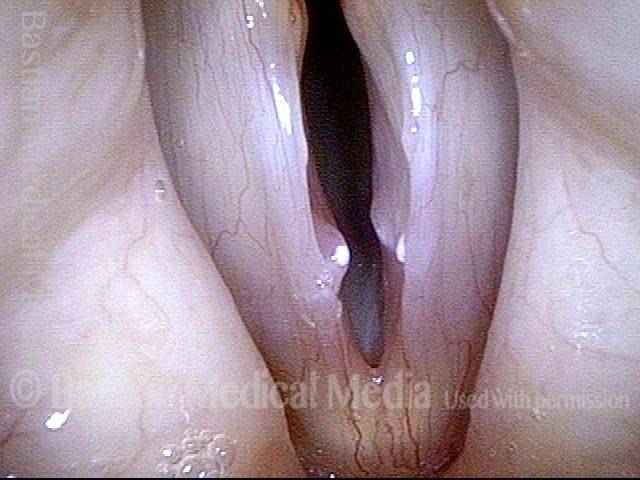
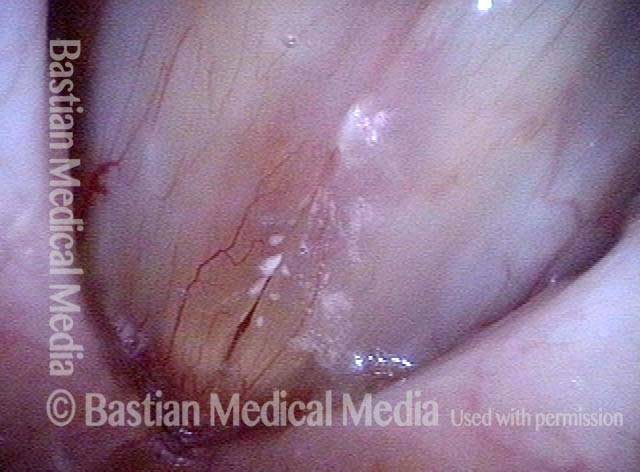
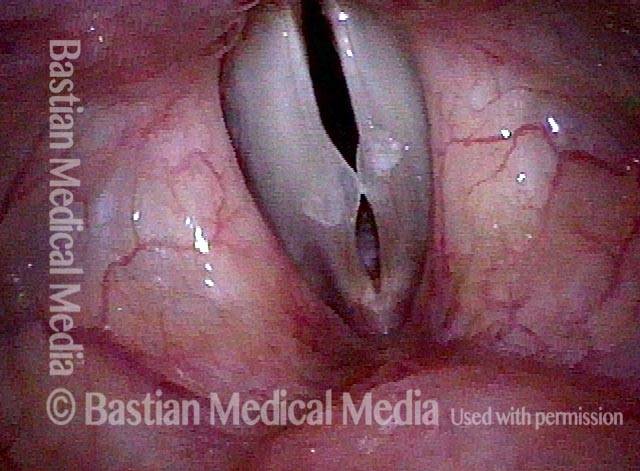
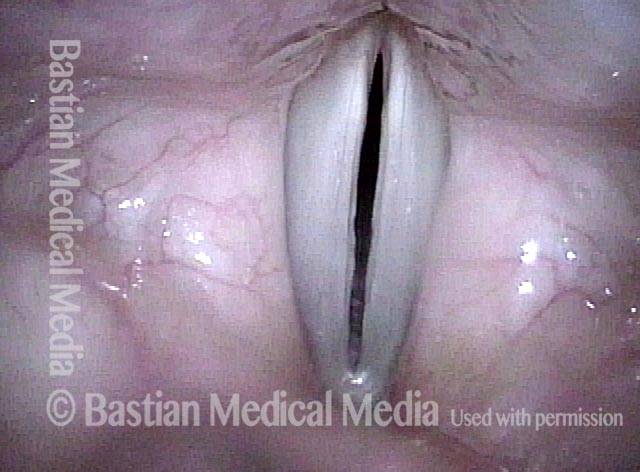
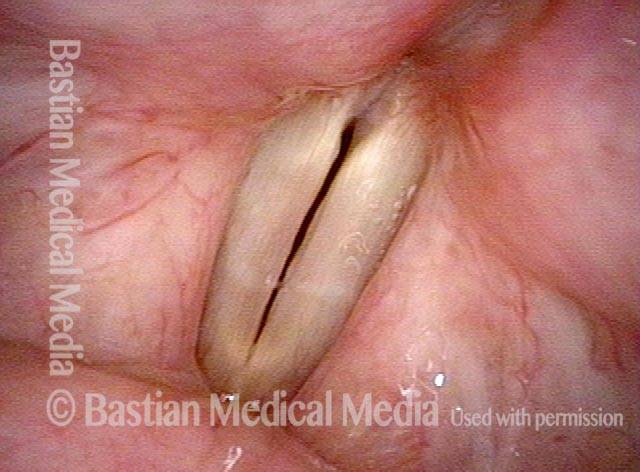
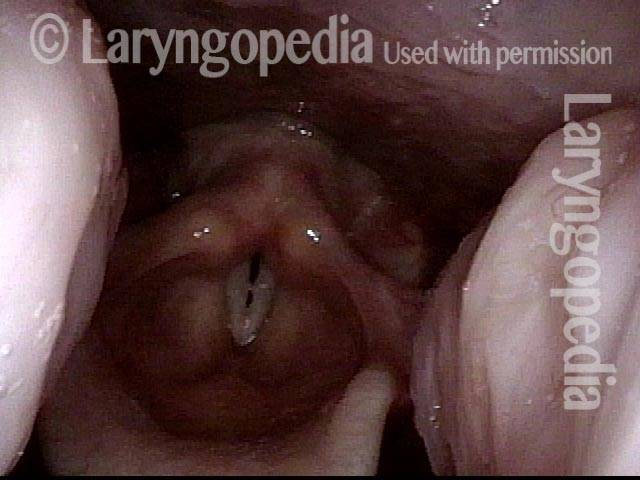
1 week after surgery (3 of 6)
One week after surgical removal of the vocal nodules. Strobe light, phonation, open phase of vibration, at the pitch B5 (~988 Hz). (The small “blob” seen at the midpoint of the cords is just incidental mucus.)
Closed phase (4 of 6)
Same as photo 3, but during the closed phase of vibration.
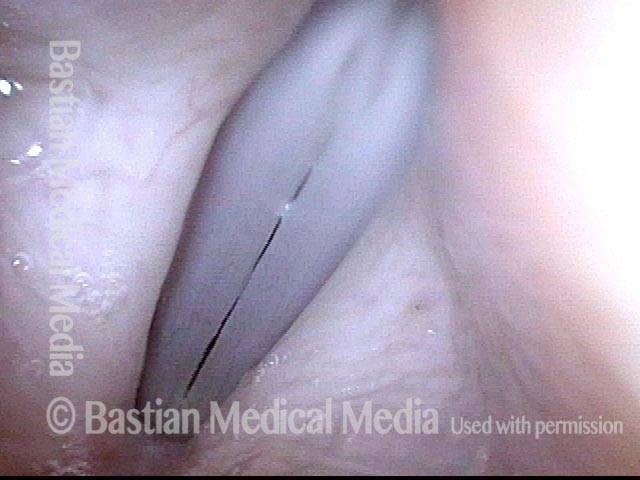
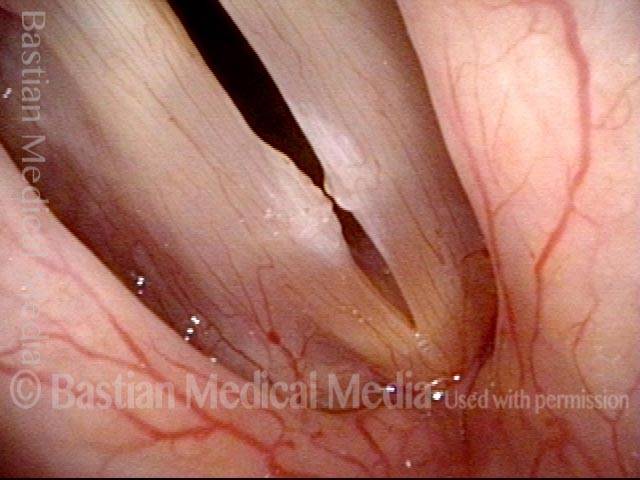
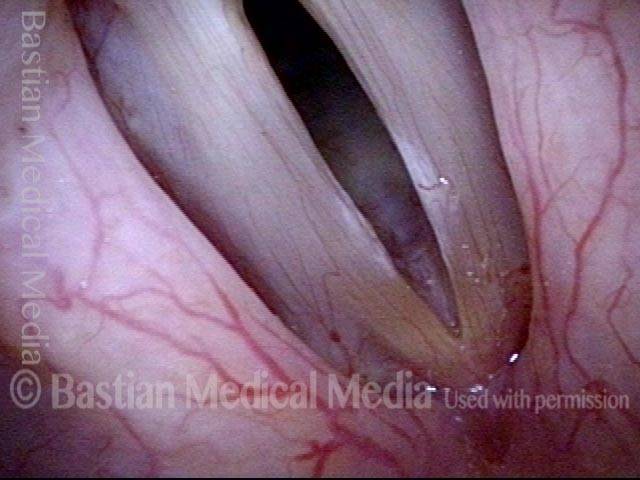
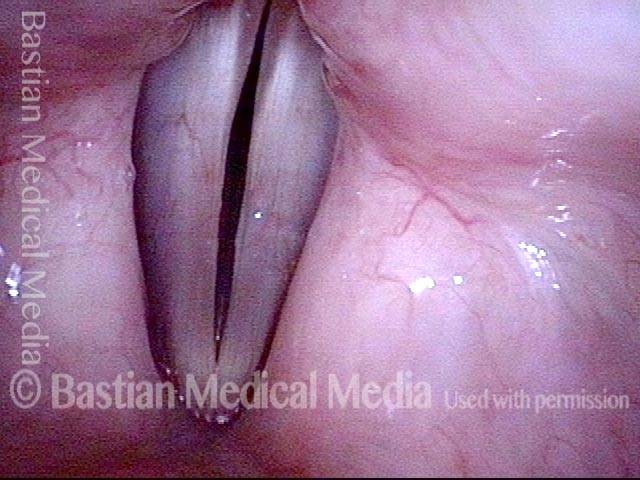
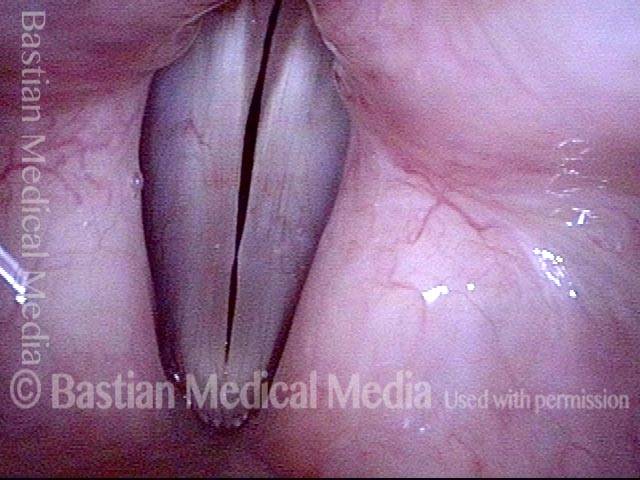
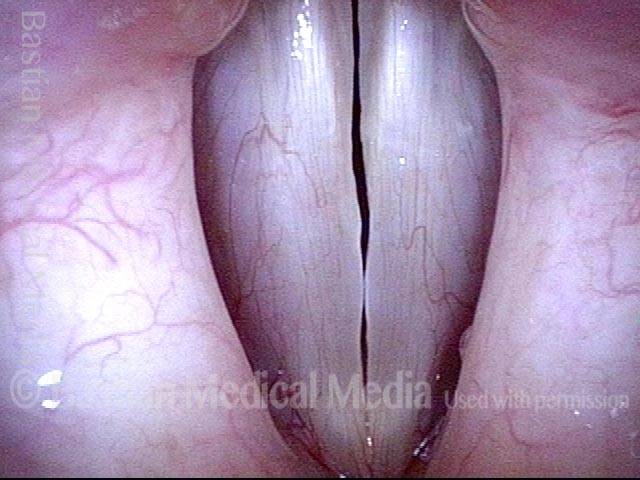
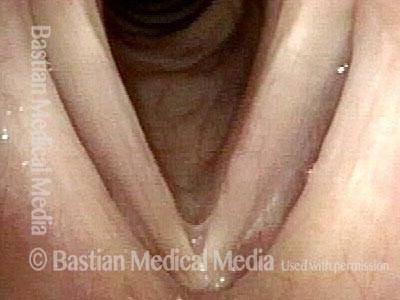
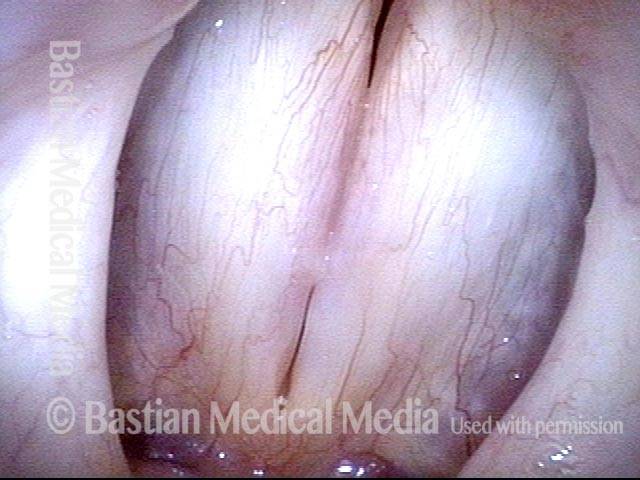
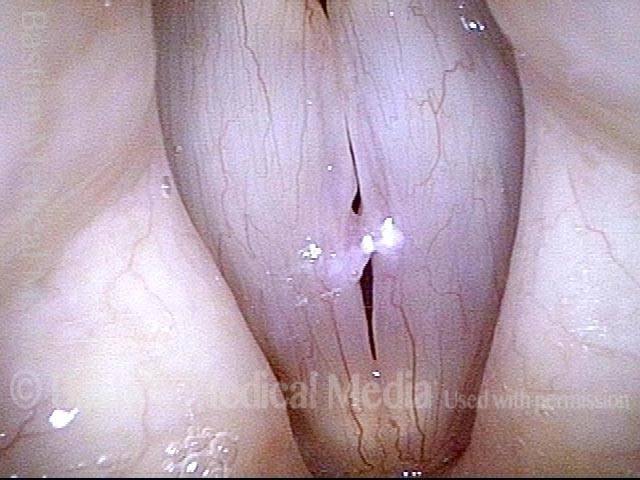
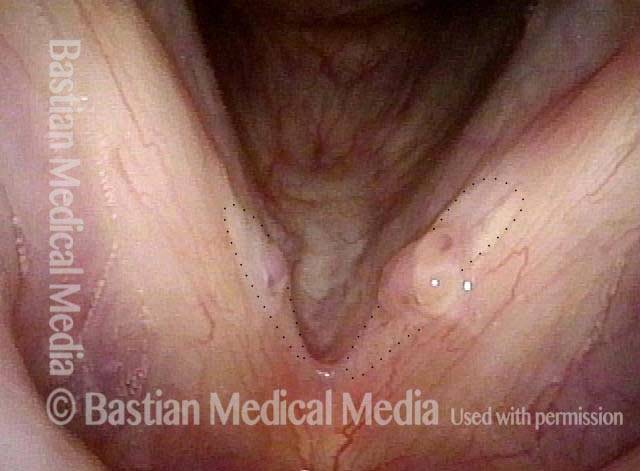
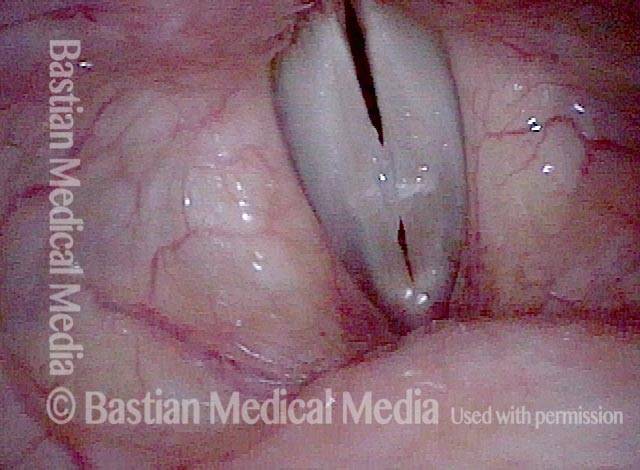
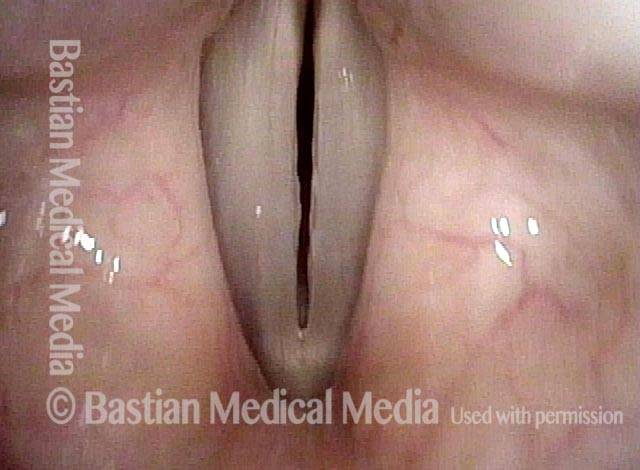
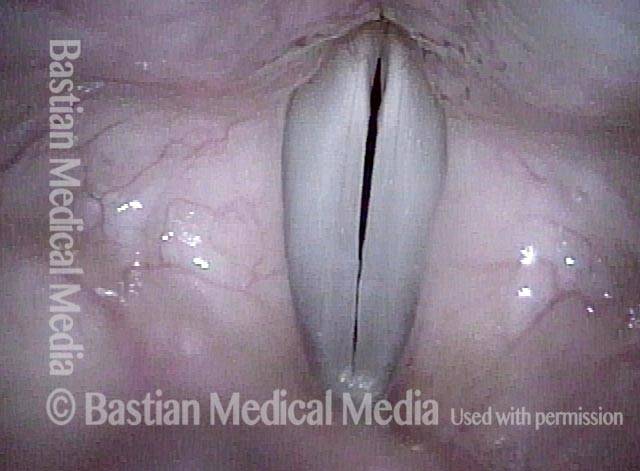
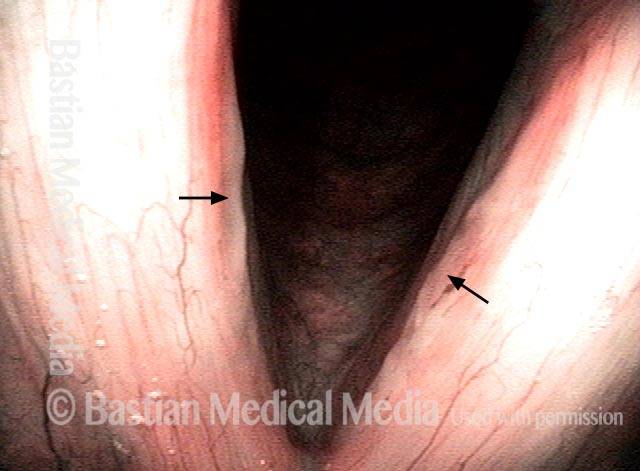
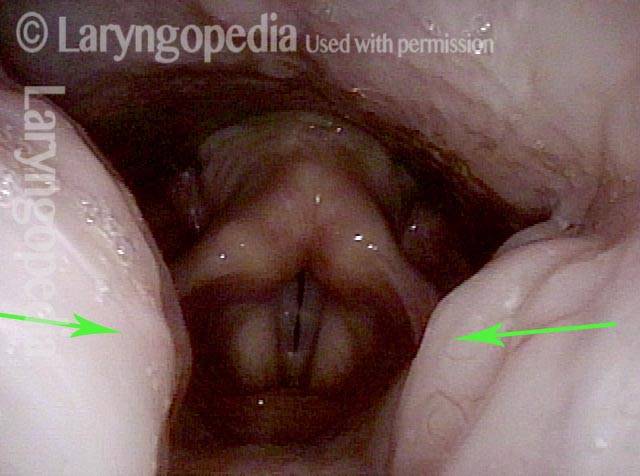
7 weeks after surgery (5 of 6)
Seven weeks after surgical removal of the nodules. Strobe light, phonation, open phase of vibration, at the pitch C#6 (~1109 Hz). (Incidental mucus is obscuring the posterior end of the vocal cords.)
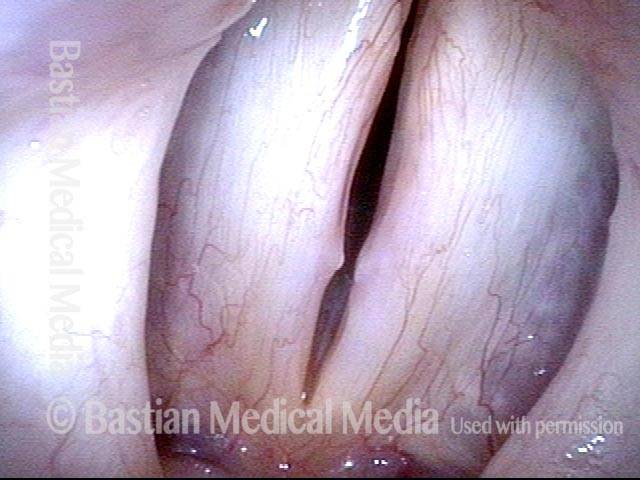
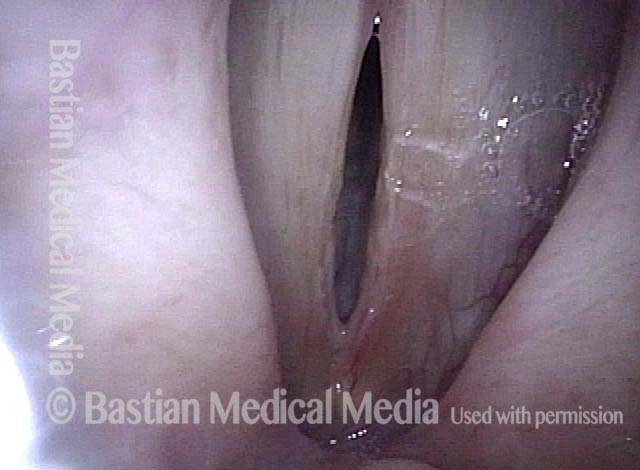
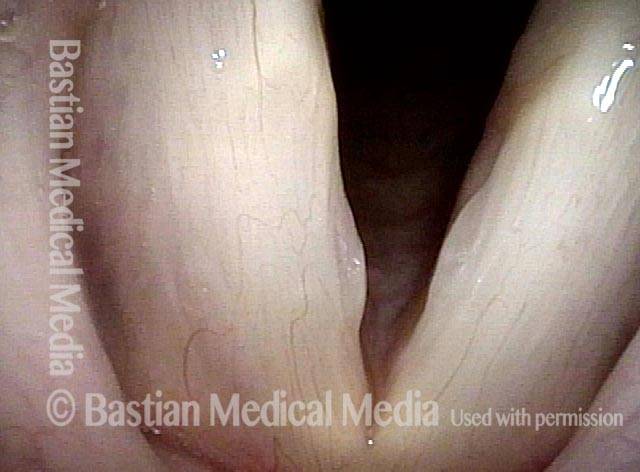
7 weeks after surgery (6 of 6)
Same as photo 5, but during the closed phase of vibration. Voice is no longer breathy, and the upper range has been restored.
Noduli corde vocali polipoidi
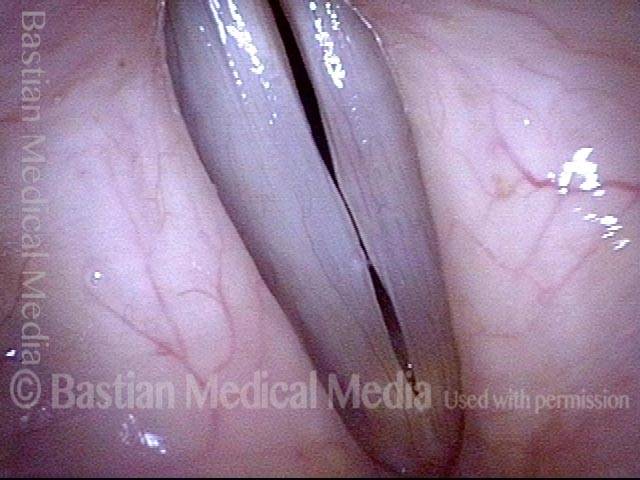
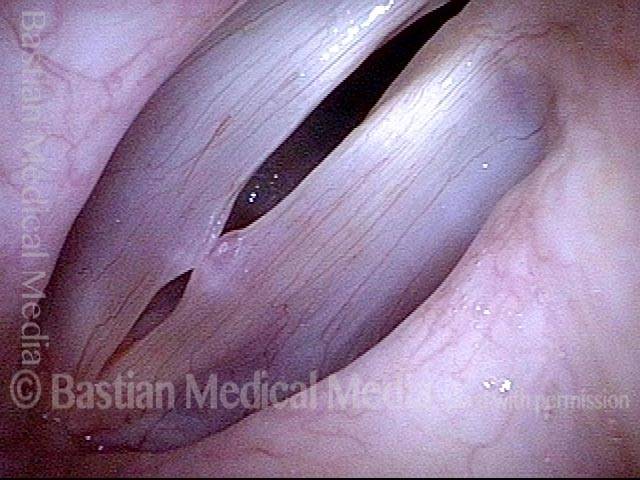
Polypoid vocal nodules (1 of 4)
Polypoid vocal nodules in a “vocal overdoer” with phenomenology typical for a mucosal injury. Narrow band illumination (blue-green light) makes vasculature more prominent. Note also the fusiform (long, low-profile) swelling, best seen on the left cord (right of image).

Incomplete closure (2 of 4)
Phonation, strobe light, at the beginning of the closed phase of vibration; one can see that closure will be incomplete due to early contact of the polypoid nodules.
Polypoid vocal nodules (3 of 4)
Phonation, strobe light, closed phase of vibration, with persistent gaps anterior and posterior to the polypoid nodules.
Polypoid vocal nodules (4 of 4)
Phonation, strobe light, open phase of vibration, continues to show the mid-cord swellings.

Noduli corde vocali, leucoplachia ed ectasia capillare
Vocal nodules, leukoplakia, and capillary ectasia (1 of 4)
Abducted breathing position, standard light. Notice not only the margin swellings (nodules) but also the ectatic capillaries and the roughened leukoplakia. This person illustrates well the idea that vibratory injury can be manifested differently. Many express the injury more in the form of sub-epithelial edema and other changes; this person also has considerable epithelial change.
Vocal nodules, leukoplakia, and capillary ectasia (2 of 4)
Prephonatory instant, standard light.
Vocal nodules, leukoplakia, and capillary ectasia: 6 months later (3 of 4)
Partial resolution of mucosal injury as a result of behavioral changes directed by a speech pathologist. Strobe light, open phase of vibration.
Vocal nodules, leukoplakia, and capillary ectasia: 6 months later (4 of 4)
Strobe light, moving towards closed phase of vibration.
Noduli corde vocali, prima e dopo l’intervento chirurgico
Vocal nodules (1 of 10)
Vocal nodules under standard light. Note asymmetry in size.

Prephonatory instant (2 of 10)
Prephonatory instant, standard light.

Translucency (3 of 10)
Closed phase of vibration, with notable translucency of the right vocal cord (left of image), which is often a predictor of chronicity and only partial response to speech (voice) therapy.

Open phase (4 of 10)
Open phase of vibration, strobe light.
1 week after surgery (5 of 10)
A week after vocal cord microsurgery, standard light.

1 week after surgery (6 of 10)
Open phase of vibration, strobe light.
1 week after surgery (7 of 10)
Closed phase of vibration, strobe light, showing tiny margin elevations, bilaterally.
Vocal nodules: 10 weeks after surgery (8 of 10)
Prephonatory instant shows recurrent swelling due to persistent vocal overuse, despite careful preoperative preparation for surgery by a voice-qualified speech pathologist. Patients must know “we are only operating on your vocal cords, not your personality, occupation, friend group, social life, etc.”
10 weeks after surgery (9 of 10)
Open phase of vibration, strobe light.
10 weeks after surgery (10 of 10)
Closed phase of vibration, strobe light. The “original equipment” capabilities of the voice early after successful vocal cord microsurgery (above) have been diminished, but capabilities remain markedly better than they were with the original lesions.
Esempio 2
Vocal nodules (1 of 4)
Vocal nodules, moderately large, seen with cords in abducted (breathing) position.

Phonation (2 of 4)
Phonation, showing early contact of the nodules, and large gaps anterior and posterior to the nodules.
After surgery (3 of 4)
Phonatory position, after surgical removal. Note the straightened vocal cord margins.
After surgery (4 of 4)
Breathing position, also post-surgery.

Esempio 3
Vocal nodules, before surgery (1 of 4)
Young sociable woman in sales, with chronic hoarseness due to broad-based “polypoid nodules.” Breathing position, standard light.
Before surgery (2 of 4)
Making voice at C5 (~523 Hz), showing large swelling on the right cord (left of photo), and lower-profile one on the opposite cord.
After surgery (3 of 4)
Seven days after vocal cord microsurgery; breathing position, standard light. Although there is mild residual post-surgical inflammation of the left cord margin (right of photo), the voice is already markedly improved and normal-sounding. Compare with photo 1.
Vocal nodules, after surgery (4 of 4)
Making voice at A5 (880 Hz). The vocal cords match accurately and both oscillate, despite mild broad-based inflammatory swelling of the left cord margin (right of photo). Compare with photo 2.
Noduli corde vocali, a forma di spicola
Vocal nodules (1 of 3)
Open phase of vibration just as vocal cords are also parting (to assume breathing position), strobe light. Note the small “spicule” nodules; these are at the other end of the continuum from “fusiform” or “broad-based” nodules.

During phonation (2 of 3)
Strobe light, high-pitched voice, showing early contact of the spicule-form nodules.

Closed phase (3 of 3)
Closed phase of vibration at lower pitch, strobe light.

Esempio 2
Vocal nodules (1 of 4)
Small, spicule-shaped nodules, in a soprano singer, as seen under standard light, in breathing position. This class of nodules is sometimes thought to have no potential to affect the voice (unlike broader-based, fusiform nodules).

Small nodules (2 of 4)
As the vocal cords approach each other to produce voice, note the pointed shape of these small nodules.
Phonation (3 of 4)
Phonation, under strobe light, closed phase of vibration, at the pitch C4 (~262 Hz). This patient’s voice is notably impaired.
Open phase (4 of 4)
Open phase of vibration, showing again the spicule-shaped nodules.
Noduli fibrotici
Fibrotic nodules (1 of 5)
This patient, a physical education instructor, has through vocal overuse developed the broad-based, rounded swellings seen here on each vocal cord. These swellings lack the watery or translucent appearance associated with edema swelling, because they are stiffer and more fibrotic.

Fibrotic nodules: full-length vibration at low pitch (2 of 5)
Phonation at low pitch, under strobe light, at moment of vocal cord contact (closed phase of vibration). At this pitch, the vocal cords are vibrating along their full length. (Ignore the small amount of whitish mucus.)
Fibrotic nodules: full-length vibration at low pitch (3 of 5)
Phonation at low pitch again, but now at the open phase of vibration.
Fibrotic nodules: segmental vibration at high pitch (4 of 5)
Phonation, very high pitch, closed phase of vibration. Now only the segment of the vocal cords indicated by the dotted lines is vibrating.

Fibrotic nodules: segmental vibration at high pitch (5 of 5)
Phonation, very high pitch, open phase of vibration. Again, there is only segmental vibration, indicated by the dotted lines.
Noduli corde vocali
Vocal nodules (1 of 4)
Vocal nodules, with cords in abducted (breathing) position. Note also a thin layer of mucus.
Prephonatory instant (2 of 4)
Vocal nodules at prephonatory instant under standard illumination.
Open phase of vibration (3 of 4)
Under strobe light, open phase of vibration.
Closed phase of vibration (4 of 4)
Under strobe light, closed phase of vibration.
Esempio 2
Vocal nodules (1 of 2)
Note that the nodules are not seen well during breathing (abducted position).

Vocal nodules (2 of 2)
In the same patient, these fusiform vocal nodules are easily seen at the prephonatory instant, and of course (not shown here) under strobe illumination.

Esempio 3
Vocal nodules (1 of 1)
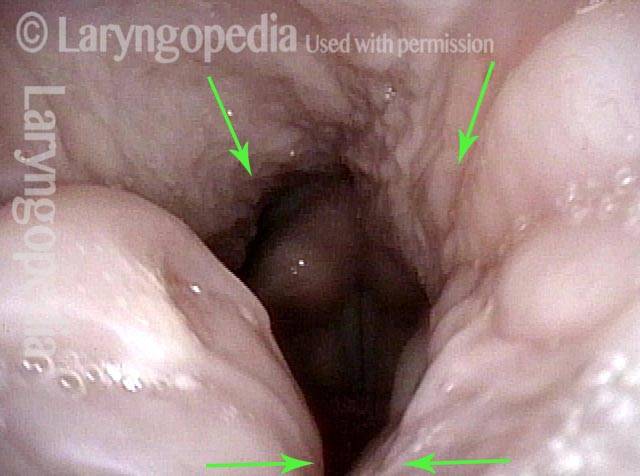
Note the asymmetry, with the nodule on the right cord (left of image) larger than left, and incomplete phonatory closure, causing breathy voice quality and loss of expected upper range.
Example 4
Vocal nodules (1 of 1)
Greatly increased glottal mucus, likely related to acid reflux, and subtle, hazy leukoplakia.
Ferite delle corde vocali, 2 ore dopo l’intervento chirurgico
Polypoid nodule, open phase (1 of 8)
Man in mid-30’s with chronic hoarseness due to boisterous personality, and work voice demands. Open phase vibration, low pitch shows large left cord (right of photo) polypoid nodule.

Polypoid nodule, closed phase (2 of 8)
Closed phase, at same low pitch, mostly conceals the injury.
Polypoid nodule, right and left cords (3 of 8)
Still at same low pitch, the early ‘closing’ phase shows the right sided (left of photo) polypoid nodule, and the larger left-sided lesion (right of photo).
Segmental vibration (4 of 8)
At high pitch, vibration is damped in mid and posterior cords, and only the anterior segment vibrates at arrows.
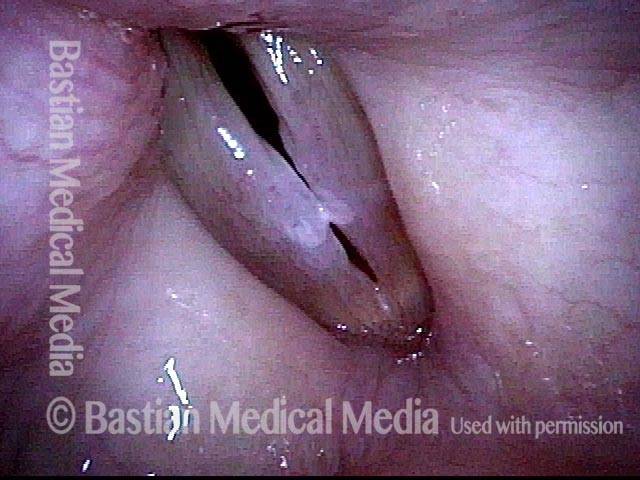
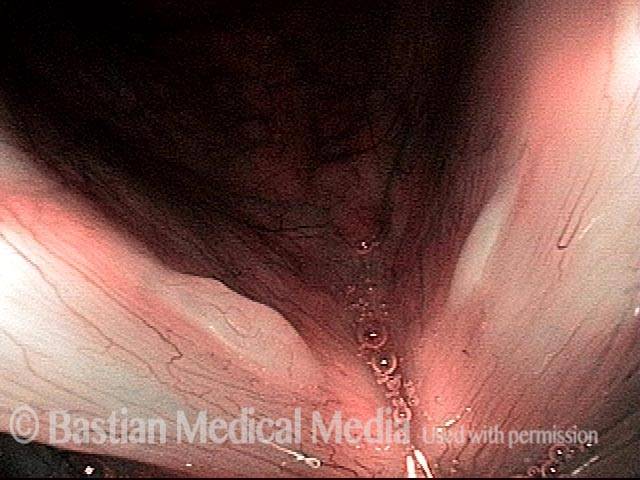
Post-surgery wounds (5 of 8)
Two hours after microsurgical removal of the lesions, the fresh, 3-mm “wounds” are seen at close range.

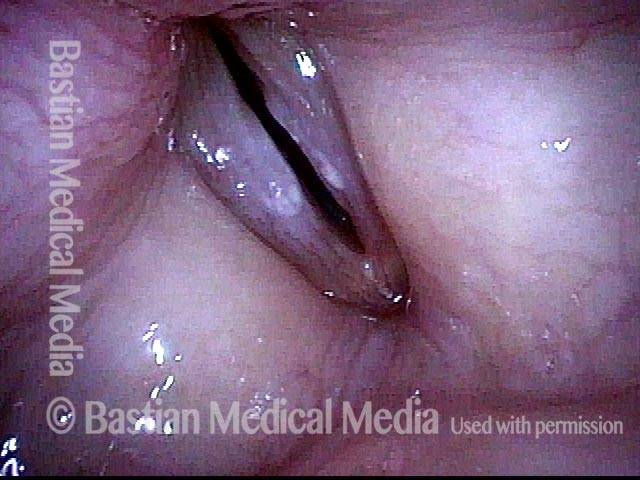
Post-surgery, closed phase (6 of 8)
View while making voice shows straight-line match of the vocal cord margins, and equal bilateral blurring, preliminarily suggesting preserved vibratory ability. Compare with photos 1-4.
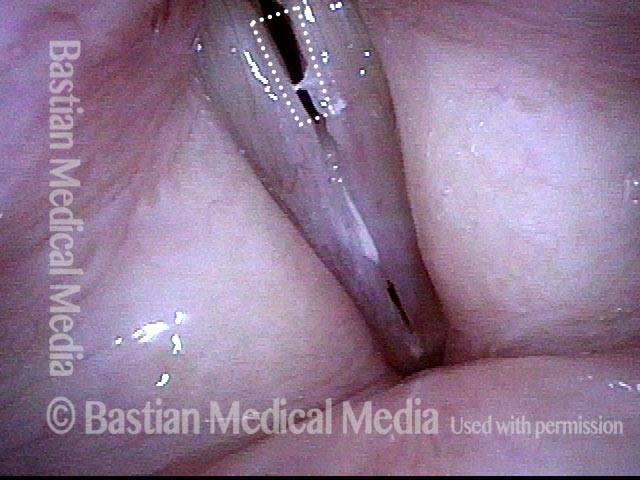
Post-surgery, open phase (7 of 8)
Open phase of vibration at E-flat 4 (311 Hz). The patient was unable to make this pitch just 2 hours earlier. Compare with photo 3.

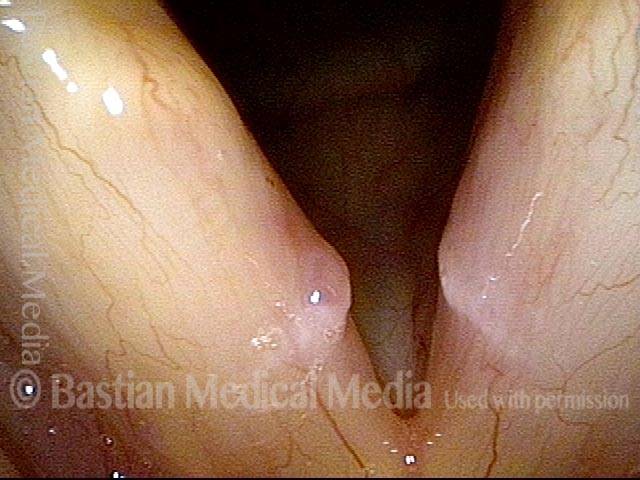
Post-surgery, precise match (8 of 8)
Closed phase vibration, also at E-flat 4, showing precise match, and verifying bilaterally equal mucosal oscillatory ability. Increased mucus is from the irritation of recent surgery.
Fibrosi come base per i noduli, prima e dopo l’intervento chirurgico
Bilateral polypoid nodules (1 of 8)
Fibrosis as a Base to Nodules, Before and After Surgery
Narrow-band lighting (2 of 8)
At greater magnification, and also under narrow-band light. The area of fibrosis is more clearly seen, now without the dotted lines.

Closed phase (3 of 8)
Closed phase of vibration at ~A4 (440 Hz), as seen under strobe light.

Open phase (4 of 8)
Open phase of vibration also at ~ A4.

Two weeks after surgery (5 of 8)
Less than two weeks after surgical removal of the polyps. The faint white zone of margin fibrosis is again seen. Compare with photo 1.

Phonation (6 of 8)
Phonation under standard light shows that vocal cord margins now match, and both margins blur; suggesting vibratory flexibility.

Margin fibrosis (7 of 8)
Closed phase of vibration, at ~ A4 (440 Hz), as seen under strobe light. Margin fibrosis seen best here, indicated by the black dotted line. Compare with photo 3.

Open phase (8 of 8)
Open phase of vibration. The same pitch (A4) reveals excellent vibratory flexibility and equal amplitude (lateral excursion) of vibration. Compare with photo 4.
Noduli vocali prima e 1 settimana dopo la rimozione
Vocal nodules (1 of 8)
Semi-professional high soprano with grossly impaired upper voice due to polypoid (fusiform) vocal nodule.

Muscular tension dysphonia (2 of 8)
Phonatory view shows a degree of muscular tension dysphonia (separated vocal processes), too.
Open phase (3 of 8)
Nearly open phase under strobe light at B4 (494 Hz).
Closed phase (4 of 8)
Closed phase of vibration, aslo at B4.
Post-op, one week (5 of 8)
A week after surgical removal of the nodules, at the prephonatory instant, D5, showing margin irregularity.
Phonation (6 of 8)
Phonation, with vibratory blur under standard light.
Open phase (7 of 8)
Open phase of vibration (strobe light), at D5 (587 Hz). Irregular margins will iron out across time.
Closed phase (8 of 8)
At closed phase of vibration, also at D5. Note excellent match, bilaterally equal vibratory excursions, and partial correction of the MTD posterior commissure gap.
Nodulo vocale Irregolarità postoperatoria ma corrispondenza e flessibilità
Large vocal nodules (1 of 8)
Bilateral large vocal nodules in band singer that does close harmony musical styles.
Narrow band light (2 of 8)
Now under narrow band light to accentuate the vascular pattern.

At B2 (3 of 8)
At low pitch (B2 or 123 Hz).
At A5 (4 of 8)
At A5 (880 Hz).

One week after surgery (5 of 8)
A week after surgery, the “wounds” measure about 3mm long (at arrows).
Prephonatory instant (6 of 8)
Prephonatory instant, standard light, at C#5 (554 Hz).
Closed phase (8 of 8)
Closed phase, also at E5.

Open phase (7 of 8)
Open phase of vibration at E5 (659 Hz). Voice is markedly improved.

Cerca non solo noduli, ma anche vibrazioni segmentali e osserva la commissura posteriore per MTD
Open phase (1 of 4)
In a young pop-style singer, the open phase of vibration under strobe light at C#5 (554 Hz). This magnified view is best to see the large fusiform nodules.
Closed phase (2 of 4)
Closed phase of vibration at the same pitch shows touch closure—that is, that the nodules barely come into contact.
Segmental vibration (3 of 4)
Even when patients are grossly impaired in the upper voice as is the case here, the clinician always requests an attempt to produce voice above G5 (784 Hz), in order to detect segmental vibration. Here, the pitch suddenly breaks to a tiny, crystal-clear D6 (1175 Hz) Only the anterior segment (arrows) vibrates.

Posterior commissure (4 of 4)
A more panoramic view that intentionally includes the posterior commissure to show that the vocal processes, covered by the more ‘grey’ mucosa (arrows), do not come into contact. This failure to close posteriorly is a primary visual finding of muscular tension dysphonia posturing abnormality.
Tonsille “da bacio”.
Tonsils enlarged (1 of 3)
A singer with very large tonsils seen on either side of the photo as she sings A3 (220 Hz). The line of sight is looking straight down from the nasopharynx.
Higher pitch (2 of 3)
At an octave above, A4 (440 Hz), a slight pharynx contraction brings the tonsils closer together.
Tonsils in contact (3 of 3)
At nearly an octave higher again, G5 (784 Hz), the pharynx has contracted more (upper arrows), causing the tonsils to come into contact just out of the view (lower arrows)–hence the term “ kissing tonsils.” This phenomenon can often be seen by looking at the tonsils through the mouth on an “ah” vowel.
Chiedere sia alla Voce (attraverso la fenomenologia vocale) che alla Laringe (attraverso un esame motivato) di rivelare i propri segreti
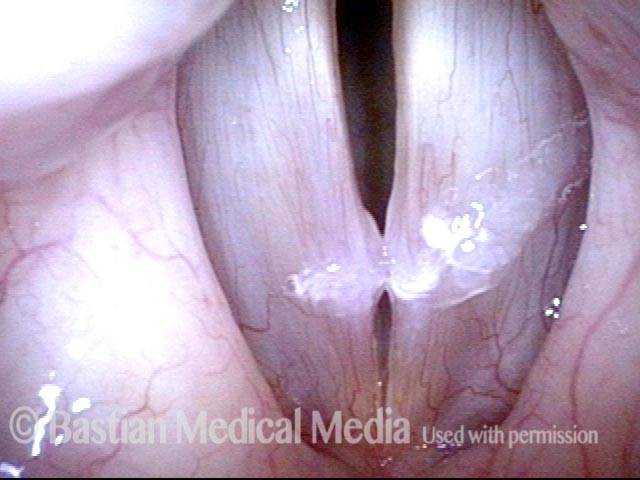
Obvious mucosal injury (1 of 3)
This young woman is hoarse, but two examinations elsewhere returned no significant findings. Her upper voice limitations during vocal capability testing already tell us “for certain” that there is mucosal injury, even before we look at the larynx. In this mid-range view, we can see early contact at the mid-cords, but the full extent and nature of the injuries are seen in the closer views that follow.

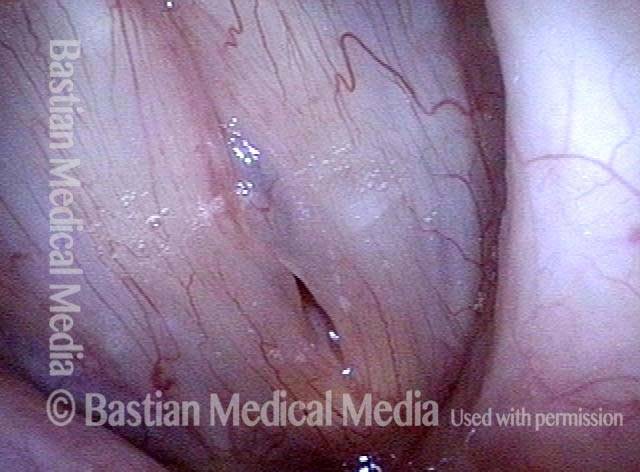
Vocal nodules (2 of 3)
At a more appropriate level of magnification, the vocal nodules are seen. But we want to know more…

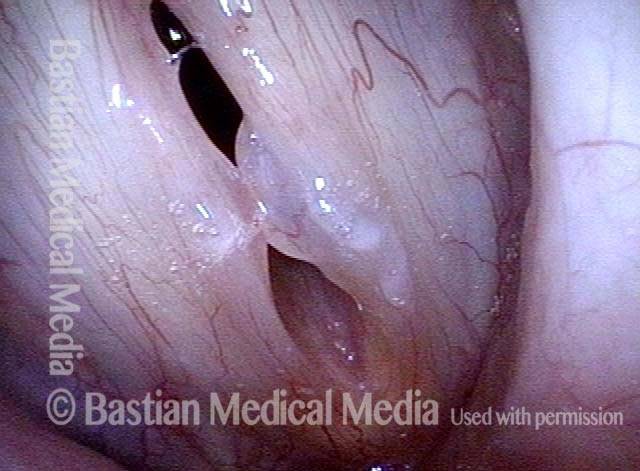
Capillary ectasia (3 of 3)
Slightly greater magnification and narrow band light point out more clearly the capillary ectasia. Now we know that for complete restoration of voice and of mucosal endurance, surgery will likely be needed, assuming this fits with the patient’s goals.

La mucosa chiazzata delle corde vocali può nascondere i solchi glottici
Vocal cord swelling and mucosa (1 of 4)
This young “dramatic” soprano is also a bona fide vocal overdoer. Her vocal capabilities have been diminishing for over two years. In this medium-range view, note the rounded swelling of the right cord (left of photo), but more significantly as we shall see, the increased vascularity and mottled appearance of the mucosa.

Same view under strobe light (2 of 4)
Under strobe light, at open phase of vibration at C#5 (523 Hz), we see a projecting, polypoid swelling of the right vocal cord, but not yet the more difficult problem.

Closed phase (3 of 4)
Closed phase of vibration, at the same pitch of C#5 shows the mismatch of the vocal cord margins. Is this the entire explanation for this patient’s hoarseness? Read on.

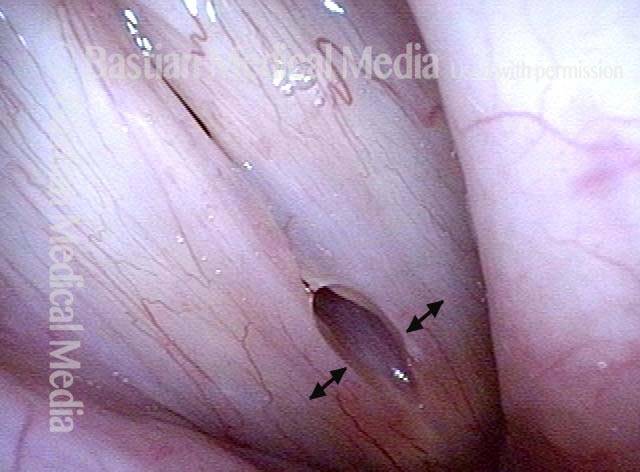
Glottic sulcus is visible (4 of 4)
At close range and high magnification, the open mouth of a right-sided glottis sulcus is seen. This side can be operated safely due to the excess, thick mucosa and would be expected to improve the margin match. On the left (right of photo), a sulcus is also seen, but the thinner mucosa makes successful surgery on the left more challenging.

{kind=link}