Torus mandibularis is a benign bony growth on the medial surface (tongue side) of the mandible or jaw bone. Also known as mandibular torus. Mandibular tori are usually seen on both the left and right sides (bilaterally). They often require no treatment unless they interfere with denture fitting.
In laryngology, mandibular tori come to attention because, when large, they can make it difficult or impossible for the clinician to gain a view of the vocal folds during microlaryngoscopy. That difficulty arises because during a microlaryngoscopy, the floor of the mouth is normally compressed by the laryngoscope to allow the scope to angle anteriorly at the viewing end, but mandibular tori, being composed of bone, do not compress.
Torus mandibularis (1 of 2)
View inside the mouth, focused on the floor of the mouth, with tongue retracted. The “mounds” seen in the foreground are unusually large tori, which are touching anteriorly.
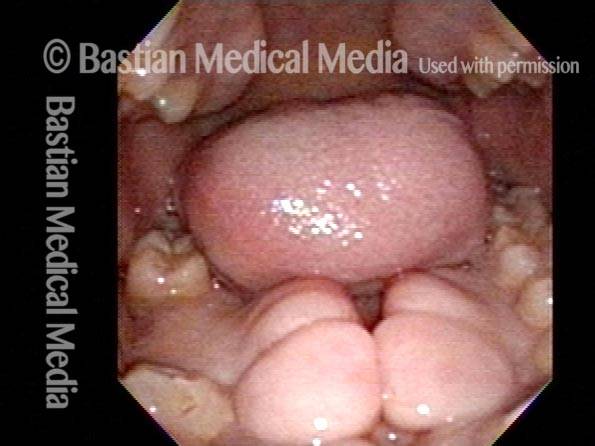
Torus mandibularis (2 of 2)
Looking more directly downward onto the tori, with the tongue now pointing upward at the roof of the mouth.
