Amyloidosis of the Larynx as Seen Over Time, with Treatment
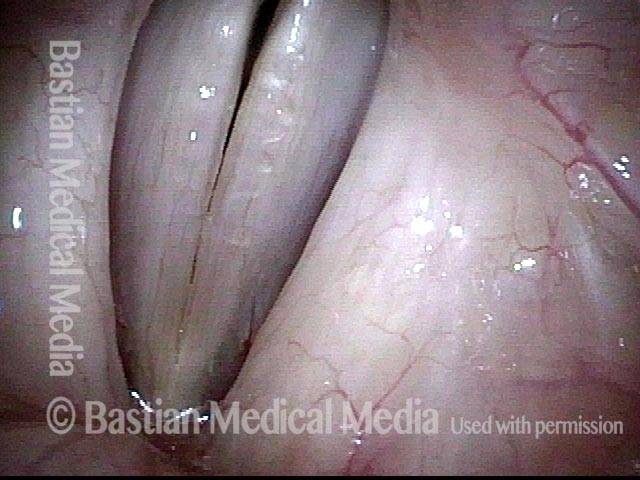
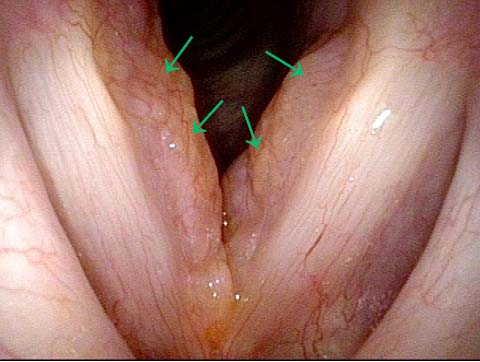
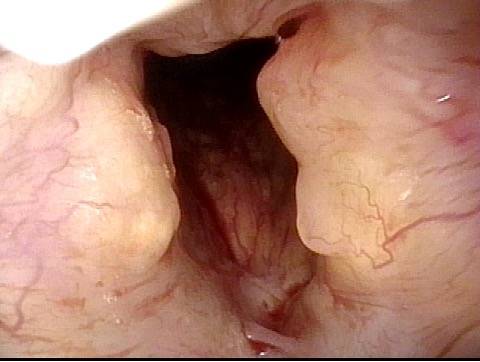
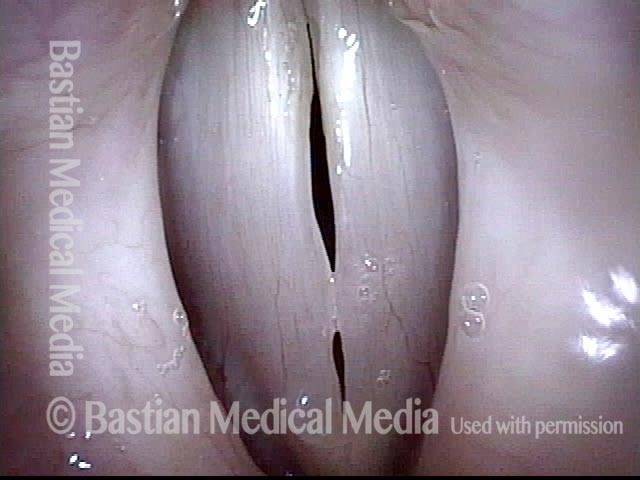
Primary laryngeal amyloidosis (1 of 7)
An example of primary laryngeal amyloidosis of the larynx. In this case, the yellowish, “candle-wax” proteinaceous material is being deposited just below the margin of the vocal cords (arrows)
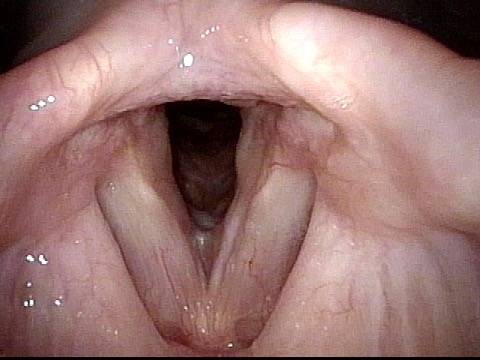
Bulky swelling (2 of 7)
When this person produces voice, the bulky swelling just below the margin of the vocal cords creates turbulence, incomplete match, and a rough voice quality. After laser debulking, the patient had a much improved voice for many years.
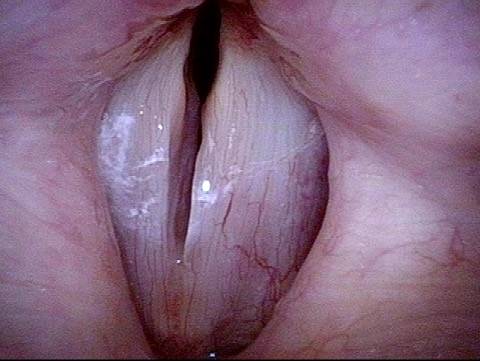
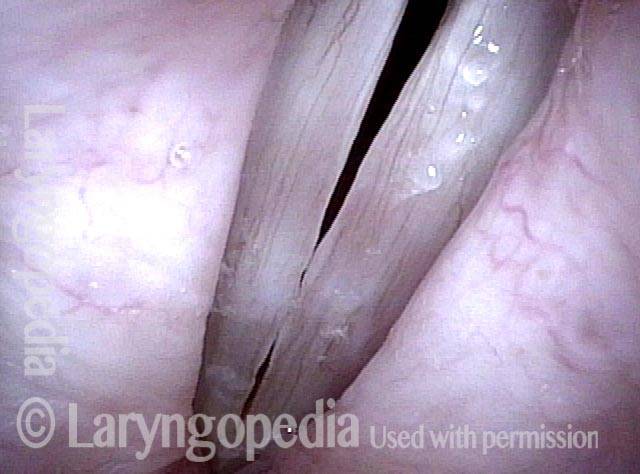
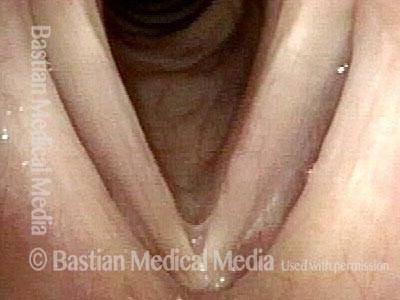
Amyloidosis (3 of 7)
Eight years later, the patient reappeared. She said voice had been good for many years but had been getting increasingly hoarse for the prior couple of years. Here you see major re-deposition of amyloid material.
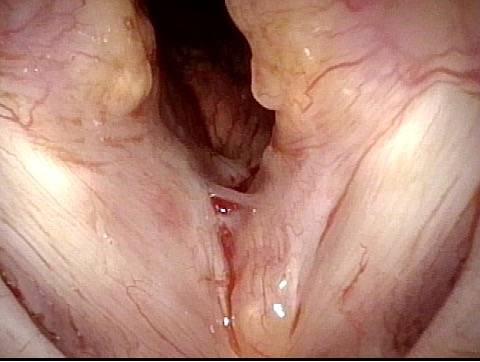
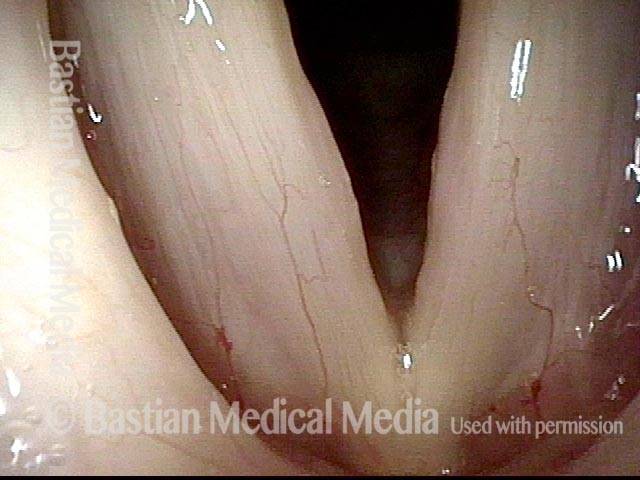
Amyloid deposits (4 of 7)
At very close range, the yellowish color typical of amyloid deposits is better seen.
Vocal cords cannot close completely (5 of 7)
During voice production under strobe light, the amyloid deposit under the left vocal cord prevents closure.

Amyloids Remain (6 of 7)
A year after laser debulking, the patient continued to have a very good voice, and only reappeared due to an unrelated question. As expected, smally amyloid deposits remain.
Voice remains clear (7 of 7)
When she produces voice, match and vibratory ability are very good, explaining her normal voice. It remans to be seen if amyloid will gradually reaccumulate over the next many years and need another debulking.

Surgery for Fibrosis, Polyp
Fibrosis + polyp (1 of 4)
An intense and dynamic teacher (not a singer) has developed not only polyp/ elevation, but fibrosis–the white submucosal deposition of scar-like tissue deposits. Narrow band illumination makes the nature of these lesions more “emphatic.”

Strobe light (2 of 4)
Under strobe light during voicing. Poor match and stiffness are best seen.

Post microsurgery, open phase (3 of 4)
A week after vocal cord microsurgery, voice is markedly improved. No attempt was made to remove all of the fibrosis, but only to straighten the vocal cord margins. Open phase of vibration at F5.

Post microsurgery, open phase (4 of 4)
Closed phase of vibration at same pitch shows that some margin swelling remains. The patient also has MTD; posterior cords are widely separated.
Vocal Nodules, Before and After Surgery
Vocal nodules, before surgery (1 of 4)
Young sociable woman in sales, with chronic hoarseness due to broad-based “polypoid nodules.” Breathing position, standard light.
Before surgery (2 of 4)
Making voice at C5 (~523 Hz), showing large swelling on the right cord (left of photo), and lower-profile one on the opposite cord.
After surgery (3 of 4)
Seven days after vocal cord microsurgery; breathing position, standard light. Although there is mild residual post-surgical inflammation of the left cord margin (right of photo), the voice is already markedly improved and normal-sounding. Compare with photo 1.
Vocal nodules, after surgery (4 of 4)
Making voice at A5 (880 Hz). The vocal cords match accurately and both oscillate, despite mild broad-based inflammatory swelling of the left cord margin (right of photo). Compare with photo 2.