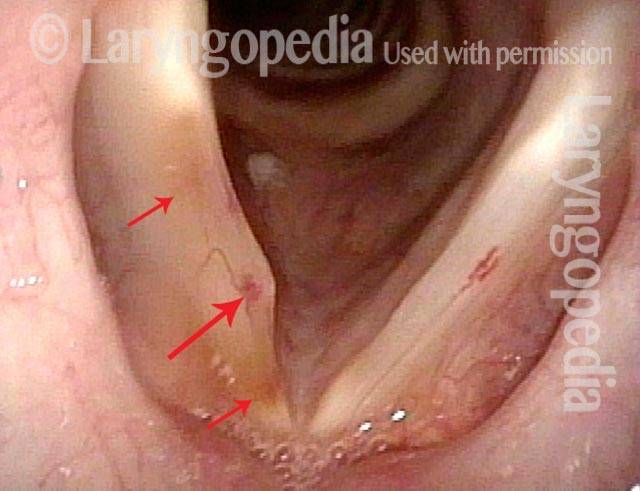
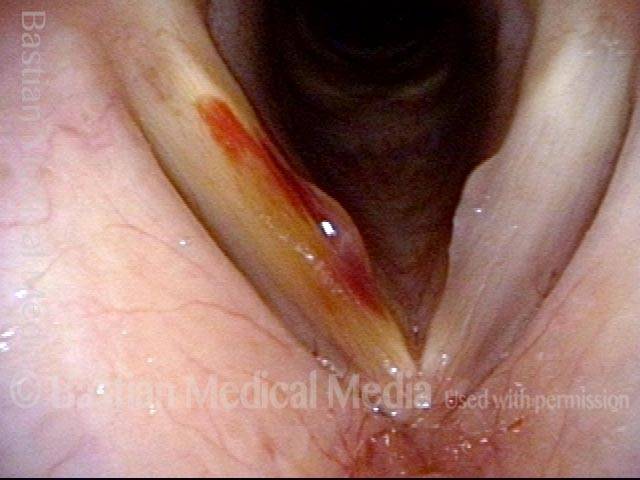
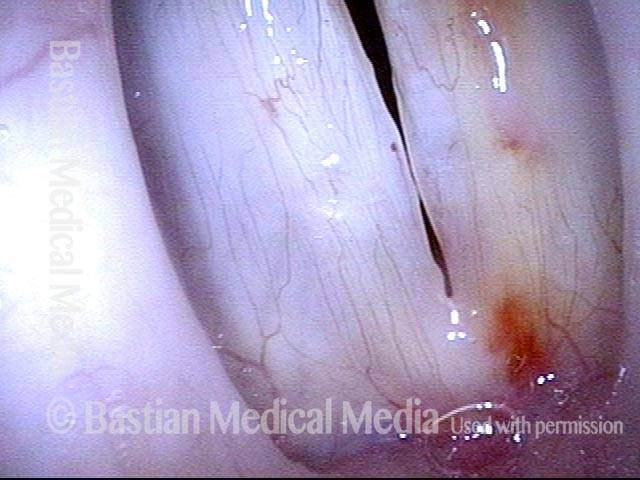
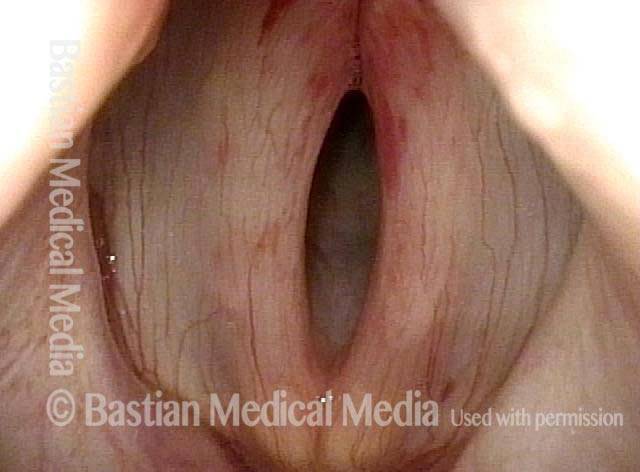
The rupture of one or more capillaries in the vocal cords, so that blood leaks into the tissue. This vocal cord bruising occurs as a result of excessively vigorous mucosal oscillation, usually during extensive or vigorous voice use, aggressive coughing, or even a very loud sneeze, and it can make the voice hoarse or otherwise limited.
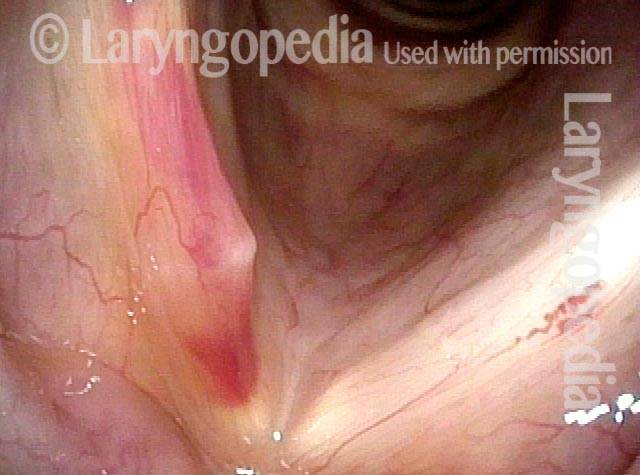
If the ruptured capillary is extremely superficial, like the capillaries seen on the white of the eye, then a “thin suffusion” kind of bruise occurs, and there is no deformity of the vocal cord margin; within a few days, the voice recovers. If the vessel is a few cell layers deeper into the cord, then a small “puddle” of blood like a micro-hematoma may collect and create a kind of “blood blister.” Although a superficial bruise resolves quickly and doesn’t seem to cause permanent damage, the “blood blister” type can become a hemorrhagic polyp and require surgery; with state-of-the-art surgery, however, the voice can virtually always be restored to its original capabilities.
Vocal Cord Bruise / Hemorrhage, Before and After Rest and Surgery
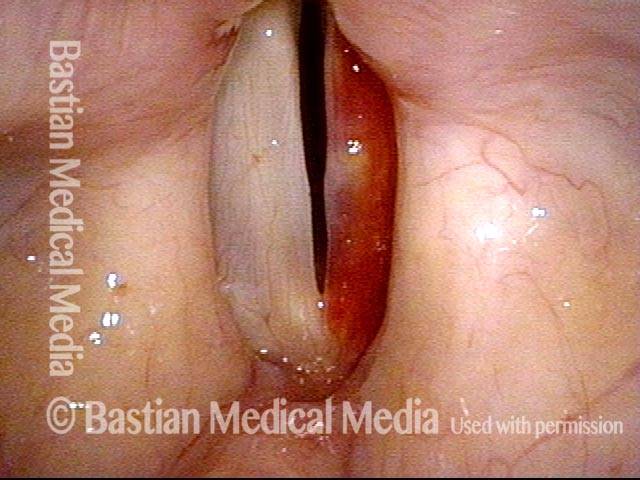
Vocal cord bruise / hemorrhage (1 of 4)
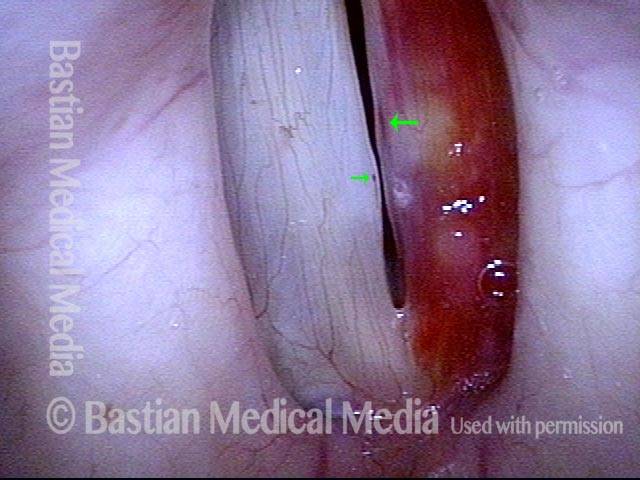
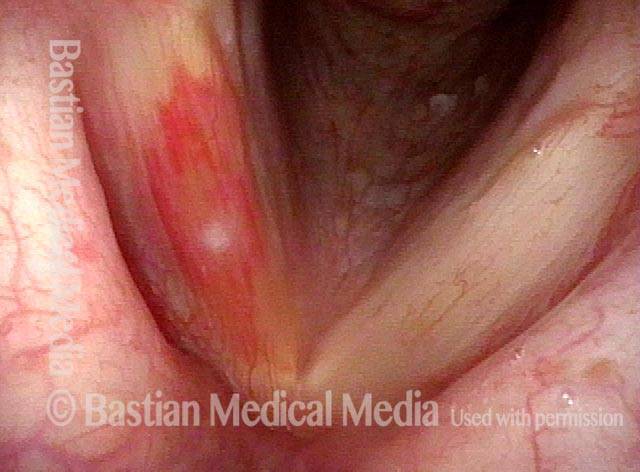
Vocal cord bruise / hemorrhage (2 of 4)

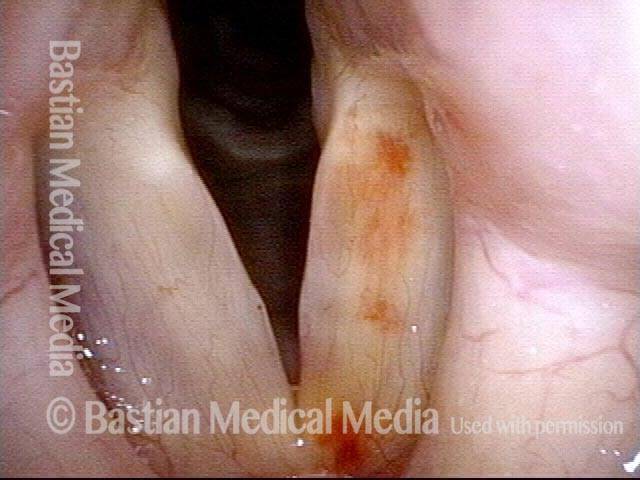
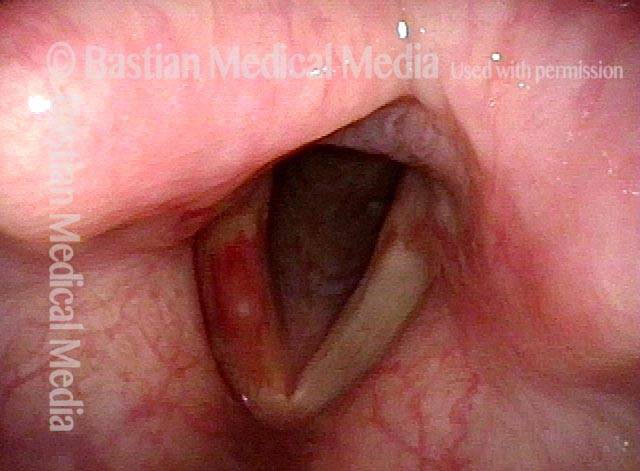
Vocal cord bruise / hemorrhage, after rest and surgery (3 of 4)
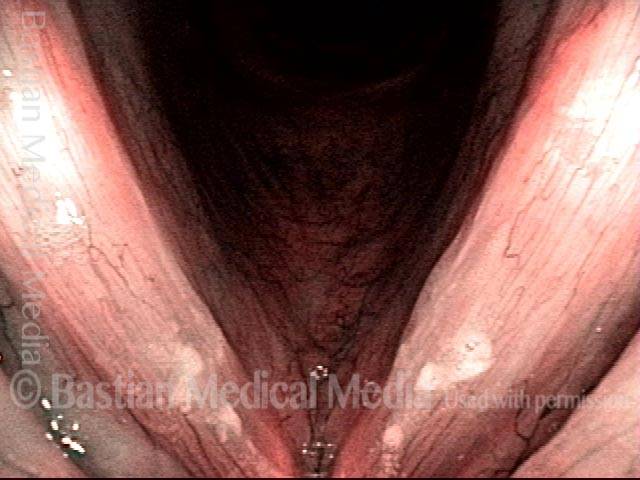
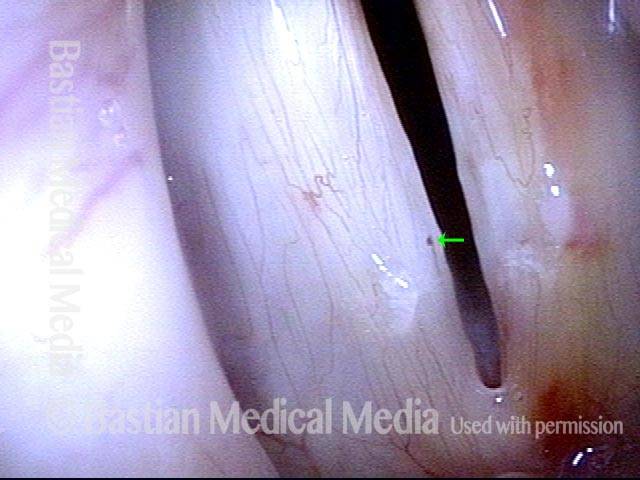
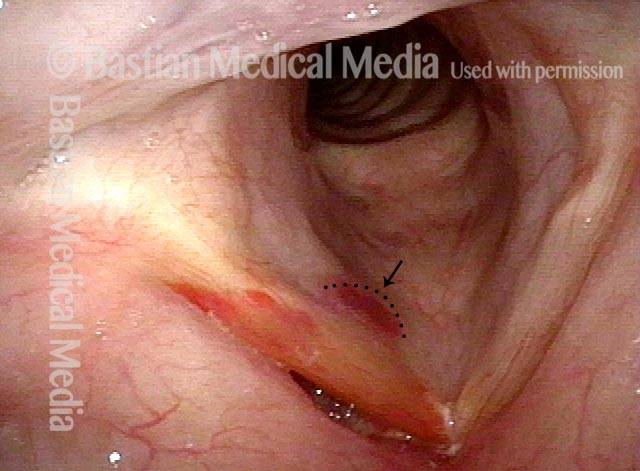
Vocal cord bruise / hemorrhage, after rest and surgery (4 of 4)

Vocal Cord Bruise / Hemorrhage
Vocal cord bruise / hemorrhage (1 of 2)

Vocal cord bruise / hemorrhage (2 of 2)

Vocal Cord Bruise / Hemorrhage, Before and After Rest
Vocal cord bruise / hemorrhage (1 of 6)

Vocal cord bruise / hemorrhage (2 of 6)
Vocal cord bruise / hemorrhage (3 of 6)
Vocal cord bruise / hemorrhage: after 2 weeks of rest (4 of 6)
After 2 weeks of rest (5 of 6)
After 2 weeks of rest (6 of 6)
Bruise Caused by Cough
Closer view of bruise (2 of 2)
Bruise caused by violent coughing (1 of 2)
Bruising from Sensory Neuropathic Cough
Bruising from SNC (1 of 1)
Vocal Cord Bruising From Coughing
Bruise from coughing (1 of 3)

Pre-phonatory instant (2 of 3)

Phonation (3 of 3)
The Evolution of Vocal Cord Bruising and Emergence of a Vulnerable Capillary
Margin swelling and bruising (1 of 2)
Six weeks later (2 of 2)