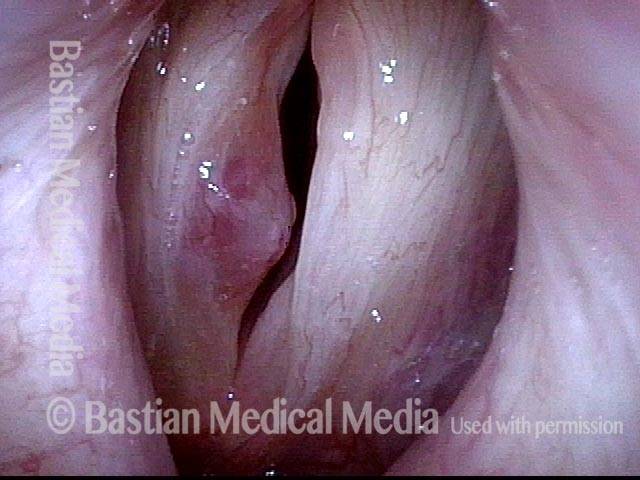
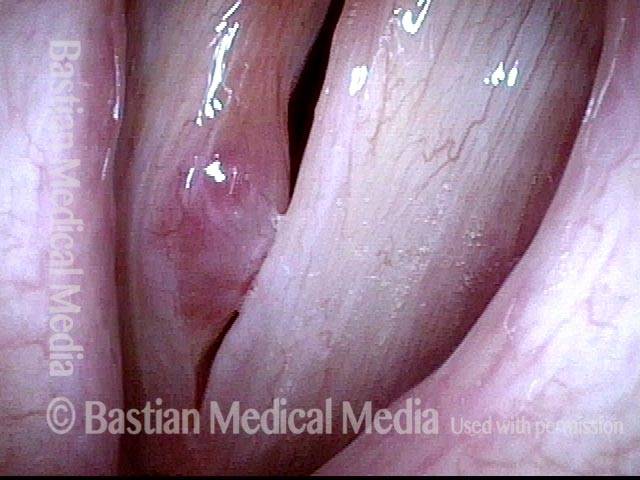
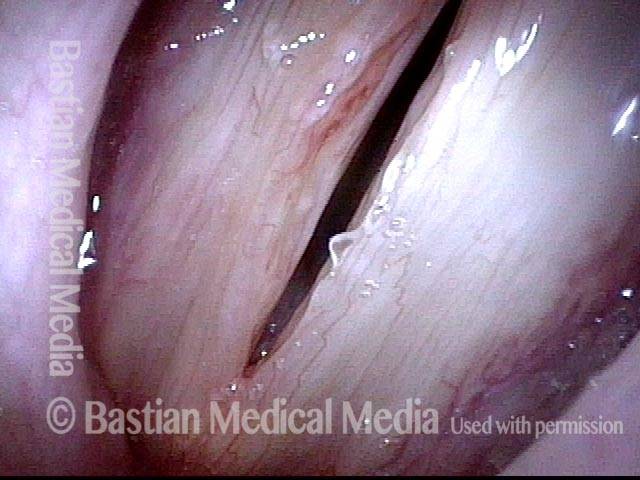
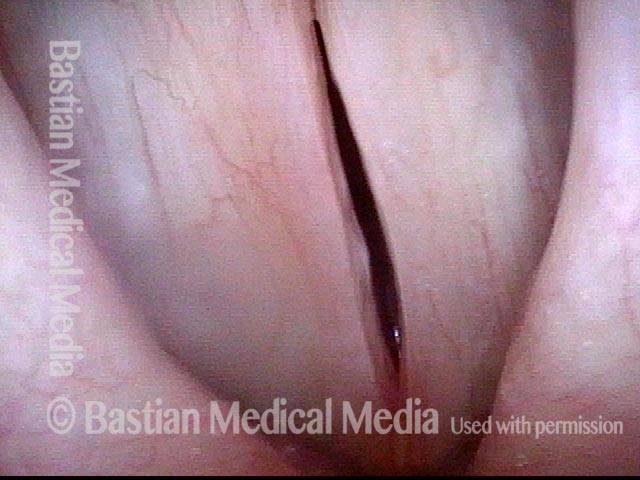
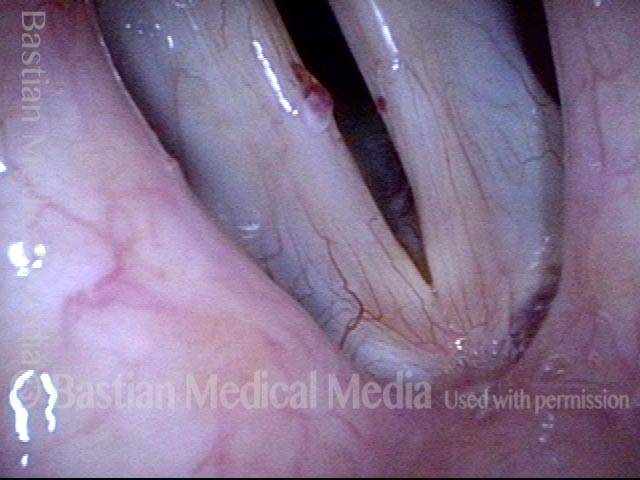
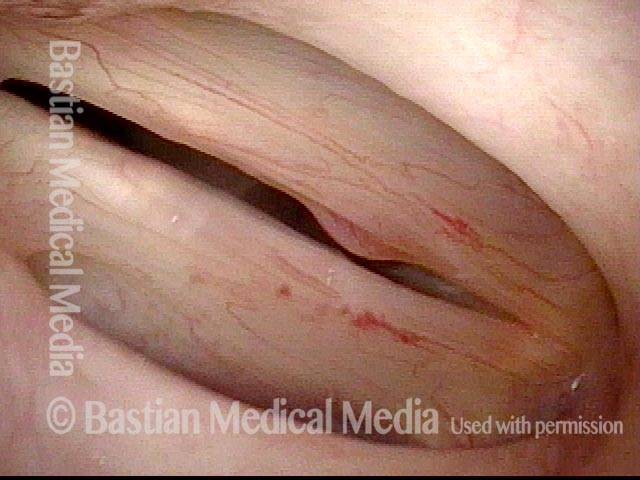
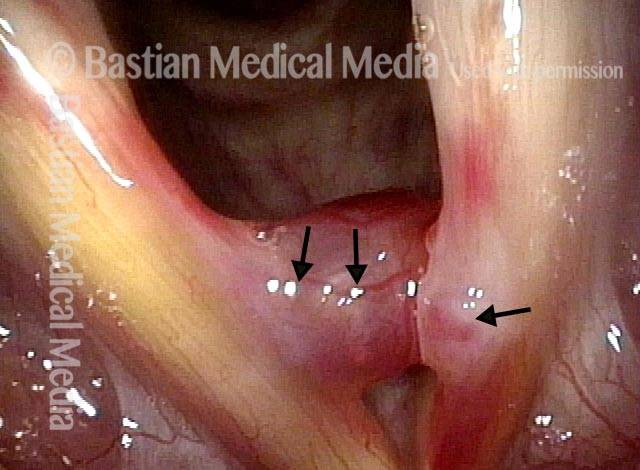
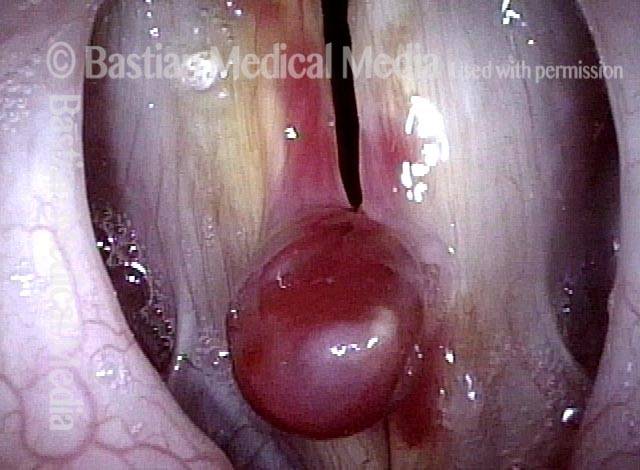
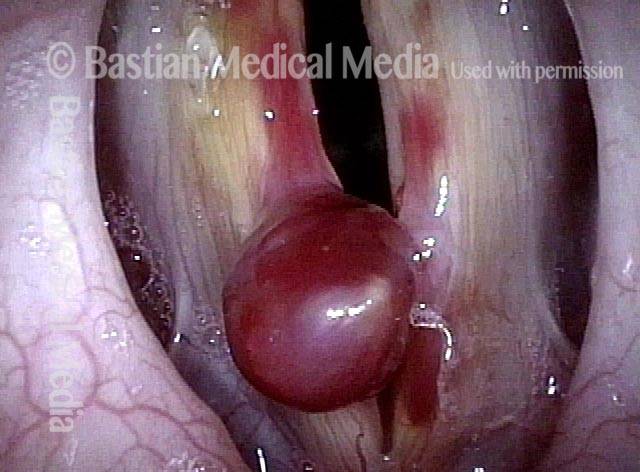
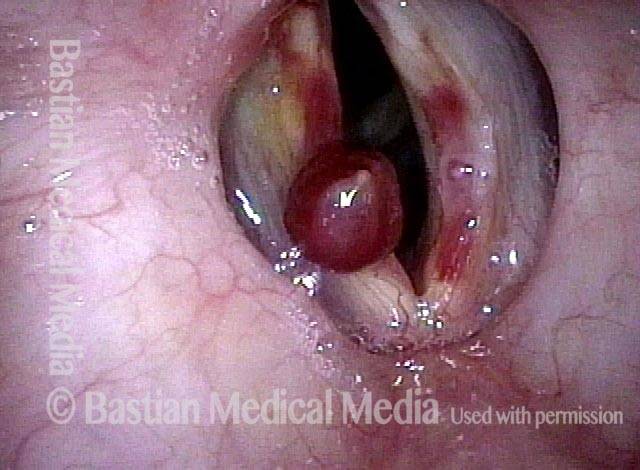
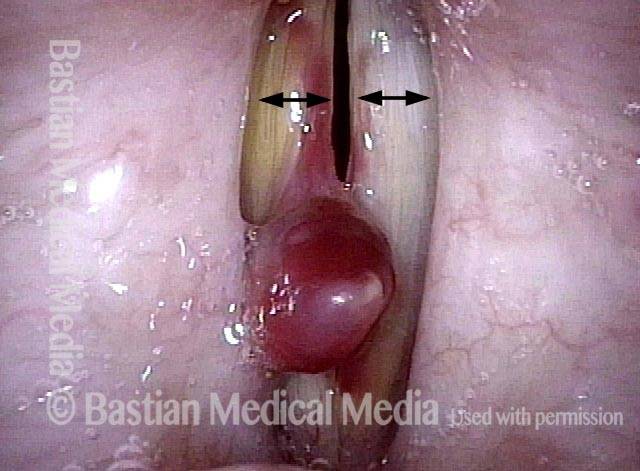
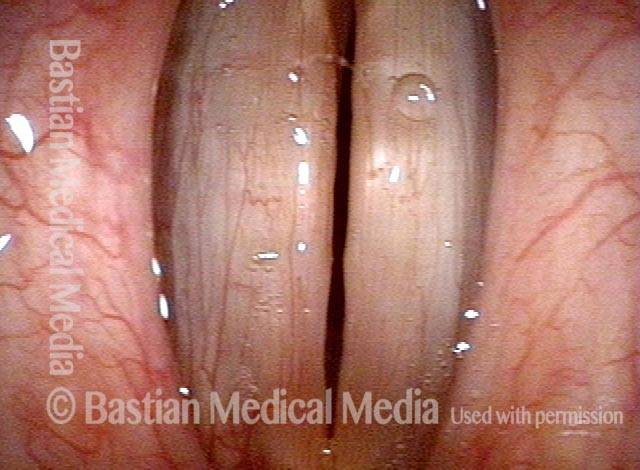
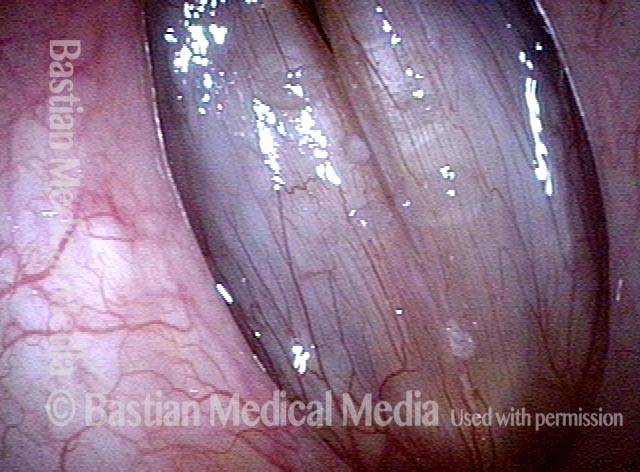
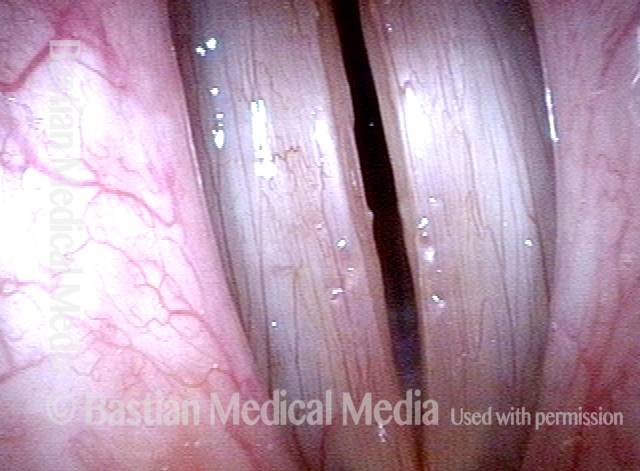
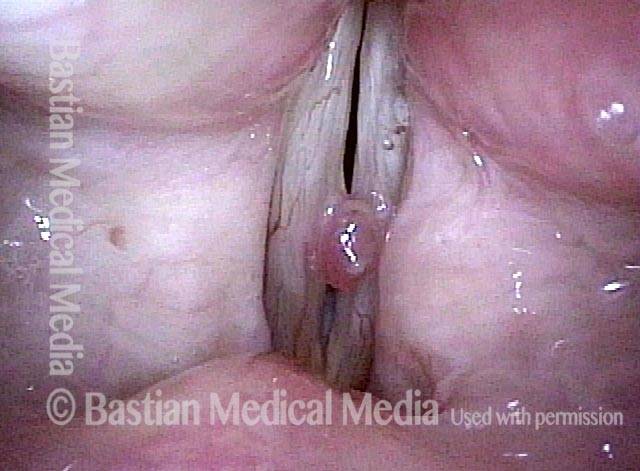
Hemorrhagic polyp is a vocal polyp that looks like a “blood blister” on the vocal cord. It may occur because of acute vocal trauma—sudden and extreme overuse of the voice—and may result in abrupt and fairly severe hoarseness that is persistent. In time, the blood may resorb and leave a translucent polyp; this kind of polyp may be prone to re-bruising intermittently.
Small hemorrhagic polyps may heal on their own, but usually require many months to do so. Larger ones should be surgically removed. Fortunately, the prognosis for full recovery after surgery is excellent.
Hemorrhagic polyp
Hemorrhagic polyp (1 of 2)

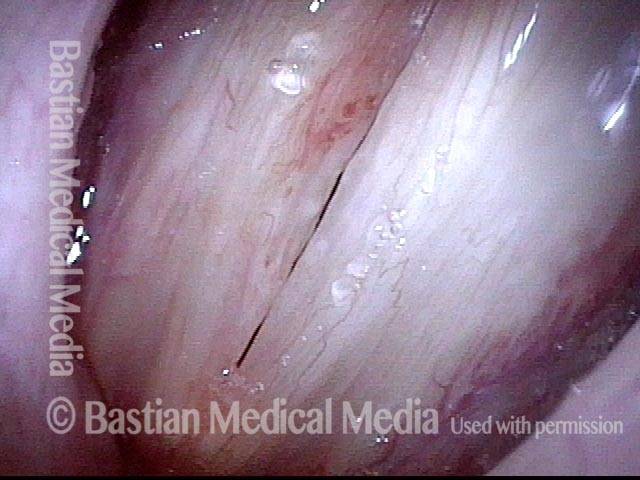
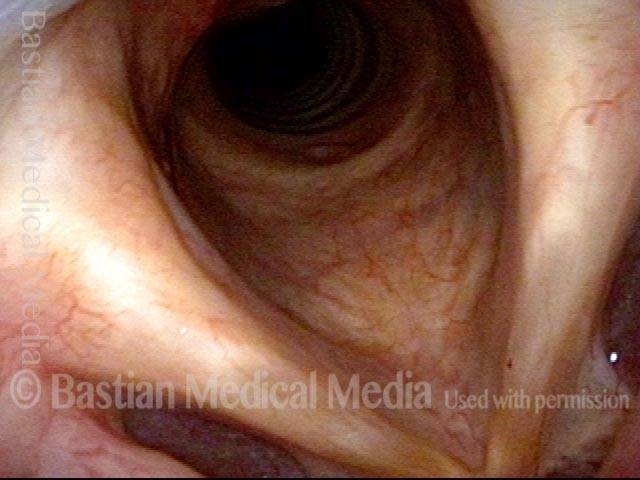
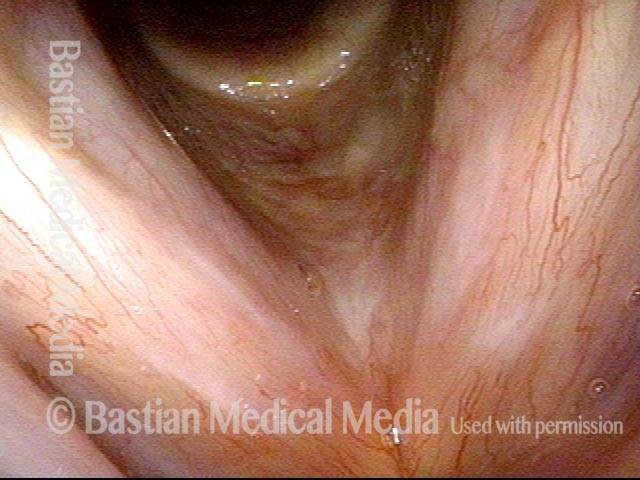
Hemorrhagic polyp (2 of 2)

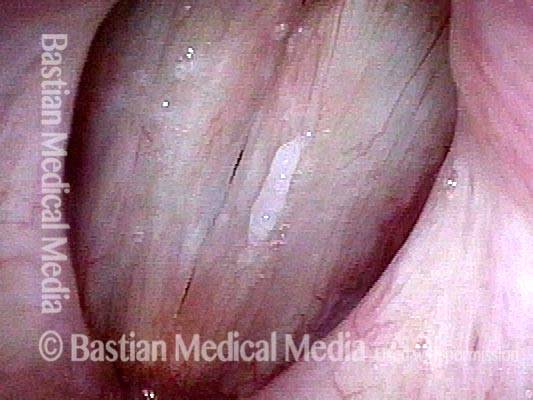
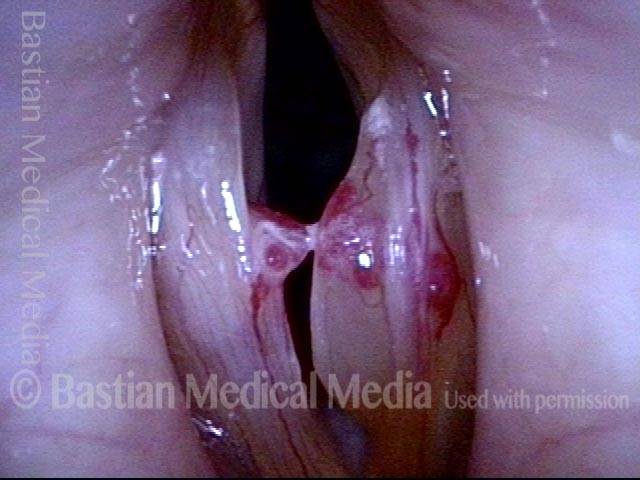
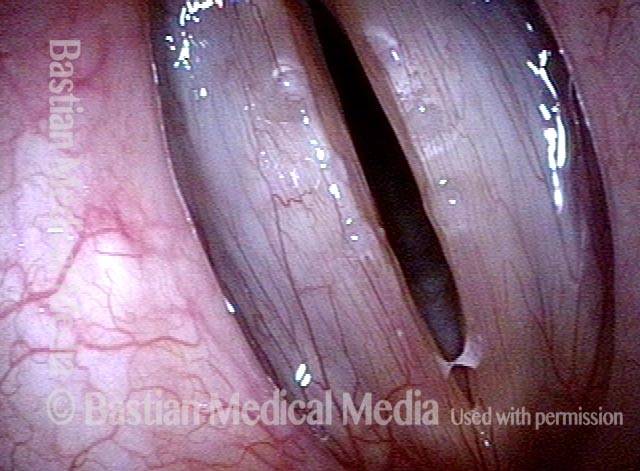
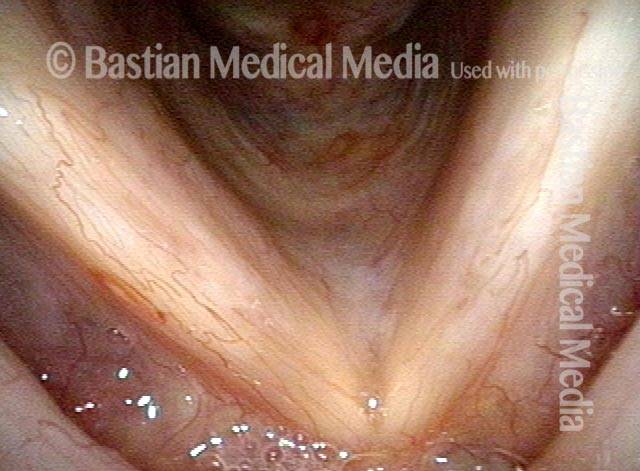
Example 2
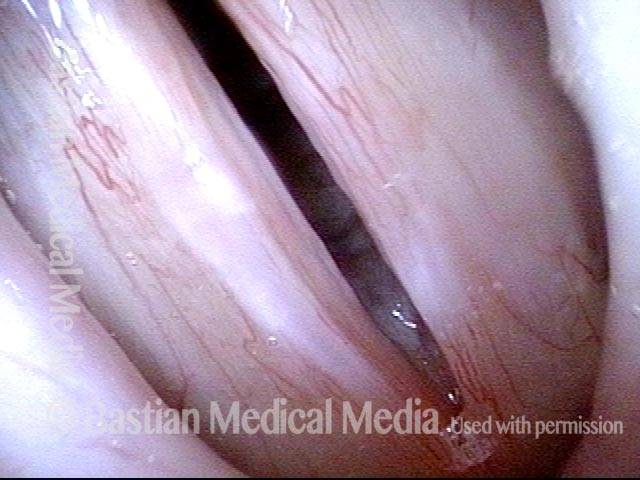
Hemorrhagic polyp (1 of 4)

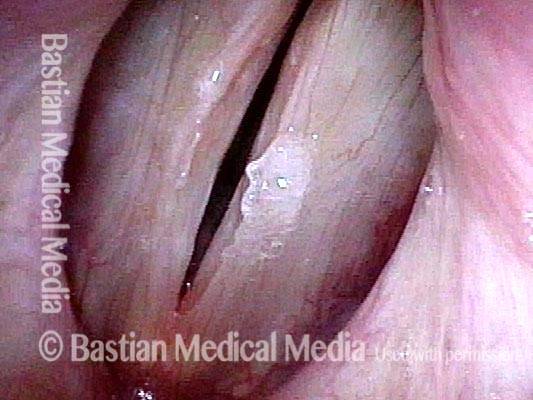
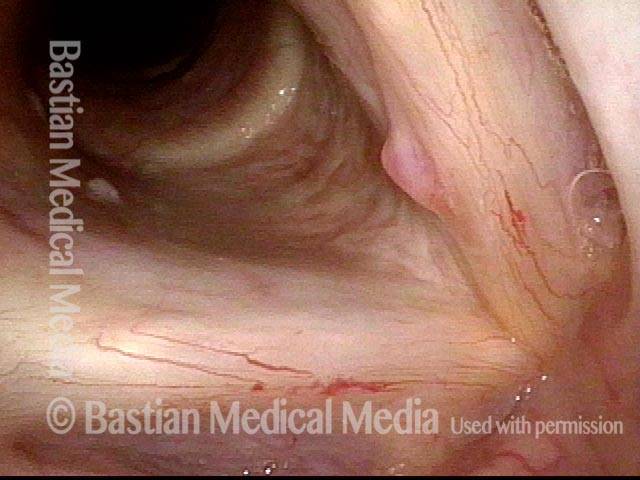
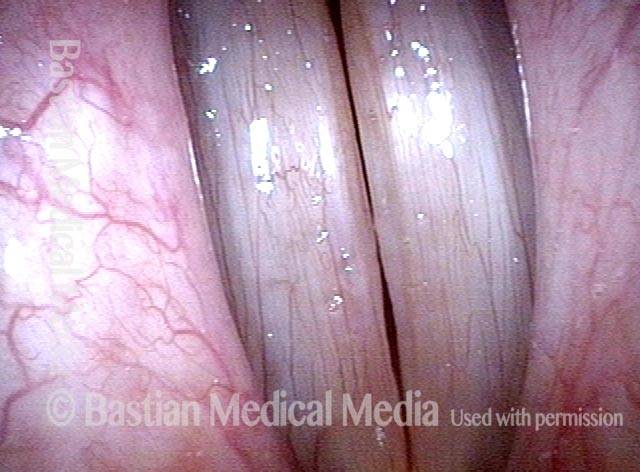
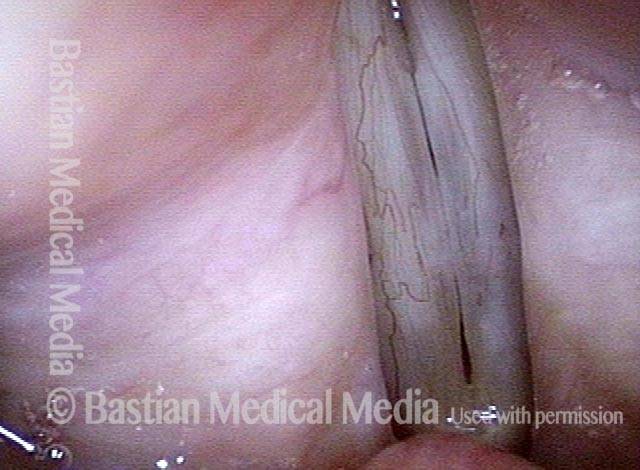
Hemorrhagic polyp (2 of 4)

Hemorrhagic polyp (3 of 4)

Hemorrhagic polyp (4 of 4)

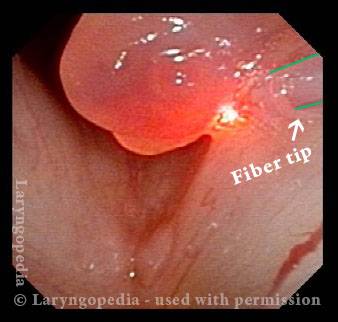
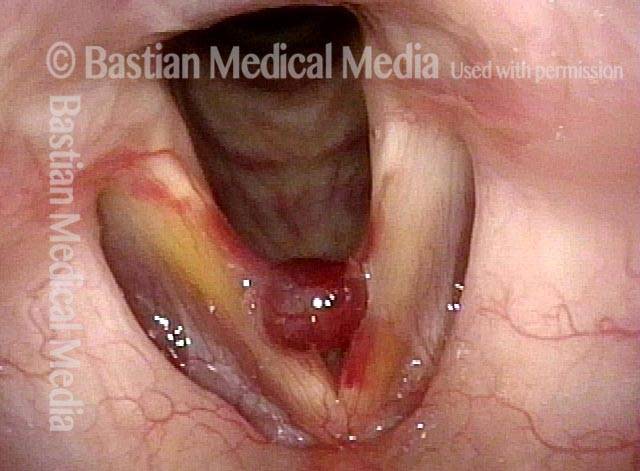
A Hemorrhagic Polyp that is Pedunculated (attached by a “stalk”)
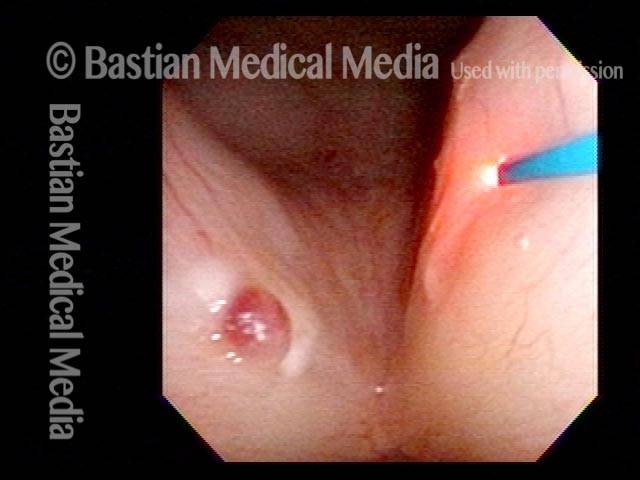
The thulium or other videoendoscopy lab (office-based) laser can be used for vocal cord injuries in persons who will not or cannot undergo general anesthesia. Reasons that patients might choose this options include severe medical issues such as:
- Heart disease that makes general anesthesia risky
- Morbid obesity
- Severe phobia of general anesthesia
- Anatomy that makes operative (O.R.) laryngoscopy difficult or impossible; enormous torus mandibularis, extreme retrognathism, kyphosis, and trismus are some examples.
Hemorrhagic polyp (1 of 4)

Laser removal (2 of 4)
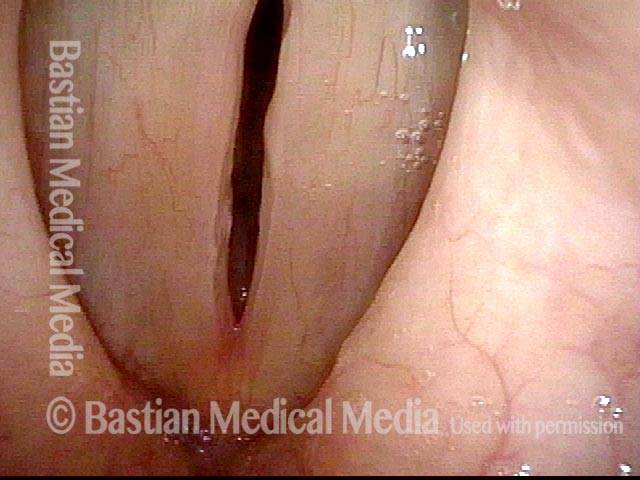
Voice immediately improves (3 of 4)

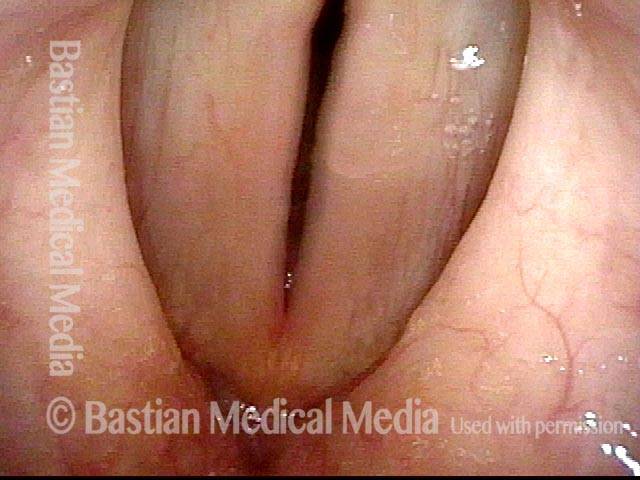
5 months post-laser (4 of 4)

Hemorrhagic Polyp, Before and after surgery
Hemorrhagic polyp (1 of 8)

Hemorrhagic polyp (2 of 8)
Hemorrhagic polyp (3 of 8)
Hemorrhagic polyp: 1 week after surgery (4 of 8)

Hemorrhagic polyp: 1 week after surgery (5 of 8)
Hemorrhagic polyp: 1 week after surgery (6 of 8)
Hemorrhagic polyp: 7 months after surgery (7 of 8)
Hemorrhagic polyp: 7 months after surgery (8 of 8)
Hemorrhagic Polyp, Treated By Thulium Laser
Hemorrhagic polyp, treated by thulium laser (1 of 8)

Hemorrhagic polyp, treated by thulium laser (2 of 8)
Hemorrhagic polyp, treated by thulium laser (3 of 8)

Hemorrhagic polyp, treated by thulium laser (4 of 8)

12 weeks after thulium laser treatment (5 of 8)
12 weeks after thulium laser treatment (6 of 8)
12 weeks after thulium laser treatment (7 of 8)

12 weeks after thulium laser treatment (8 of 8)
Capillary Ectasia and Hemorrhagic Polyp, Before and After Treatment
Capillary ectasia and hemorrhagic polyp (1 of 4)
Capillary ectasia and hemorrhagic polyp (2 of 4)

Capillary ectasia and hemorrhagic polyp, after treatment (3 of 4)
Capillary ectasia and hemorrhagic polyp, after treatment (4 of 4)

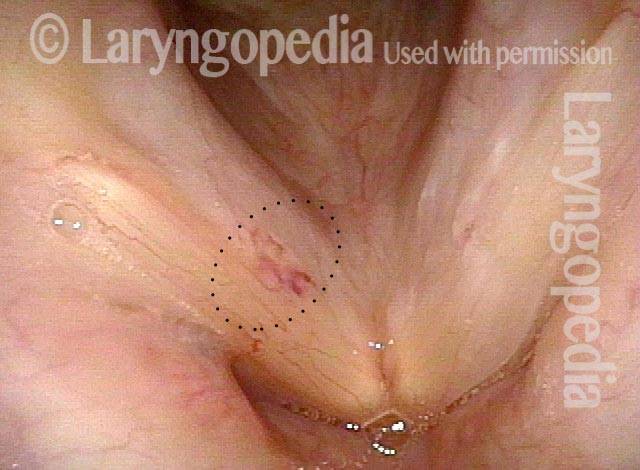
Capillary Ectasia and Hemorrhagic Polyp
Capillary ectasia and hemorrhagic polyp (1 of 2)

Capillary ectasia and hemorrhagic polyp (2 of 2)
Capillary Ectasia and Hemorrhagic Polyp, Treated by Thulium Laser
Capillary ectasia and hemorrhagic polyp (1 of 7)
Capillary ectasia and hemorrhagic polyp (2 of 7)
Capillary ectasia and hemorrhagic polyp, thulium laser treatment (3 of 7)

Capillary ectasia and hemorrhagic polyp, thulium laser treatment (4 of 7)

Capillary ectasia and hemorrhagic polyp, after treatment (5 of 7)
Vocal cord margin (6 of 7)

Capillary ectasia and hemorrhagic polyp, after treatment (7 of 7)
Hemorrhagic Polyp with Added Rumble at Low Pitch and Segmental Vibration at High Pitch
Young woman with hoarse voice (1 of 8)
Inspiratory phonation (2 of 8)
Closed phase (3 of 8)
Open phase (4 of 8)
Open phase, rumble (5 of 8)
Closed phase, segmental vibration (6 of 8)
One week post-op, prephonatory instant (7 of 8)
One week post-op, phonation (8 of 8)

Pre-op and Very Early Post-op Mucosal Match and Flexibility in Male Singer
Bilateral chronic injuries (1 of 8)
Closeup of injuries (2 of 8)
Post microsurgery (3 of 8)

Prephonatory instant (4 of 8)
Closed phase, A-flat 3 (5 of 8)
Open phase (6 of 8)
Dramatically improved match (7 of 8)
Equal mucosal flexibility (8 of 8)
Before and After Repair of Dilated Capillaries and Hemorrhagic Polyp
Hemorrhagic polyp (1 of 4)

Attempted voice production (2 of 4)
Post surgery (3 of 4)
Closed phase (4 of 4)
Pedunculation Defined in Pictures
Polyp (1 of 7)

Inspiration (2 of 7)

Closed position (3 of 7)

Phonatory view (4 of 7)

After removal (5 of 7)
Closed phase (6 of 7)

Open phase (7 of 7)

The Operated Side Often Looks Better Than the Unoperated…
Polyp (1 of 8)

Polyp rides upwards (2 of 8)

Post-surgery (3 of 8)

Prephonatory view (4 of 8)

Six weeks post-surgery (5 of 8)

Phonation (6 of 8)

Closed phase (7 of 8)

Open phase (8 of 8)