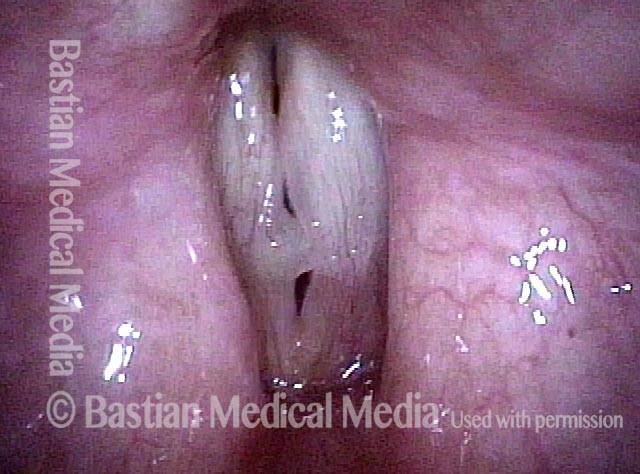
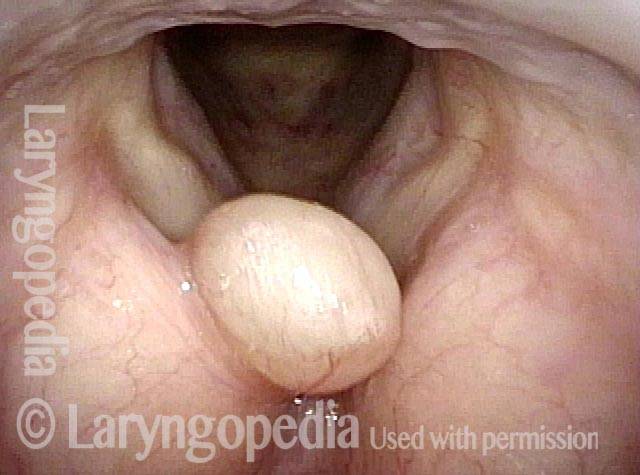
Vocal polyp is a large swelling on the vocal cord that typically occurs unilaterally—that is, without a similar swelling on the opposite cord. The term vocal polyp is somewhat imprecise, but vocal polyps can be distinguished from a similar kind of swelling, vocal nodules, in at least two ways:
- Polyps tend to be larger than nodules
- Polyps occur unilaterally or are markedly larger than an injury of the opposite vocal cord, whereas nodules occur in pairs and are usually similar in size.
Both vocal polyps and nodules are caused at least in part by vibratory trauma, due to vocal overuse that is acute (with polyps) or chronic.
A vocal polyp disrupts the voice’s clarity and other capabilities by interfering with accurate approximation of the vocal cords during phonation. A polyp may also add mass to the vocal cord, thereby dropping the pitch range available to the voice. Polyps may be referred to as hemorrhagic, pedunculated, and so forth.
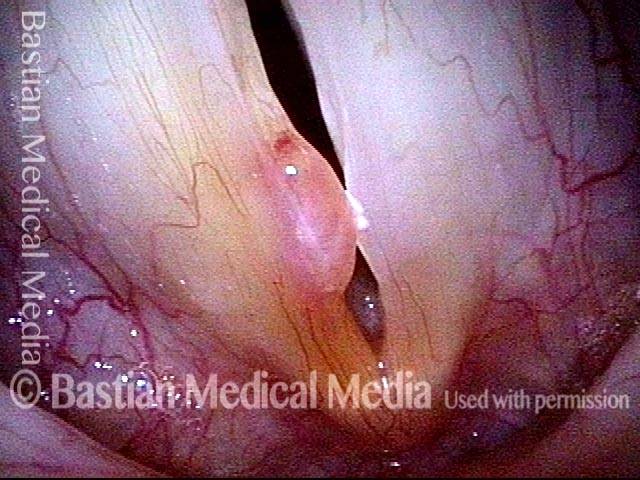
Vocal Polyp, Removed and then Recurring
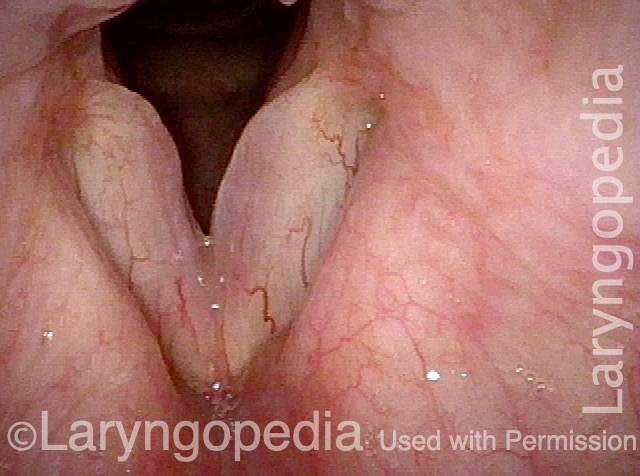
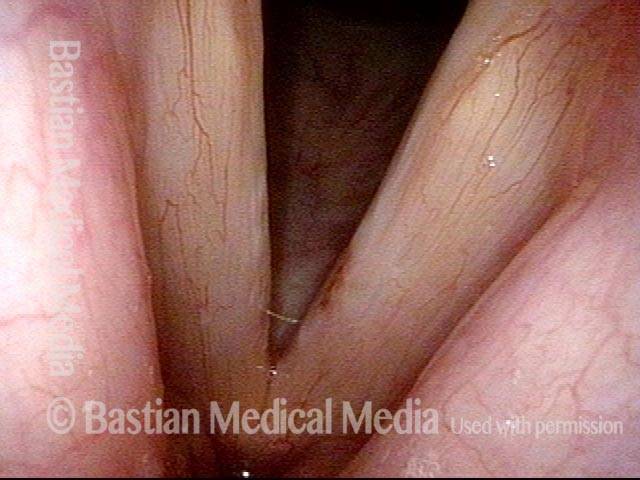
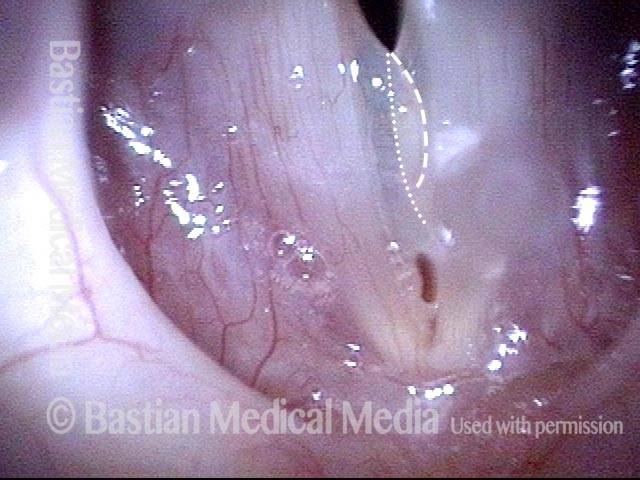
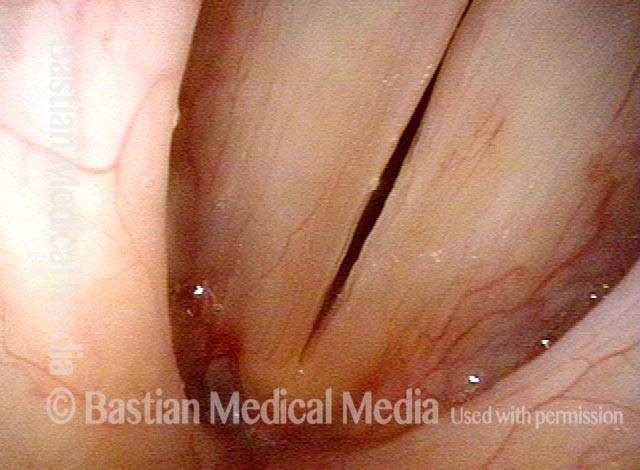
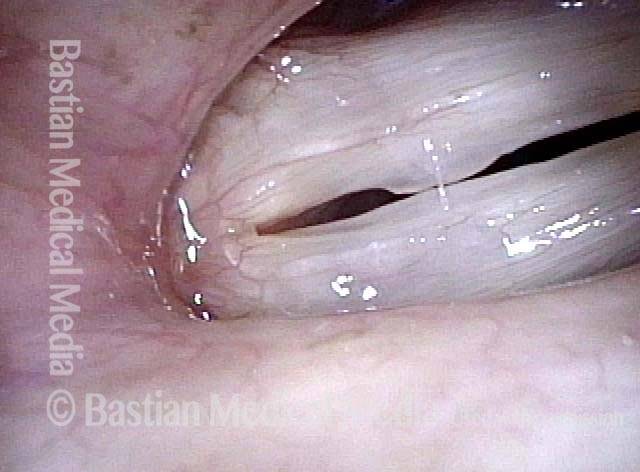
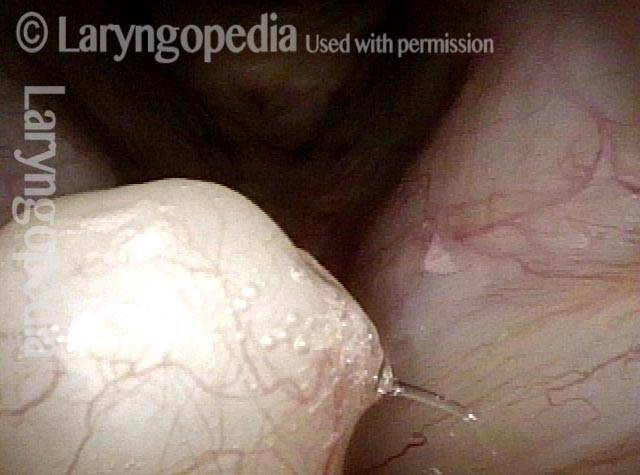
Vocal polyp (1 of 4)
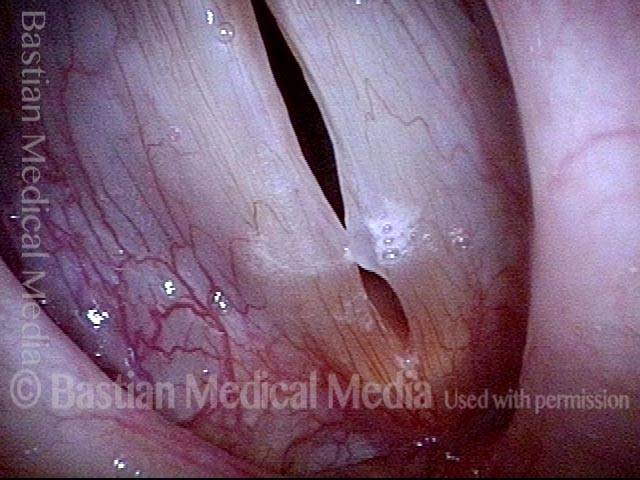
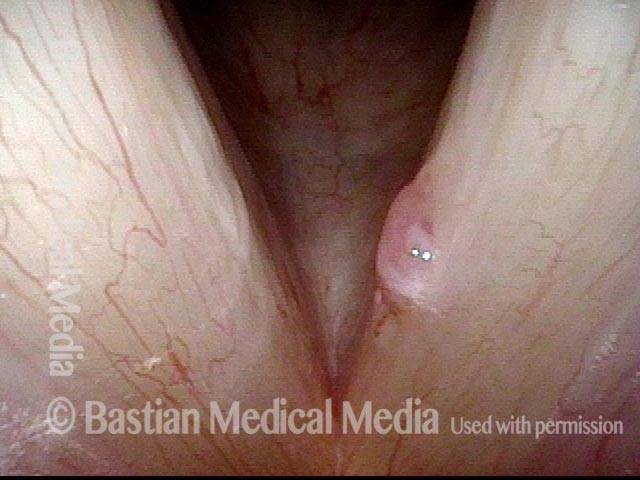
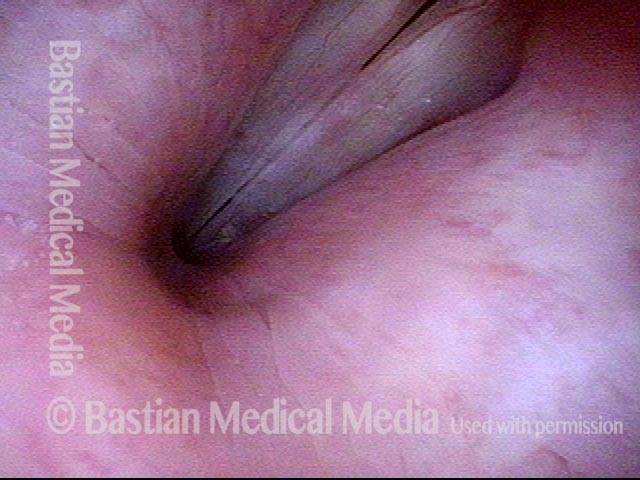
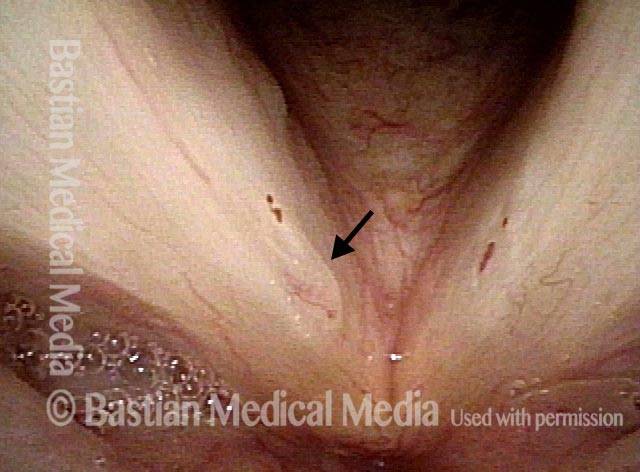
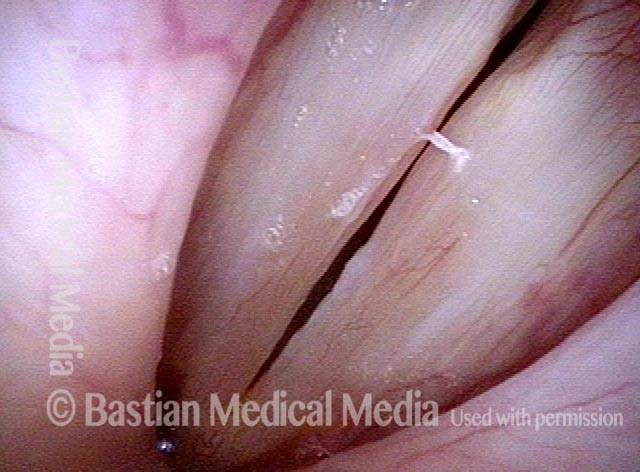
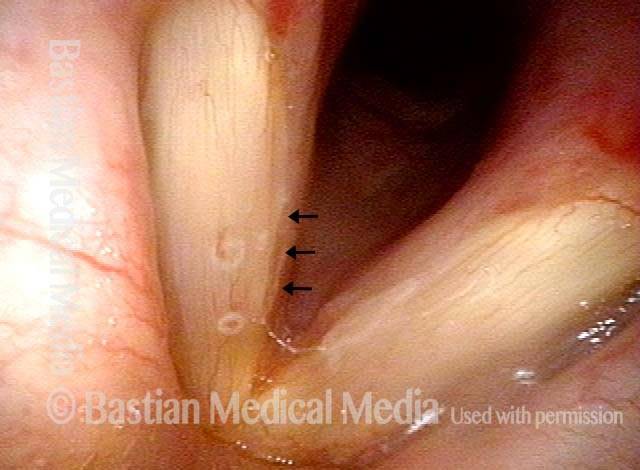
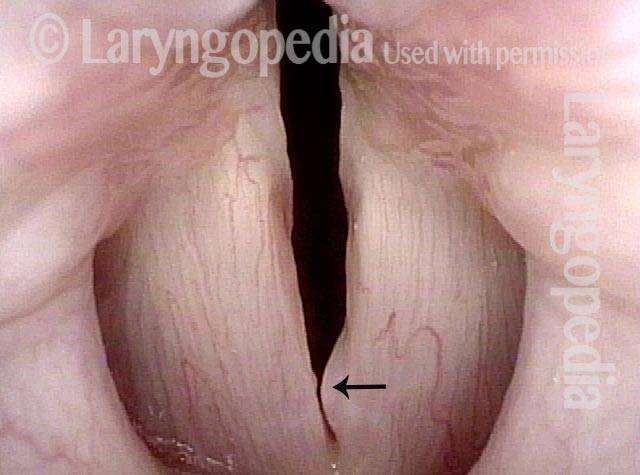
Vocal polyp (2 of 4)
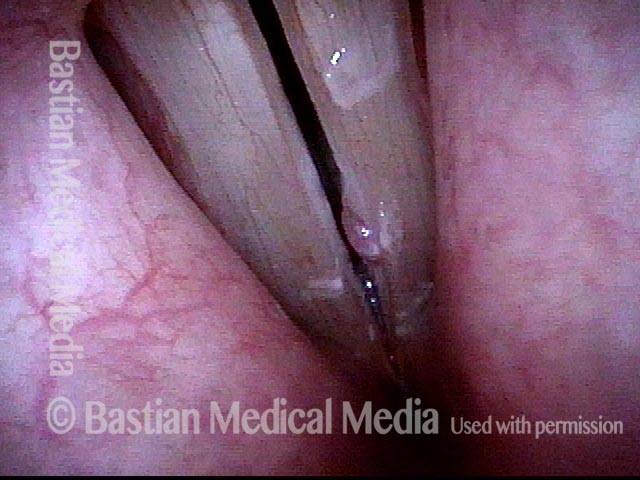
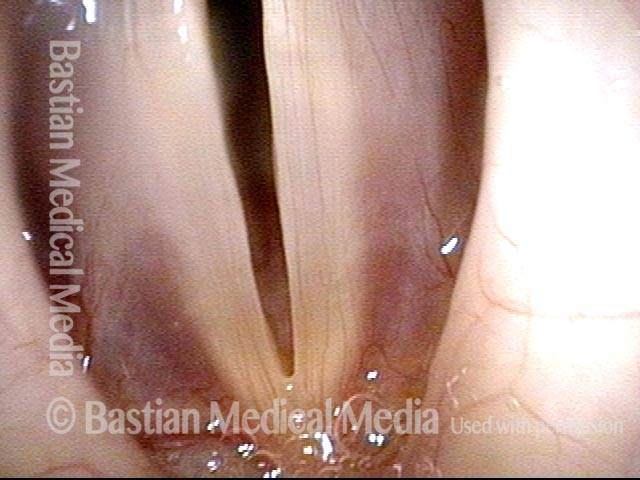
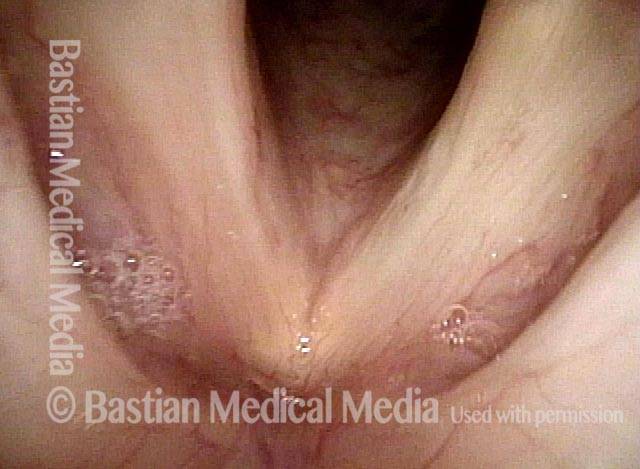
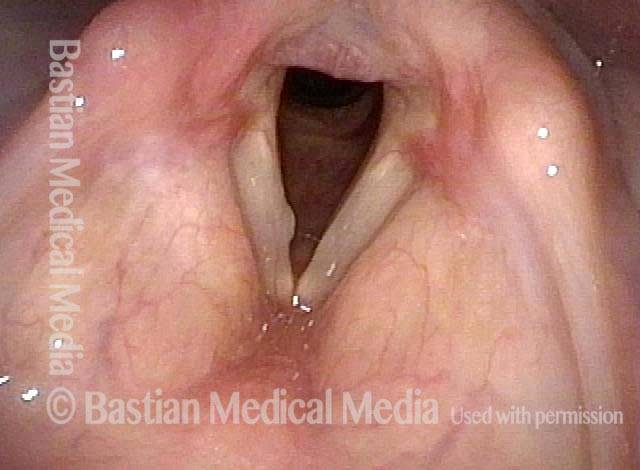
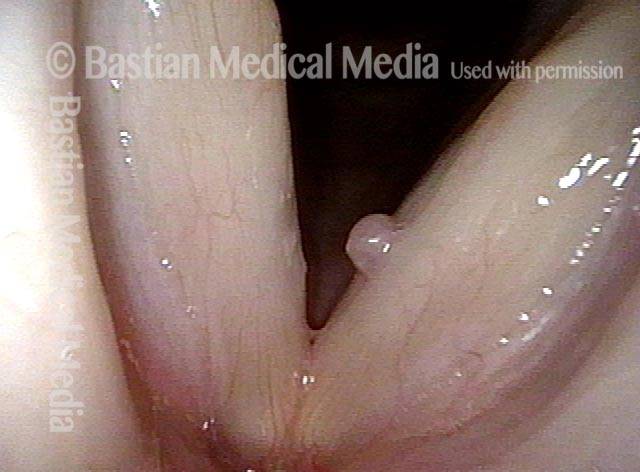
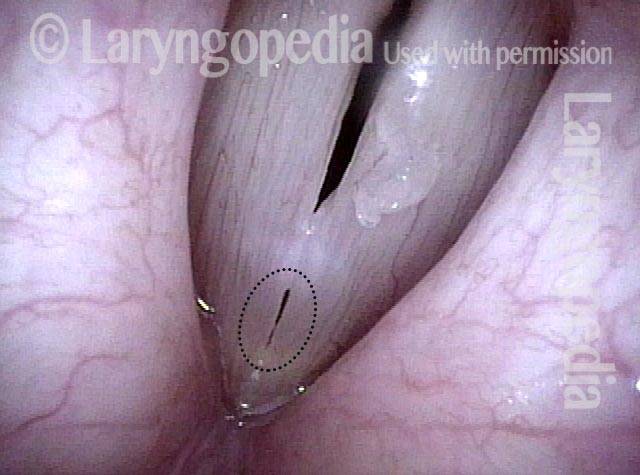
Vocal polyp, one week after surgical removal (3 of 4)

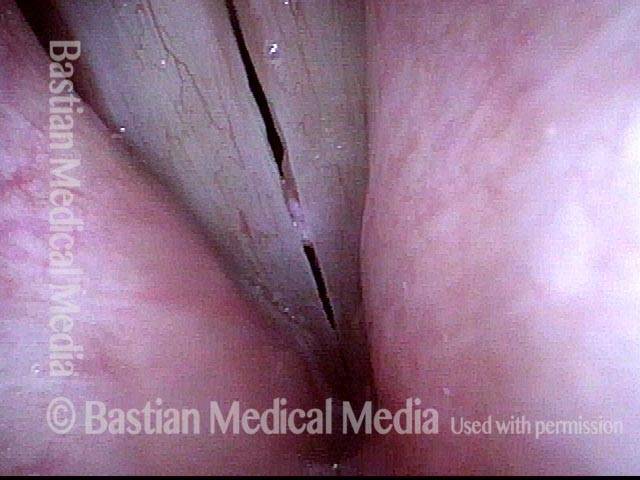
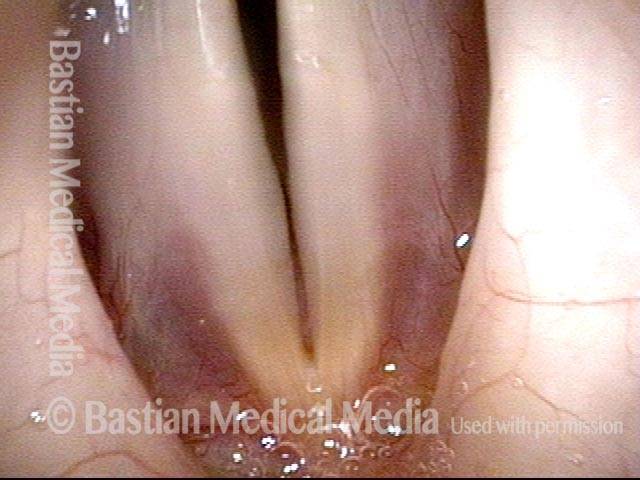
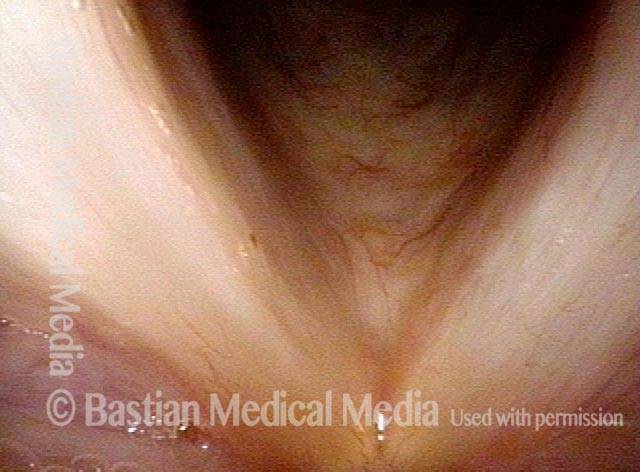
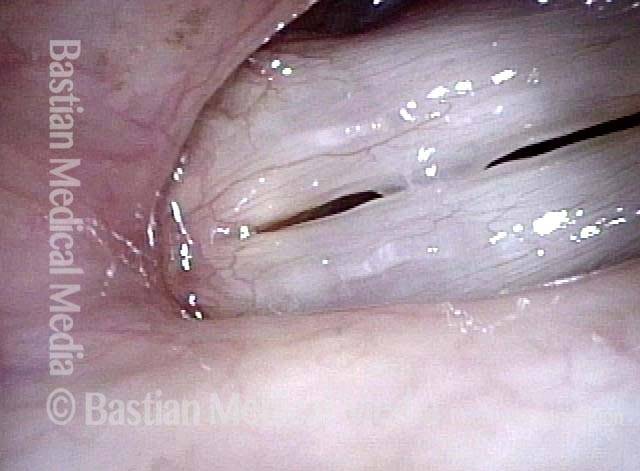
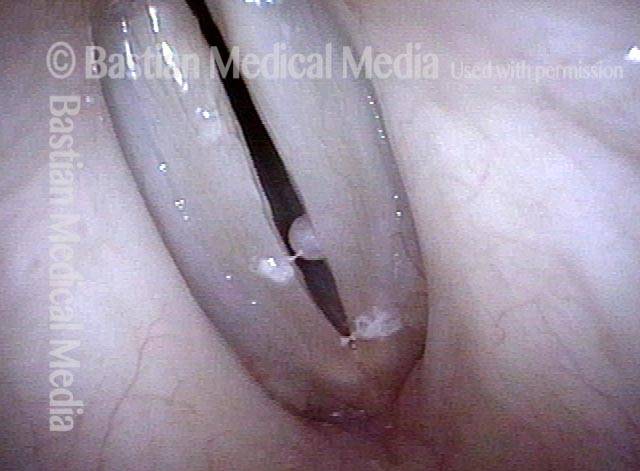
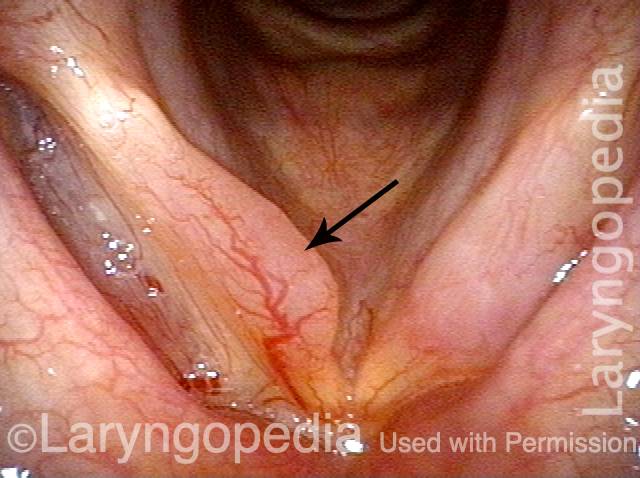
Vocal polyp, subsequent new injury (4 of 4)
Vocal Polyp, Before and After Surgery
Vocal polyp (1 of 6)
Vocal polyp (2 of 6)
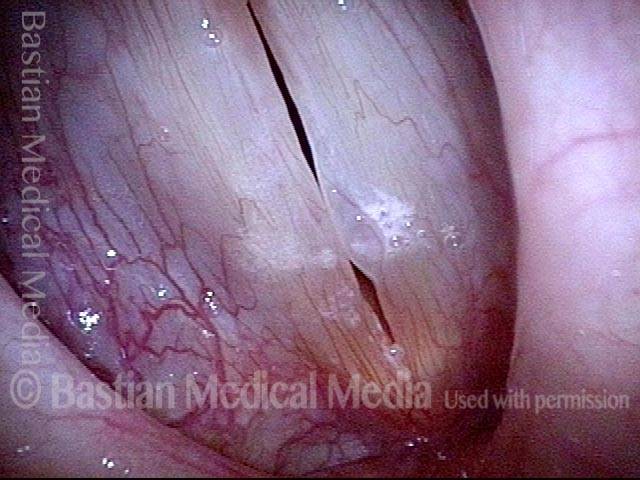
Vocal polyp (3 of 6)
Vocal polyp, surgically removed (4 of 6)
Vocal polyp, surgically removed (5 of 6)

Vocal polyp, surgically removed (6 of 6)
Example 2
Vocal polyp (1 of 2)

Vocal polyp, surgically removed (2 of 2)

Example 3
Vocal polyp (1 of 6)

Vocal polyp (2 of 6)

Vocal polyp, surgically removed (3 of 6)
Vocal polyp, surgically removed (4 of 6)
Vocal polyp, surgically removed (5 of 6)
Vocal polyp, surgically removed (6 of 6)
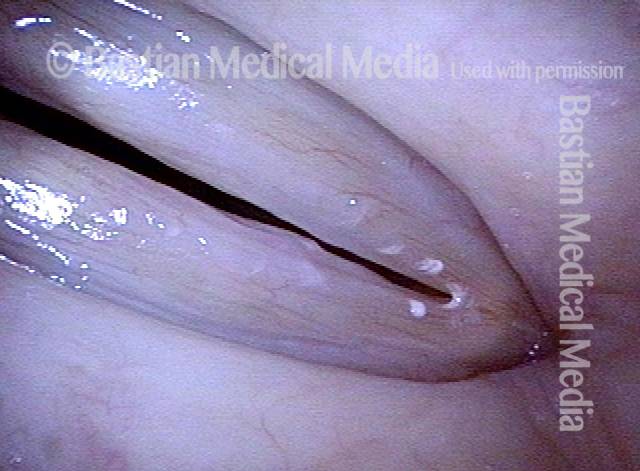
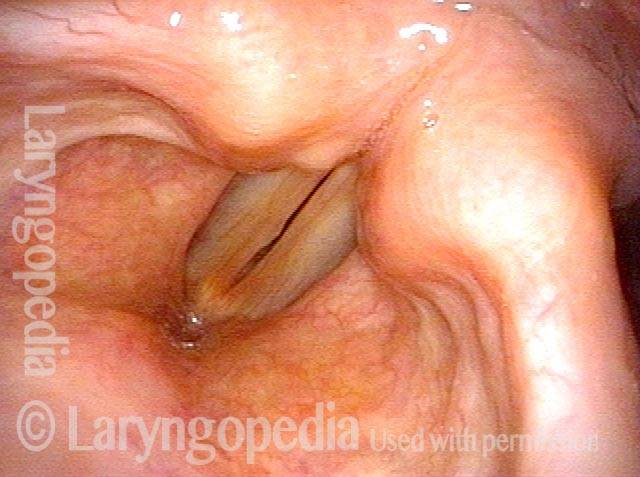
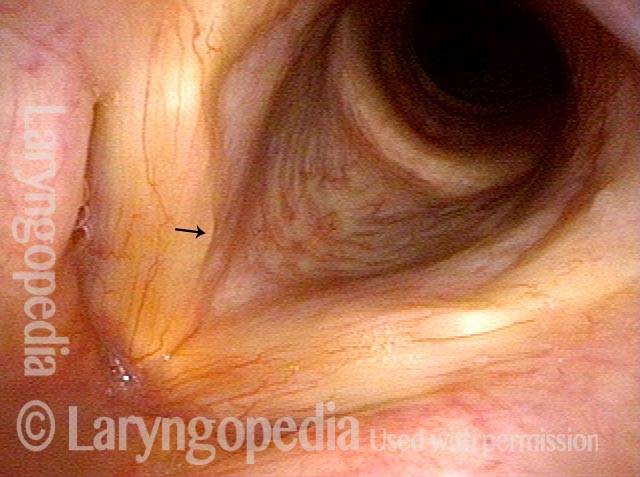
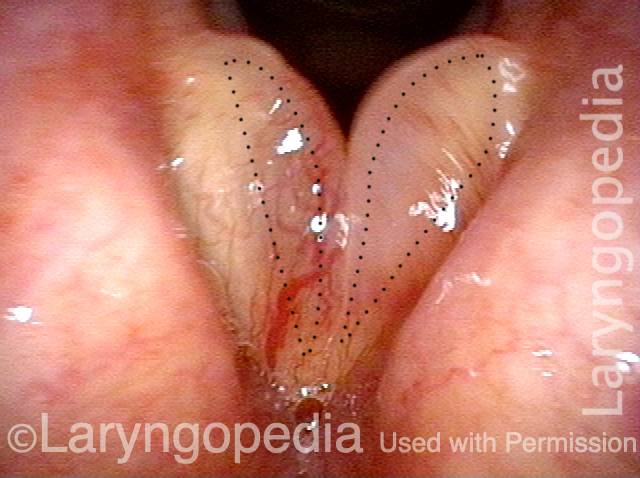
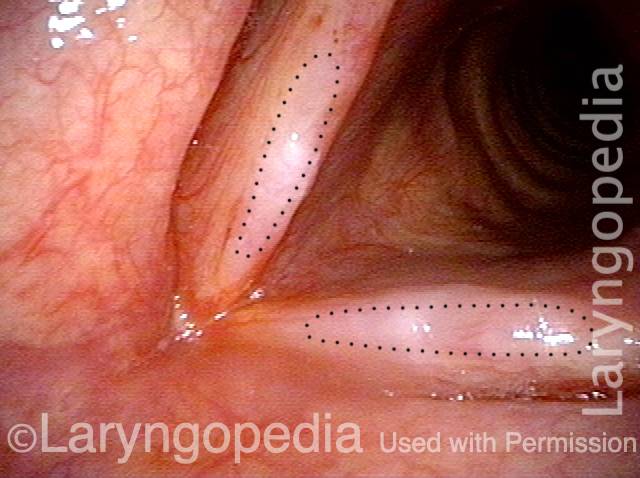
Translucent Polyp
Translucent polyp (1 of 4)

Translucent polyp (2 of 4)
Translucent polyp (3 of 4)
Translucent polyp (4 of 4)
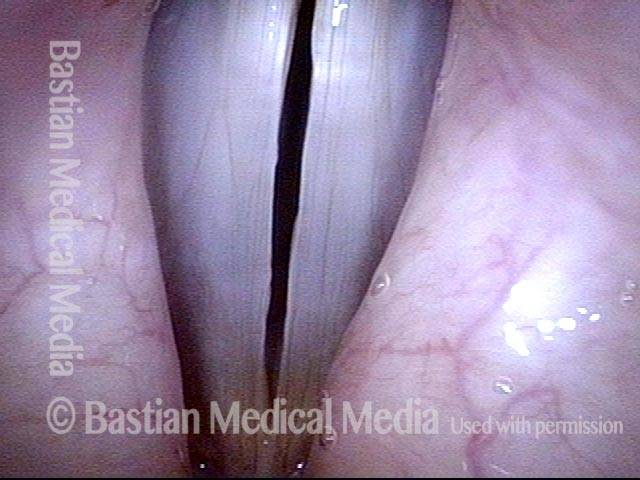
Opera Singer’s Polyp Removed with Restoration of Original Capabilities
Polyp and capillary ectasia (1 of 8)
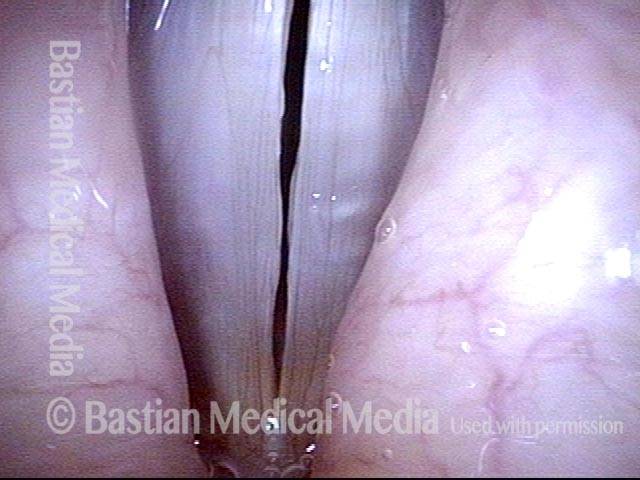
Prephonatory instant (2 of 8)

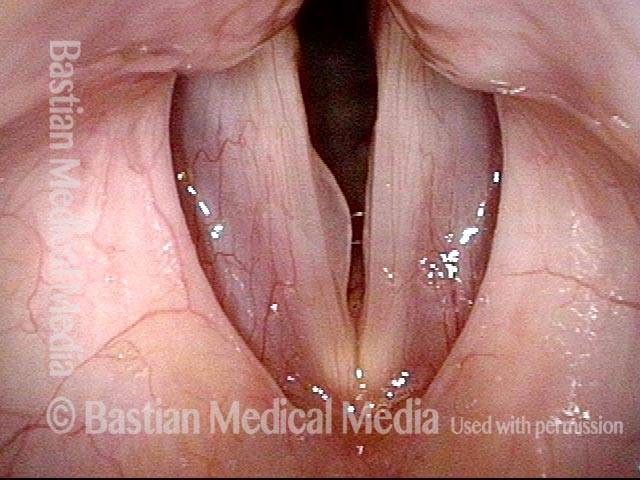
One week post-op (3 of 8)
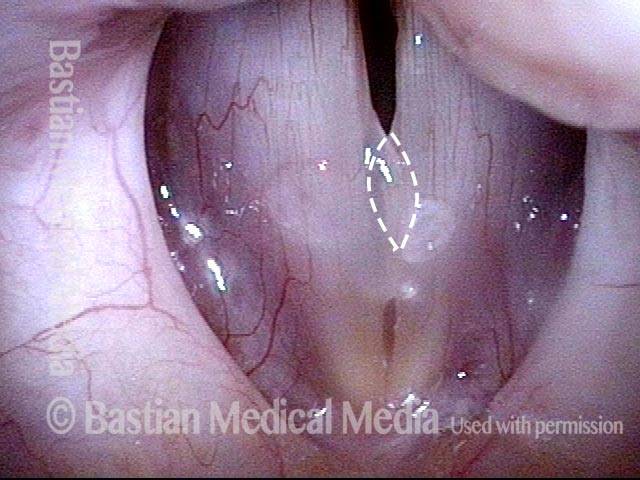
Prephonatory instant (4 of 8)

One month post-op (5 of 8)
Prephonatory instant (6 of 8)
Closed phase (7 of 8)

Open phase (8 of 8)
An Actress’ Polyp Before and Hours After Surgical Removal
Vocal cord polyp (1 of 8)
Closer view (2 of 8)

Closed phase (3 of 8)
Open phase (4 of 8)
24 hours post surgery (5 of 8)

Primary “wound” (6 of 8)
Closed phase (7 of 8)

Open phase (8 of 8)

Operated Cord Looks Better than the Unoperated Cord
Singer with chronic hoarseness (1 of 4)
Attempting phonation (2 of 4)
One week post surgical removal (3 of 4)
Open phase (4 of 4)
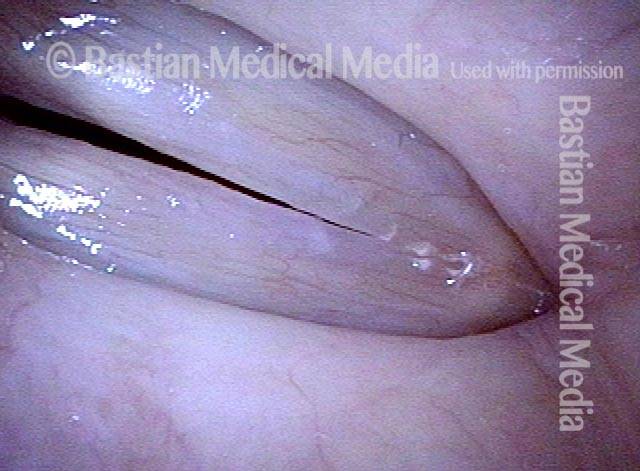
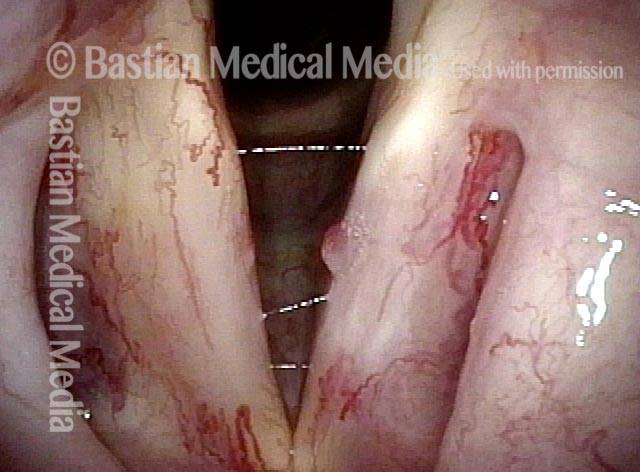
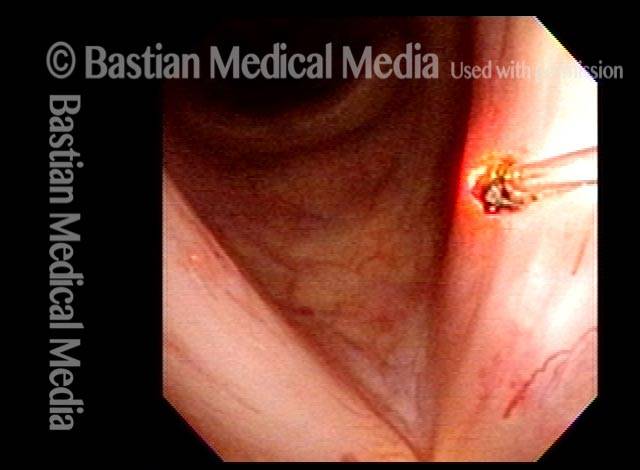
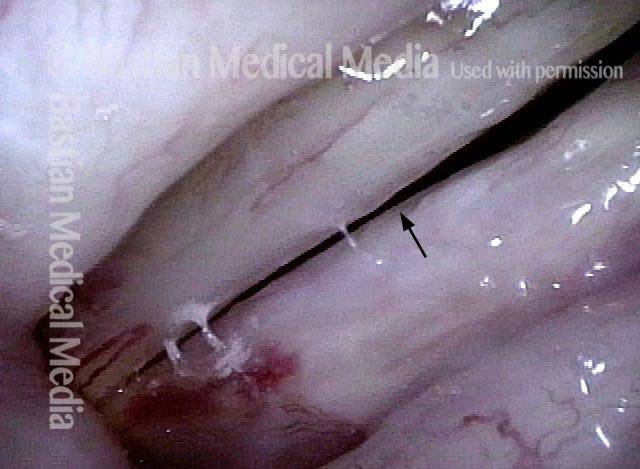
Office Laser of Post-radiation Telangiectatic Polyp
Post-radiation telangiectasias (1 of 4)
Pulsed-KTP coagulation (2 of 4)
“Polyp” pulled off (3 of 4)

Three weeks later (4 of 4)
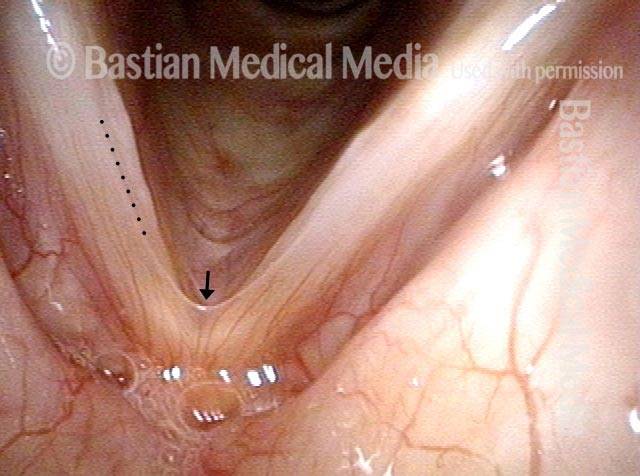
Nuances “Gleaned” from Daily Examinations
Vocal “overdoer” (1 of 4)
Inspiratory phonation (2 of 4)
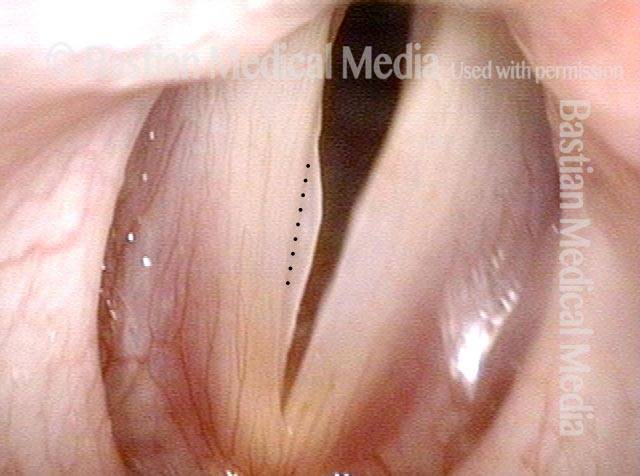
Translucent polyp (3 of 4)

Open phase (4 of 4)

The Mucosa’s Expression of Injury Varies
Vocal cord injuries (1 of 4)

Narrow band lighting (2 of 4)

Strobe lighting (3 of 4)
Phonation (4 of 4)
The Power of “Close-clear” Not “Far-fuzzy” to See a Polyp
Disant view (1 of 4)
Closer view (2 of 4)
Close-clear view (3 of 4)

Open phase (4 of 4)

Polyp or Cyst?
Hoarseness (1 of 4)

Position of lesion (2 of 4)
Close view (3 of 4)
Anterior saccular cyst (4 of 4)

Tiny Vibrating Segment Gives Tiny Tin Whistle Voice
Prephonatory instant (1 of 6)
Phonation (2 of 6)

Gaps due to nodules (3 of 6)

Open phase (4 of 6)

“Tin whistle” sound (5 of 6)
“Tin whistle” at open vibration (6 of 6)

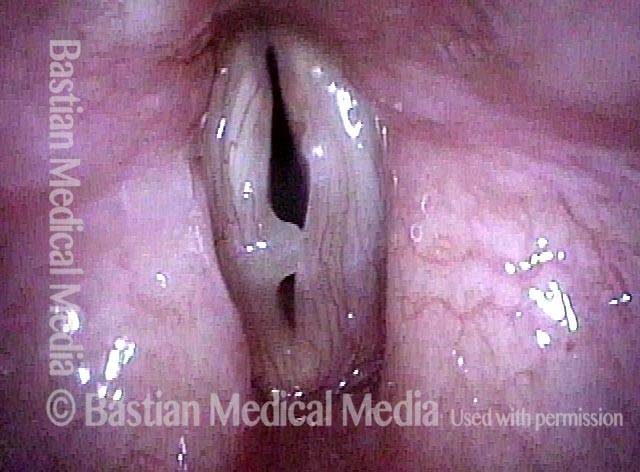
Smoker’s Polyp Reduction Improves Voice Even Though the Larynx Result May not be “Pretty”
Smokers Polyp (1 of 5)
Reine’s edema (2 of 5)
A week after surgery (3 of 5)
Residual Reinke’s edema (4 of 5)

Residual submucosal edema (5 of 5)