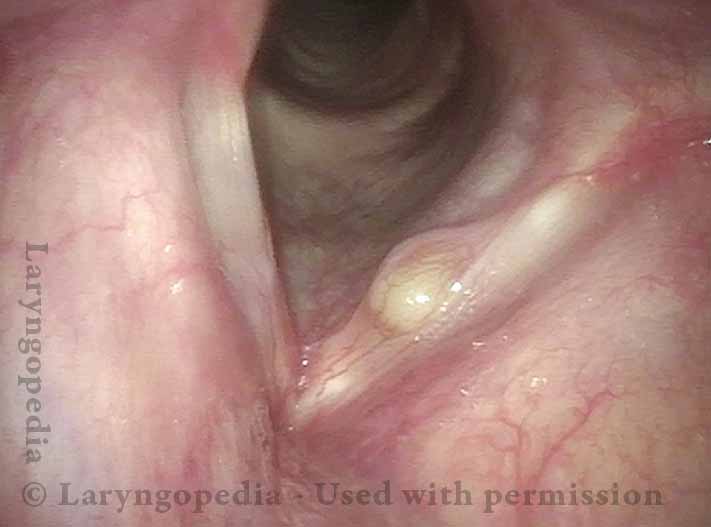
Image Example
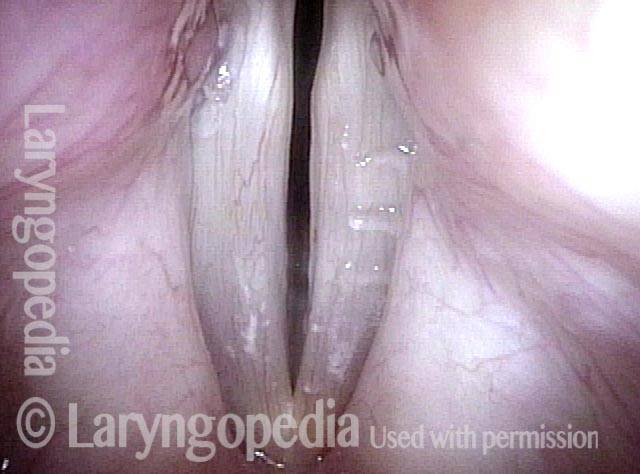
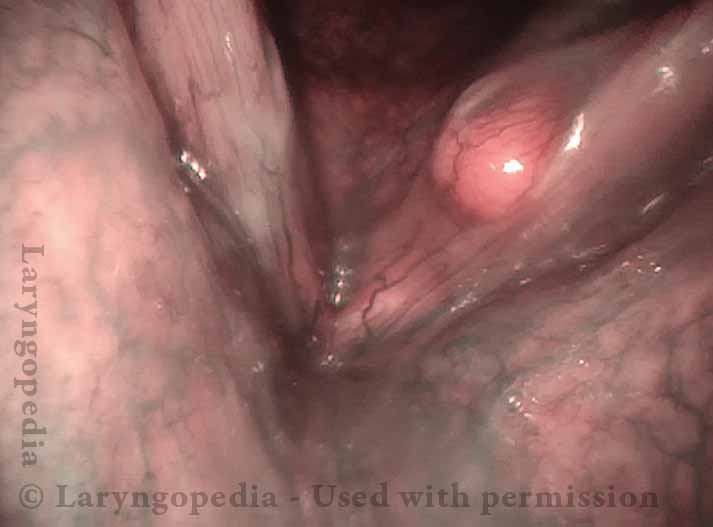
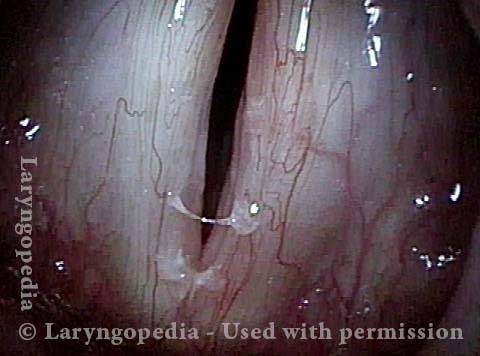
After laser excision of early vocal cord cancer, left vocal cord (right of image), a small mucus gland became plugged. This could instead be mistaken as a polyp, but a polyp does not fit this man's quiet nature and minimal vocal commitments. Note that the lesion is below the point of maximum vibratory contact that would produce a polyp. This man's voice is excellent.

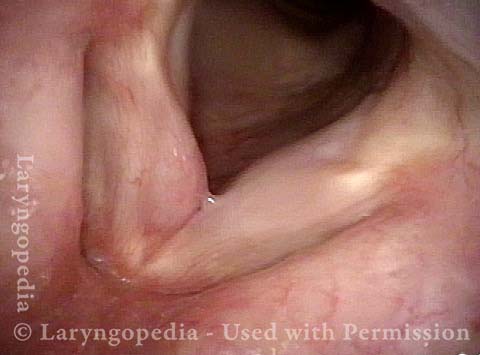
Before and After Mucus Retention Cyst Removal
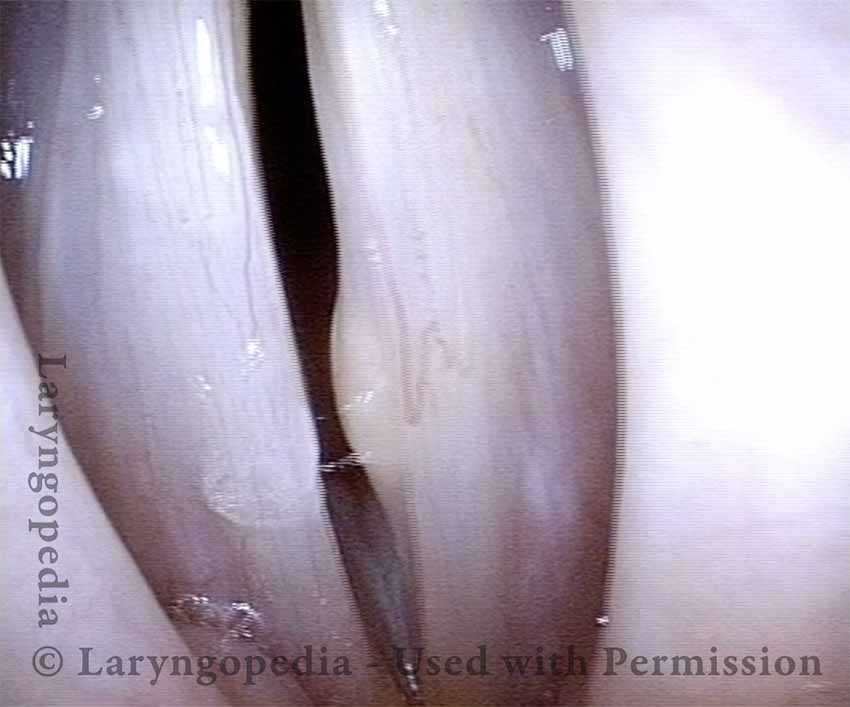
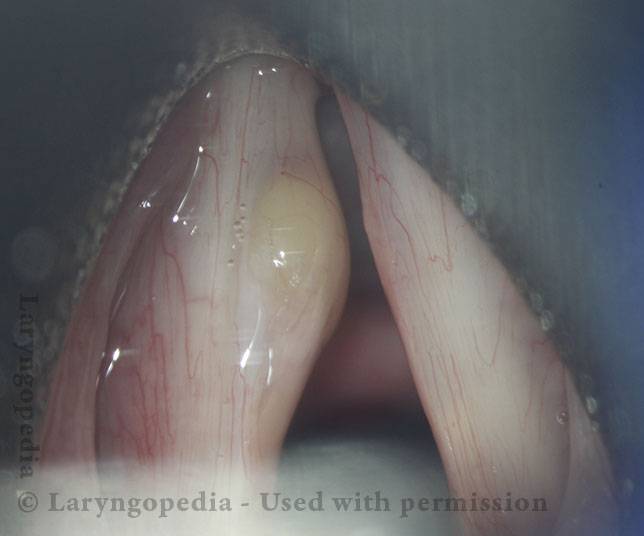
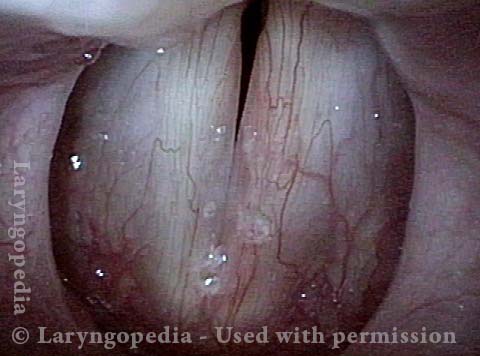
This patient has experienced chronic hoarseness and diplophonia (double pitch) for the past two years, with significant loss of her upper range. Examination shows a mucus-retention cyst on the left vocal cord (right of photo). The etiology of such cysts is usually not vibratory injury, but simple plugging of a mucus gland. Still, the fact that a mucus-retention cyst can occur in a quiet introvert does not exclude its occurrence in an extrovert. That is the situation here, as evidenced by the reactive nodule on the right vocal cord (left of photo).
Accordingly, while not every patient with a mucus-retention cyst requires speech therapy, this particular patient does. Therapy goals include:
- Preparing the patient for surgery;
- Instruction in early postoperative vocal voice use parameters and strategies
- Reducing the risk of future overuse and nodule formation.
In an “introvert,” a single session—or none—may be appropriate. In this extrovert, approximately six sessions is typically sufficient. The risk of cyst recurrence is determined primarily by the completeness of surgery not by future overuse.
Mucus Retention Cyst (1 of 15)

Segmental Vibration, Open Phase (2 of 15)

Segmental Vibration, Closed Phase (3 of 15)

Full-cord Vibration, Open Phase (4 of 15)
Full-cord Vibration, Close Phase (5 of 15)

Inverted Operative View (6 of 15)

Xylocaine Injection (7 of 15)

Dissection begins (8 of 15)

Dissection continues (9 of 15)

Dividing the last strand of attachment (10 of 15)

The Intact Cyst Has Been Removed (11 of 15)

Overlying Mucosa Preserved (12 of 15)

Mucosa Being Released (13 of 15)

Three Months Postop, Open Phase of Vibration (14 of 15)

Three Months Postop, Closed Phase of Vibration (15 of 15)

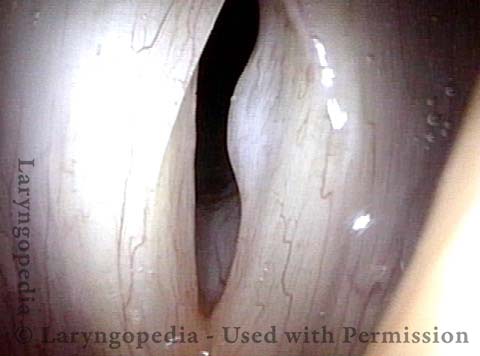
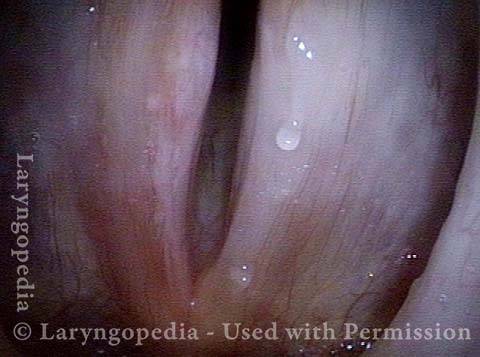
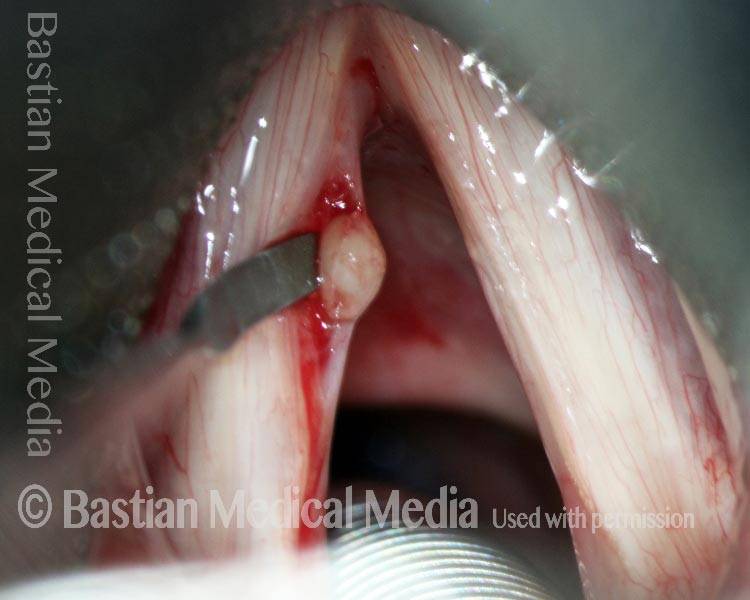
Is it a Cyst or Polyp?
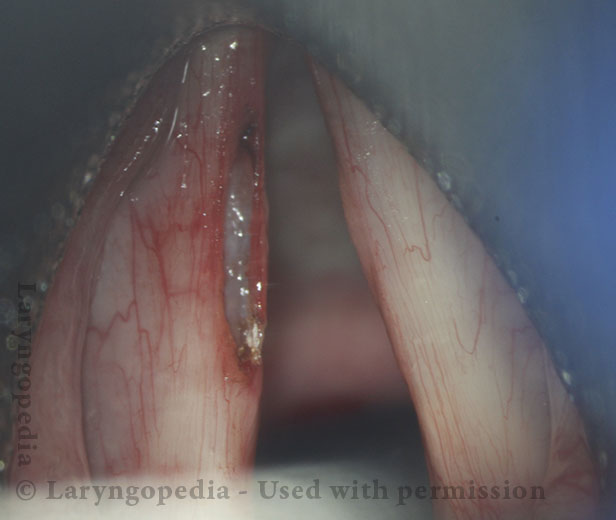
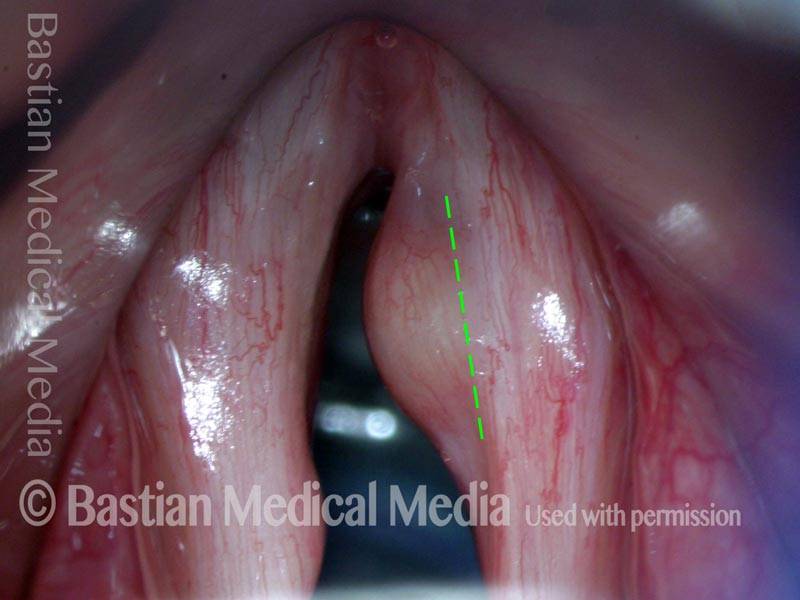
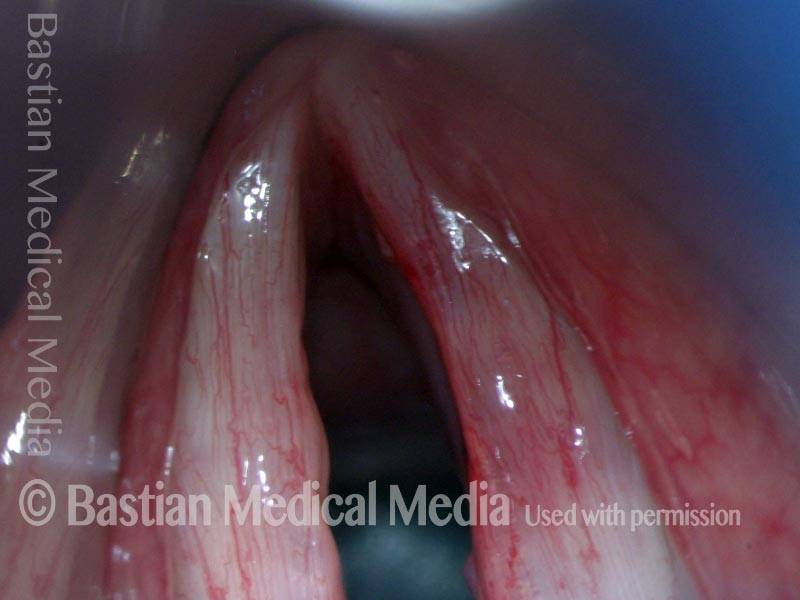
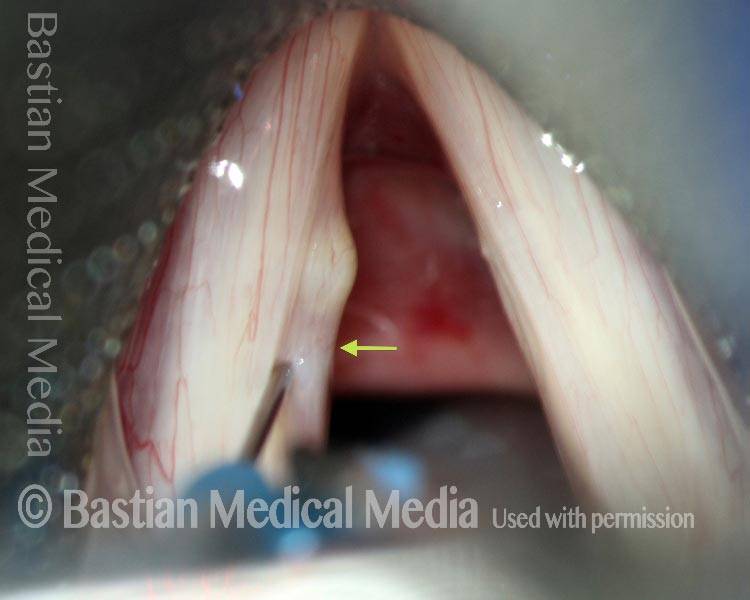
Sometimes a vocal cord lesion resembles a polyp but is not; it is in fact a cyst. Not an epidermoid or saccular type, but a mucus retention cyst. A small mucus gland becomes plugged, and its secretions cannot escape. The result is a cyst filled with mucus.
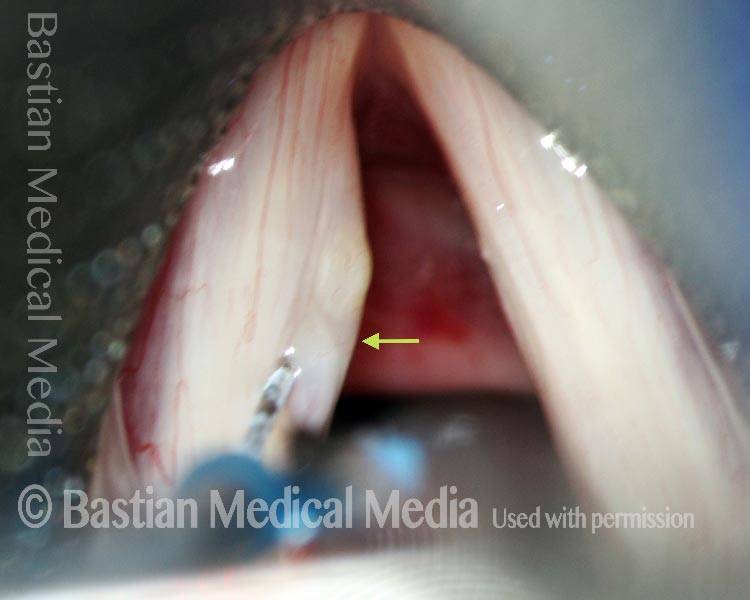
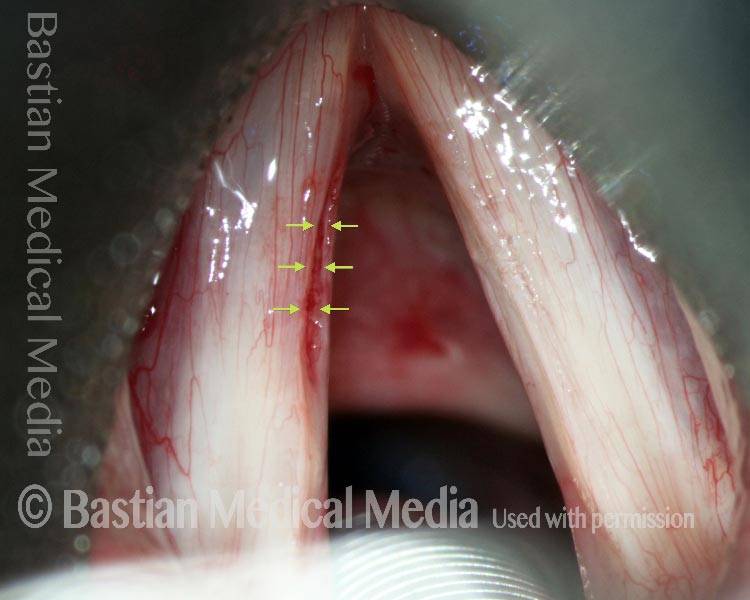
For proper differentiation from a polyp, it is important to know that mucus glands are not found within the primary vibratory mucosa covering the cord. Instead, they populate the area from just under the vocal cord margin, downward into the subglottis and below. Cysts form typically just below the margin, likely due to the gland being affected by adjacent vibration. And by seeing that the swelling is centered just below rather than at the margin, one can distinguish between polyp and mucus retention cyst.
Lesion below the margin (1 of 5)

Vibratory flexibility (2 of 5)
Vocal cord margin above cyst (3 of 5)

Margin of cords (4 of 5)

Cyst occur below match (5 of 5)

![]()
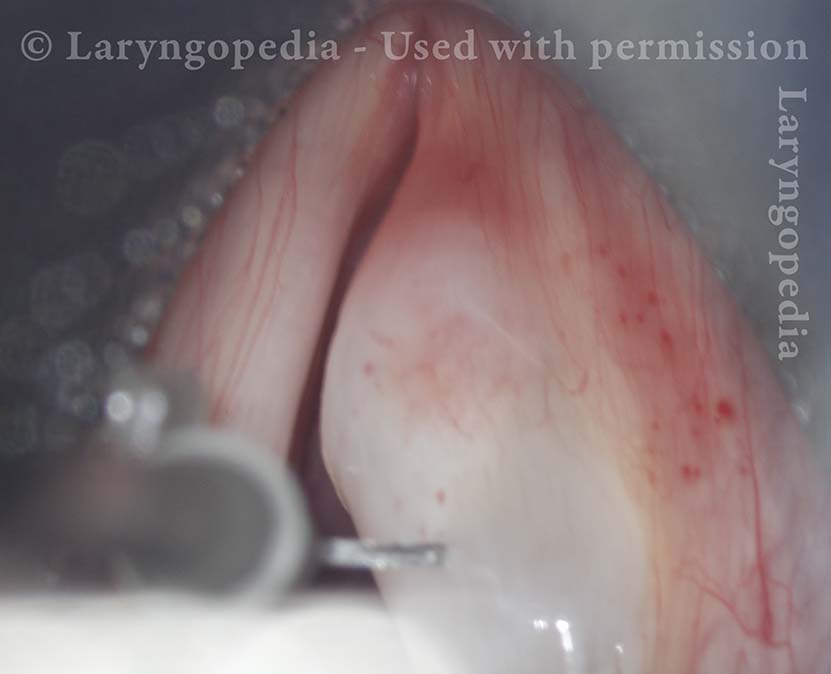
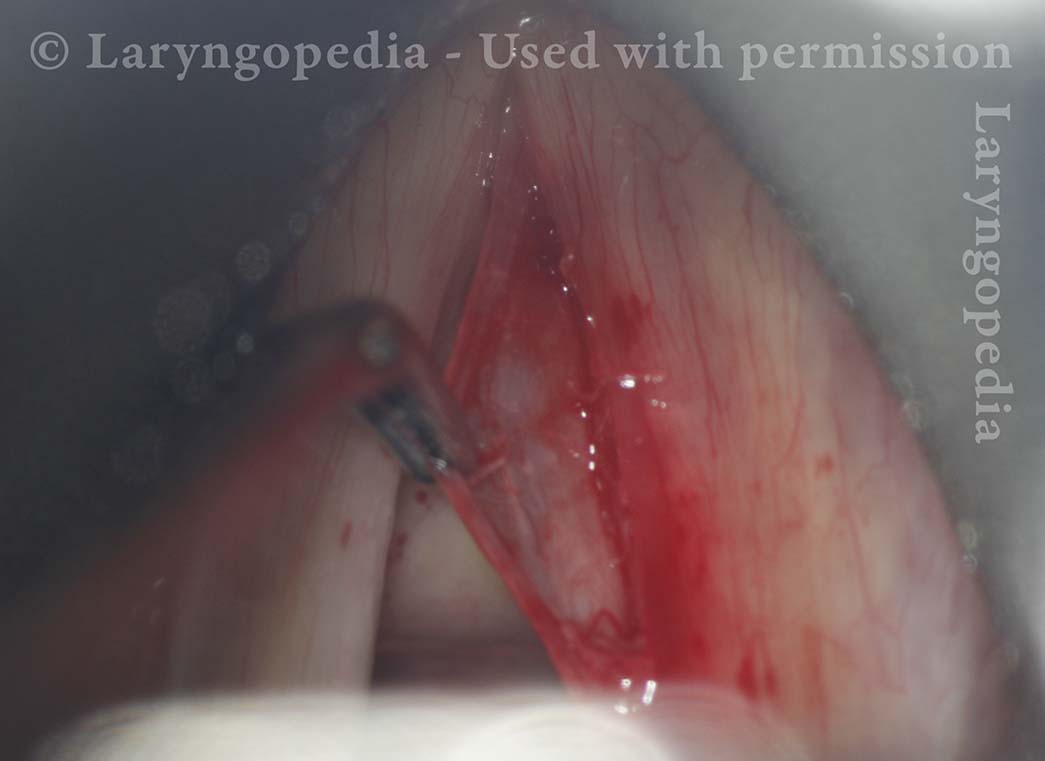
Surgical Removal of a Mucus Retention Cyst
A mucus retention cyst occurs when a small mucus gland becomes plugged and its secretions accumulate, progressively swelling into a cyst. It isn’t known why this happens. There does not seem to be a correlation with vocal overuse, in contrast to vocal nodules, polyps and even epidermoid cysts. Instead, inflammation (viral, or acid reflux-related, for example) seems to be the culprit that plugs the duct of the mucus gland.
In this long series, an older male public speaker presents with severe hoarseness of many months’ duration. Elsewhere, the swelling of his right cord was described as a polyp, rather than a mucus retention cyst. The only solution is surgery(microlaryngoscopy); voice therapy is ineffective for this lesion.
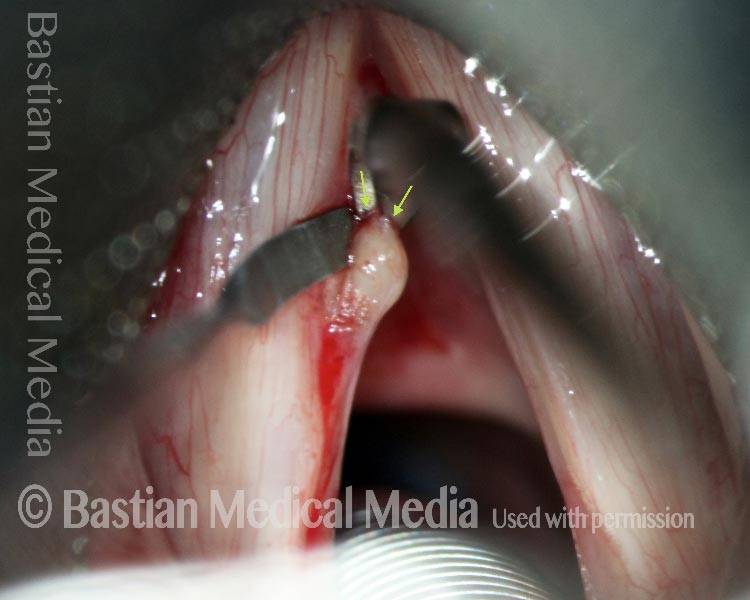
Working with long instruments down a laryngoscope, a very superficial incision is made, the “dragonfly wing” mucosa overlying the cyst is peeled back to expose the cyst. The wall of the cyst itself is also “dragonfly wing” in thickness, making the cyst subject to rupture during removal. Usually if rupture occurs, it is nearing the completion of removal, when most of the dissection has been accomplished and making it possible to remove the entire cyst. In this case, the cyst is delivered intact. Vocal recovery is virtually to normal.
Right vocal cord cyst (1 of 20)
Cyst under strobe illumination (2 of 20)

Cyst margin projection (3 of 20)
Operating view of cyst (4 of 20)

Injecting Lidocaine (5 of 20)
Preparing for Microlaryngoscopy (6 of 20)

Incision of mucosa (7 of 20)

Incision in process (8 of 20)

Dissection of cyst (9 of 20)

Dissection near complete (10 of 20)

Un-ruptured cyst removal! (11 of 20)

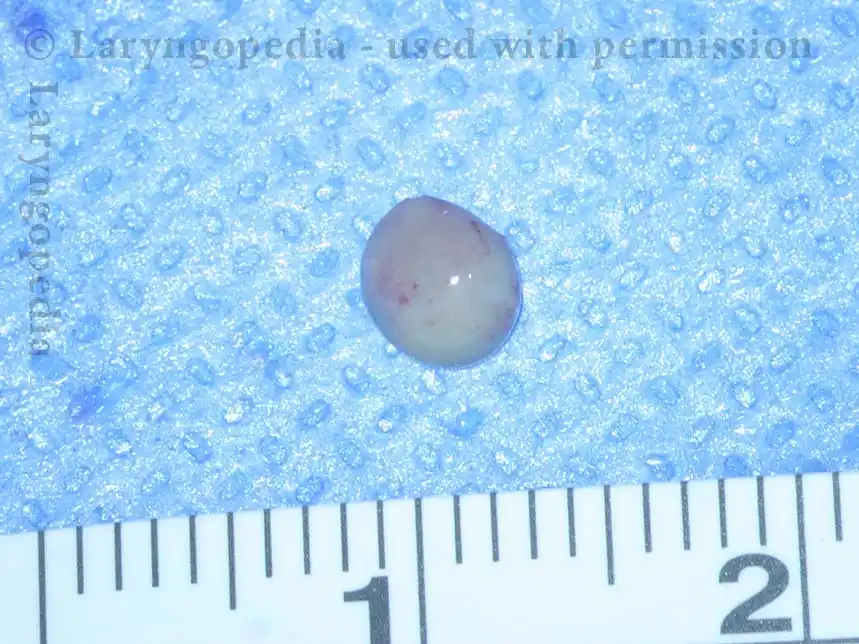
7mm intact cyst (12 of 20)

Mucosa flap (13 of 20)
Is the voice affected? (14 of 20)

Voice is much improved! (15 of 20)
Vocal cord vibrates (16 of 20)

Slight bowing (17 of 20)

Equal vibratory blur (18 of 20)

Reasonable closure (19 of 20)

Voice returns to baseline (20 of 20)
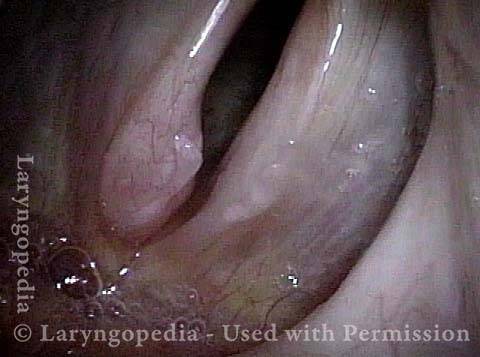
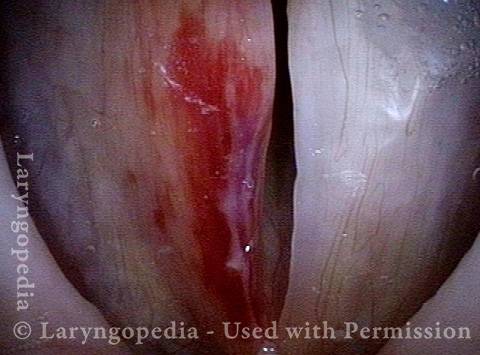
Excision of a Mucus Retention Cyst that Decompresses during Dissection
This man has had slight hoarseness for many years, possibly related to his self-described highly talkative and loud-spoken nature. His voice took a significant turn for the worse soon after a bout of mild laryngitis, and had remained extremely hoarse for many months.
An ENT doctor diagnosed a polyp of his left vocal cord. Instead, this represents a mucus retention cyst. Removal provided dramatic return of clear speaking voice. Seen below is preop, intra-operative sequence, and then the result at 3 months after surgery.
Mucus retention cyst (1 of 17)
Closer look (2 of 17)

Cyst under narrow band light (3 of 17)
Cyst interferes with phonation (4 of 17)

Surgical view (5 of 17)

After infiltration (6 of 17)
Lifting the mucosa (7 of 17)

Dissecting cyst from deep attachments (8 of 17)

Cyst has ruptured and emptied (9 of 17)

Dissection of empty sac (10 of 17)

Flaps retract (11 of 17)
Voice is virtually normal at 3 months (12 of 17)

Evidence of vibration, standard light (13 of 17)
Open phase at E3 (14 of 17)
Closed phase at E3 (15 of 17)
Open phase at A4 (16 of 17)

Closed phase at A4 (17 of 17)

Removal of Mucus Retention Cyst, Still Intact
Mucus retention cyst (1 of 8)

Injection in Reinke’s space (2 of 8)

Incision begins (3 of 8)

Removal of cyst (4 of 8)

Removal nearly complete (5 of 8)

Cyst is removed (6 of 8)

Post-op (7 of 8)

Open Phase (8 of 8)

Removal of Mucus Retention Cyst
Mucus retention cyst (1 of 7)
Xylocaine prepares for removal (2 of 7)

Removal of Cyst (3 of 7)

Removal of cyst (4 of 7)

Removal of Cyst (5 of 7)

Voice immediately improves (6 of 7)
4mm Cyst (7 of 7)
Example 2
Injecting Xylocaine (1 of 5)
{kind=link}
Hydrodissection effect (2 of 5)
{kind=link}
Removal of cyst (3 of 5)
{kind=link}
Removal of cyst (4 of 5)
Cyst is gone! (5 of 5)
{kind=link}
Mucus-Retention Cyst—not Polyp—Before and After Removal
Mucus-retention cyst (1 of 11)

The cyst is centered below cord margin (2 of 11)

Initial (Inverted) Operative View (3 of 11)

Initial incision (4 of 11)

Dissection continues (5 of 11)

Dissection continues (6 of 11)

Dissection complete (7 of 11)

Final operative result (8 of 11)

One week post-op (9 of 11)

Margins now match (10 of 11)
Retained vibratory flexibility (11 of 11)