An epidermoid cyst has a wall lined by squamous epithelium and therefore accumulates keratin. It may also be called an epidermal cyst, an epidermal inclusion cyst, or a keratin cyst. In the larynx, an epidermoid cyst typically occurs in one or both of the vocal cords. These epidermoid cysts are usually white in color, and are often seen in vocal overdoers.
What causes an epidermoid cyst
Epithelium is the tissue that makes up the outermost layer of skin, and is also the top layer of tissue that lines the interior of the body. Epithelial tissue produces a protein called keratin. If any of this epithelial tissue somehow becomes buried in the subepithelial layer, then the keratin it produces may become trapped and accumulate within the subepithelial layer, leading to an epidermoid cyst.
In the vocal cords, an epidermoid cyst may sometimes occur simply due to a congenital defect: keratin-producing epithelial cells were buried in the subepithelial layer from birth. Some believe this is the explanation even when the initial manifestation of hoarseness doesn’t occur until adulthood.
In these cases, however, it is more logical to see vocal overuse as the key factor, perhaps because epithelial cells can get buried in the subepithelial layer as the vocal cord mucosa heals in response to a vocal overuse injury.
Vocal symptoms of an epidermoid cyst
An epidermoid cyst may cause vocal limitations similar to that of vocal nodules. However, patients with epidermoid cysts are more likely to experience diplophonia in the upper voice, and as the voice ascends in pitch, its impairment may manifest itself much more abruptly and severely at a particular frequency, as compared to most patients with nodules, who experience a more gradual transition to increasing impairment as they ascend in pitch.
Appearance of an epidermoid cyst
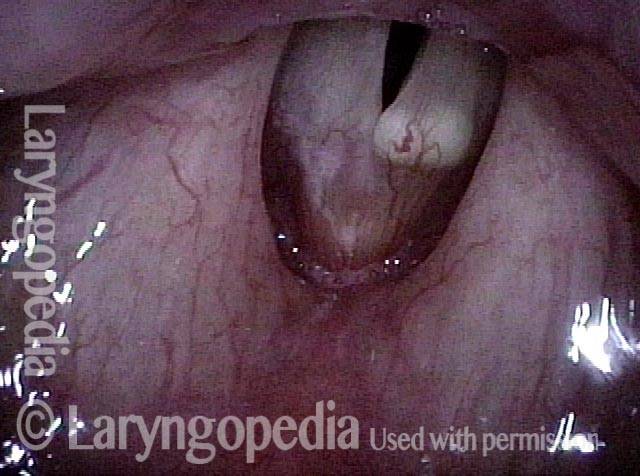
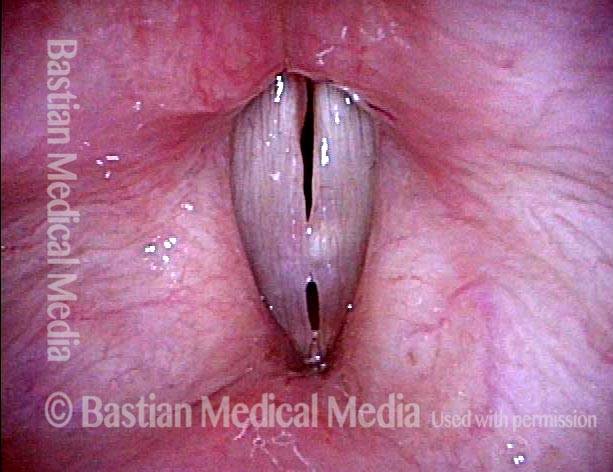
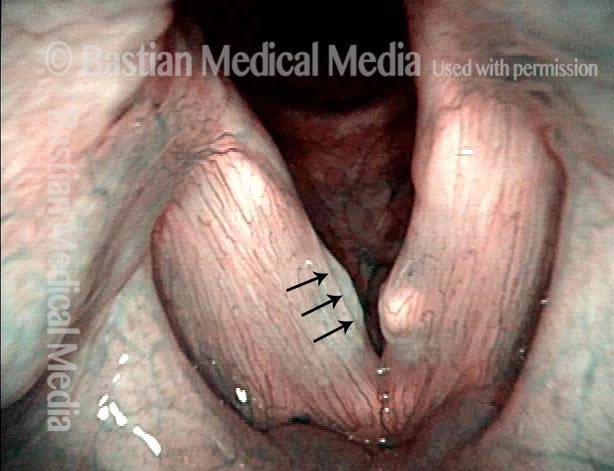
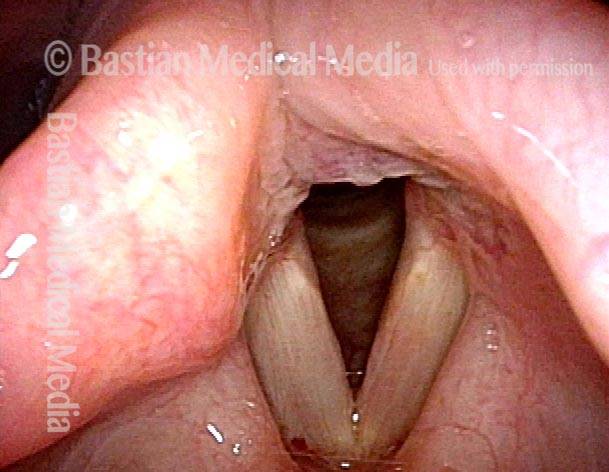
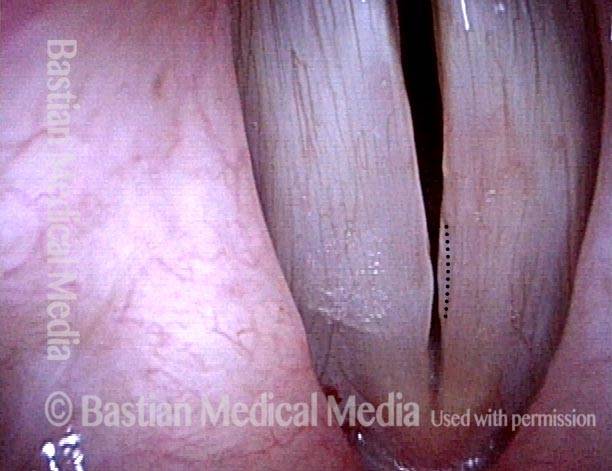
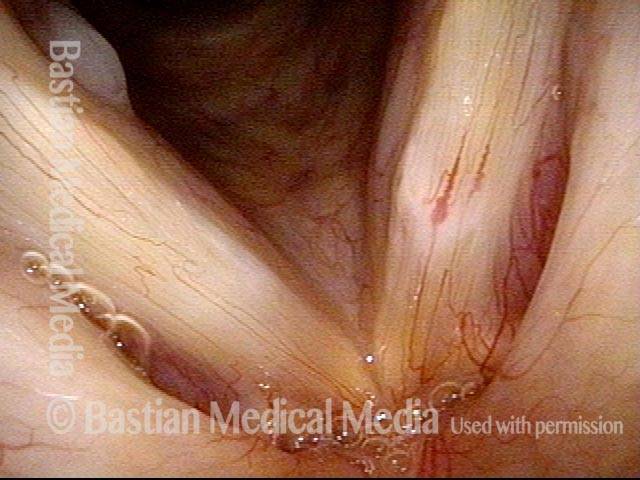
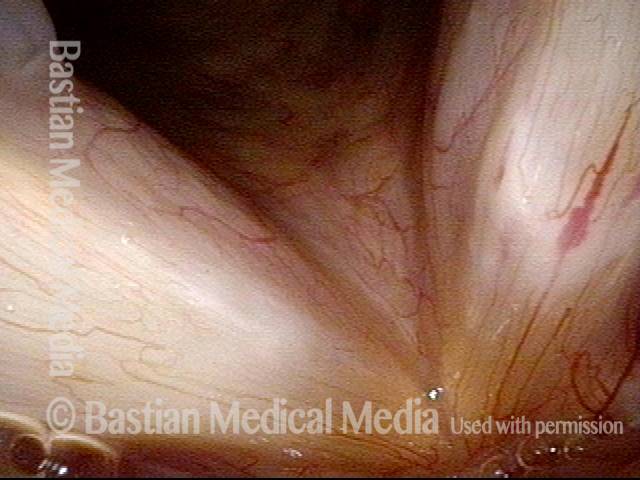
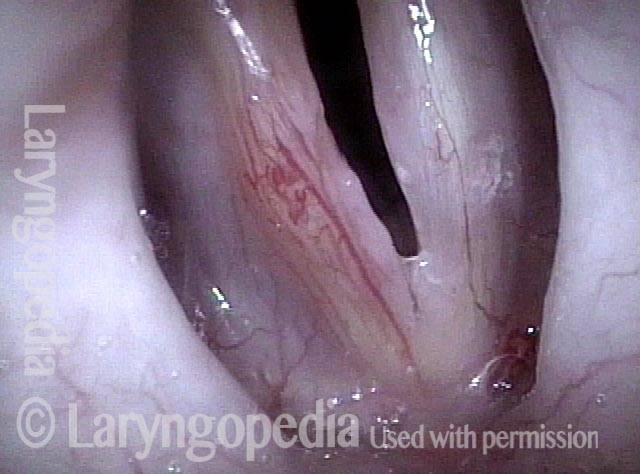
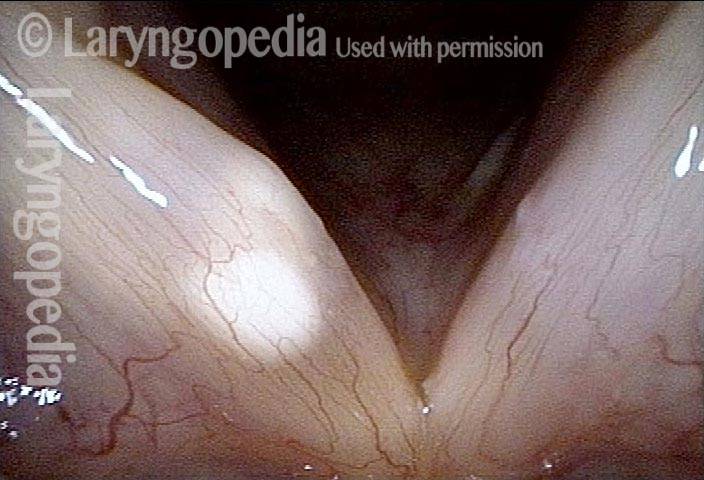
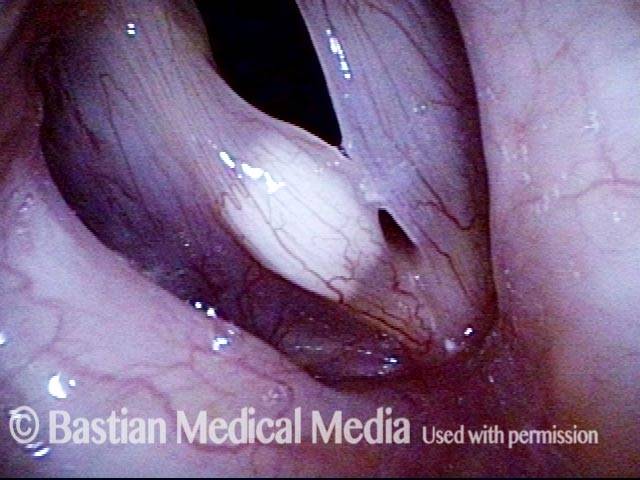
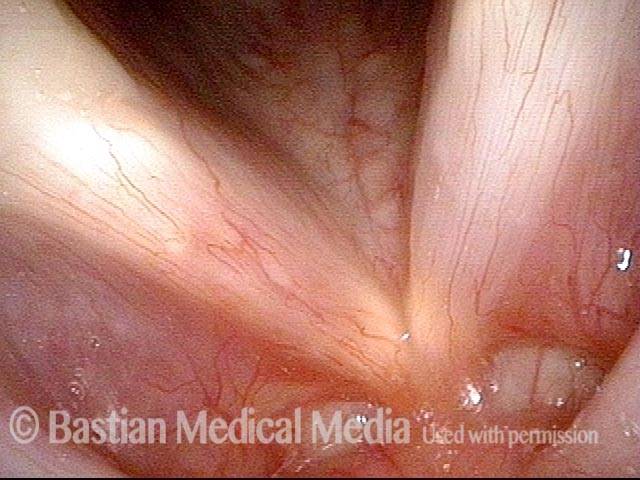
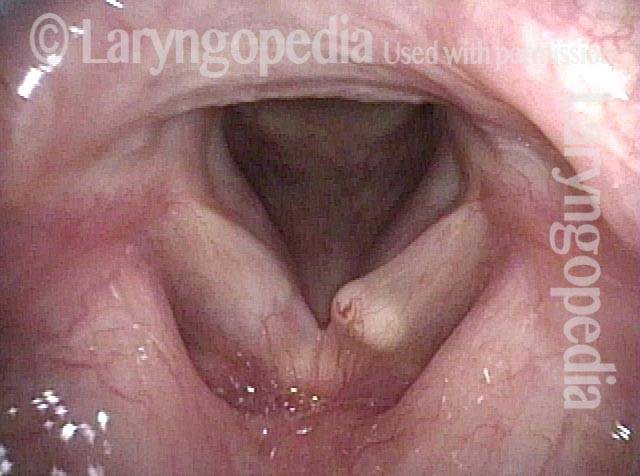
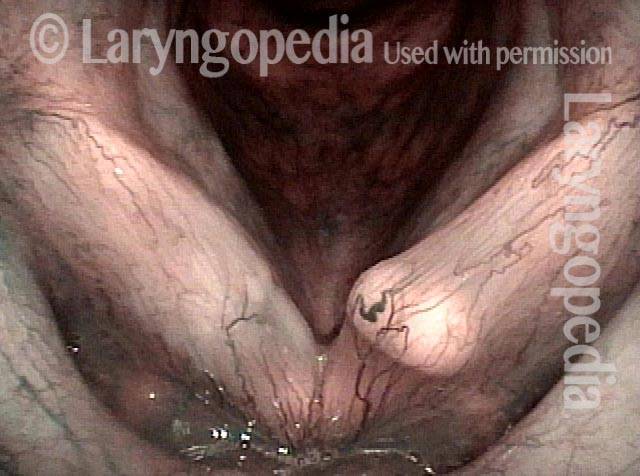
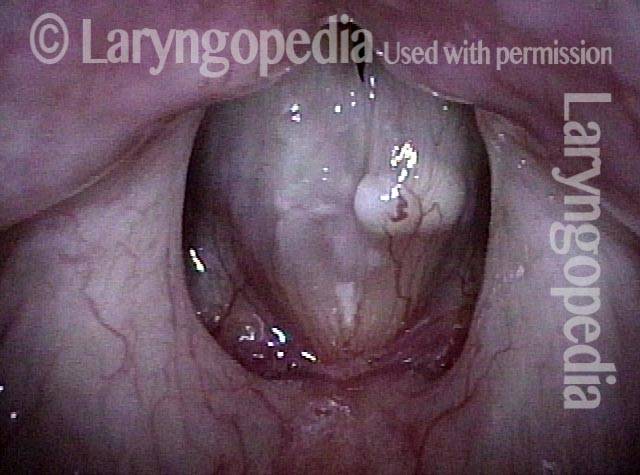
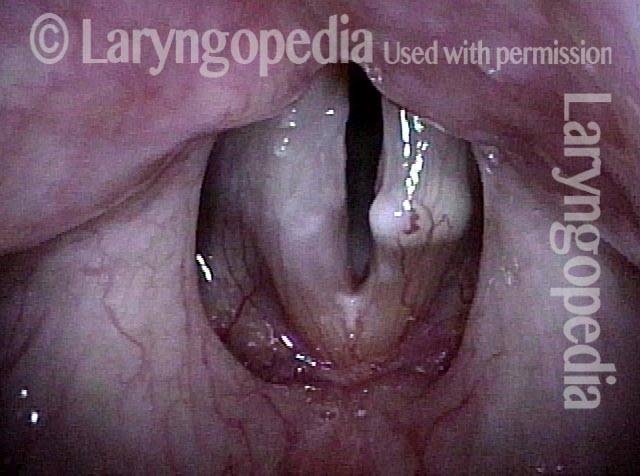
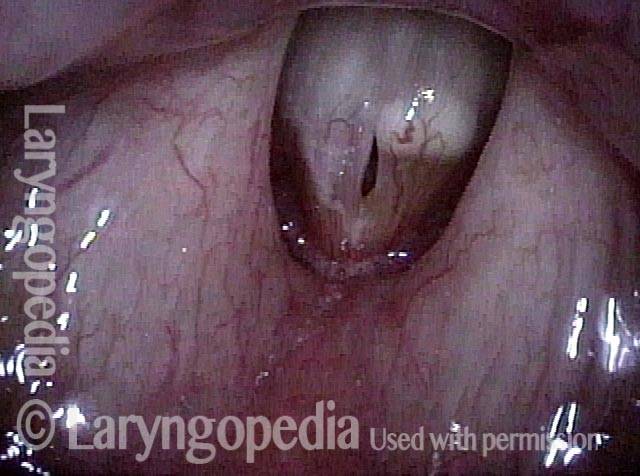
An epidermoid cyst of the vocal cord is generally most visible on the cord’s upper surface, and is whitish in color. In comparison with mucus retention cysts, epidermoid cysts project less from the cord, and when smaller, they can be quite subtle and easy to miss. Sometimes an epidermoid cyst will have spontaneously ruptured but still retain some of the accumulated keratin (an open cyst); in this case, the cyst’s outline may be more subtle, and usually assumes an oval shape with the long axis oriented anteriorly and posteriorly. An open cyst may also produce a mottled appearance.
Treatment for an epidermoid cyst
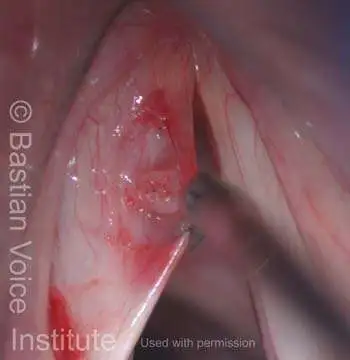
Speech therapy is important for patients who are vocal overdoers, to help prevent the future occurrence of this or other vocal overuse-related lesions and injuries, but it will not resolve the cyst. Surgery can be performed to remove the cyst. This requires an incision and then dissection of the entire intact sphere of the cyst. The surgery is technically far more difficult than is removal of nodules or polyps, and is more likely to cause chronic stiffness of the disturbed mucosa. Still, results can be very good, especially if the overlying mucosa is relatively thick.
Cyst Removal
Cyst removal (1 of 7)
Cyst removal (2 of 7)
Cyst removal (3 of 7)

Cyst removal (4 of 7)
Cyst removal (5 of 7)

Cyst removal (6 of 7)

Cyst removal (7 of 7)

Epidermoid cyst
Epidermoid cyst (1 of 2)

Epidermoid cyst (2 of 2)

Example 2
Teacher with longstanding hoarseness (1 of 4)
Epidermoid cyst and polypoid nodule seen (2 of 4)
Six days post-surgery, voice improved (3 of 4)
Expected early postsurgical swelling (4 of 4)
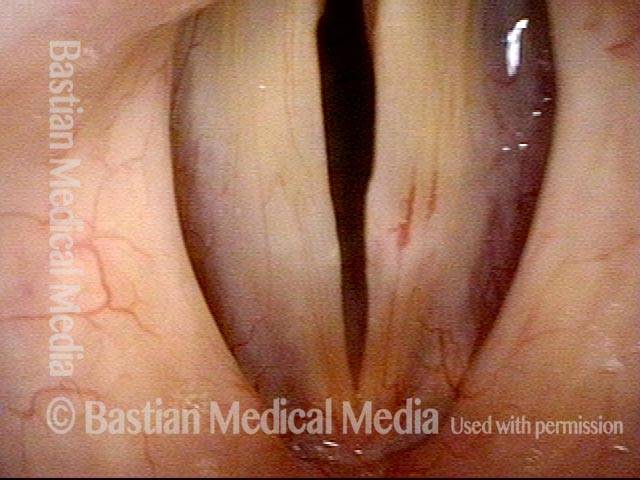
Possible Open Epidermoid Cyst
Capillary ectasia and white submucosal abnormality (1 of 3)
Prephonatory view, mtd (2 of 3)
Open cyst (3 of 3)
Open Cyst and Sulcus in Same Patient
Hoarse voice (1 of 4)

Cyst + sulcus (2 of 4)

Closed phase (3 of 4)

Open phase (4 of 4)
Epidermoid Cyst, Before and After Removal
Epidermoid cyst (1 of 4)
Phonatory view (2 of 4)

Post microsurgery (3 of 4)

4 months post surgery (4 of 4)

Example 2
Epidermoid cyst (1 of 3)

Epidermoid cyst (2 of 3)
Epidermoid cyst, removed (3 of 3)
Bilobed Epidermoid Cyst and Shimmying Vibration
Distant view (1 of 6)
Closer view, narrow band light (2 of 6)
Closure under strobe light (3 of 6)
Open phase (4 of 6)
An octave above (5 of 6)
“Shimmying” vocal cord (6 of 6)