Vocal Nodules
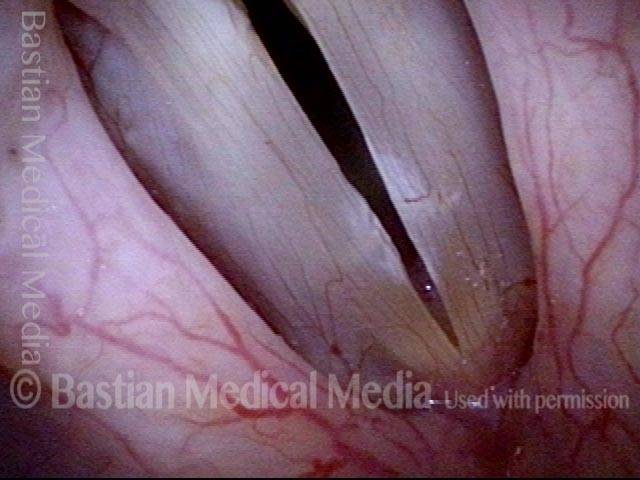
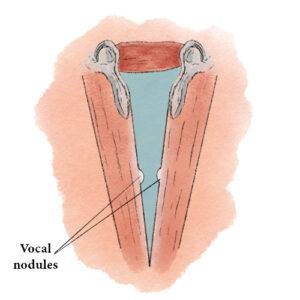
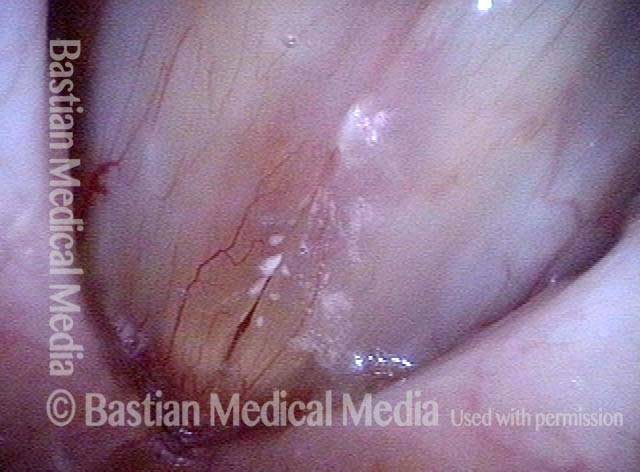
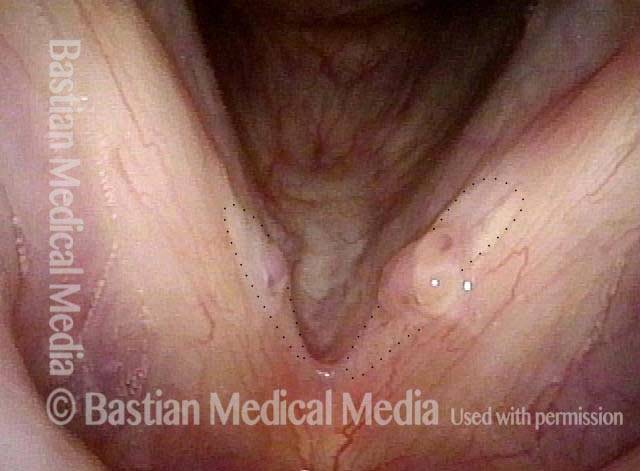
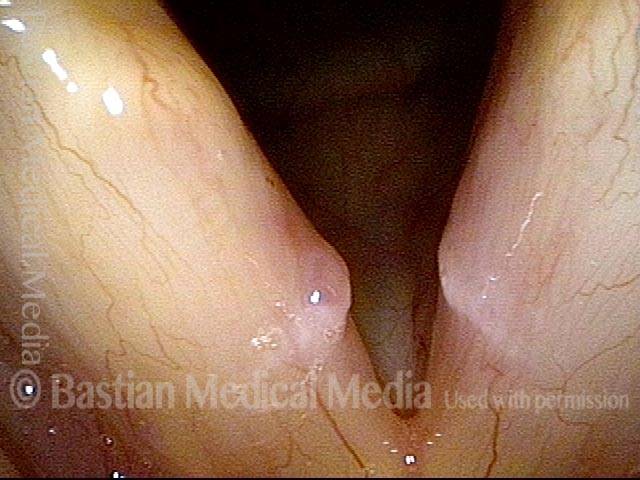
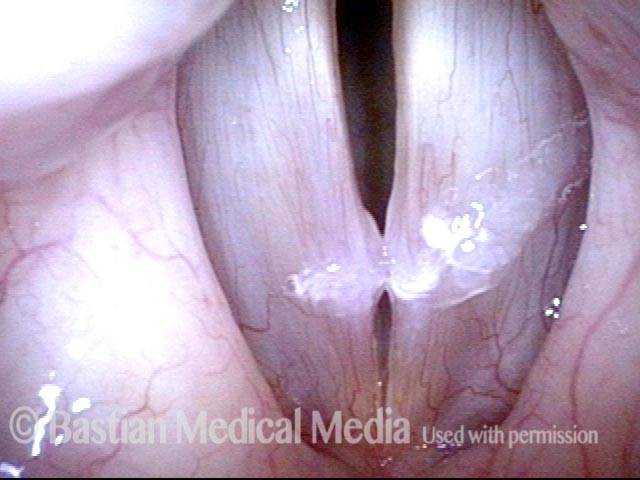
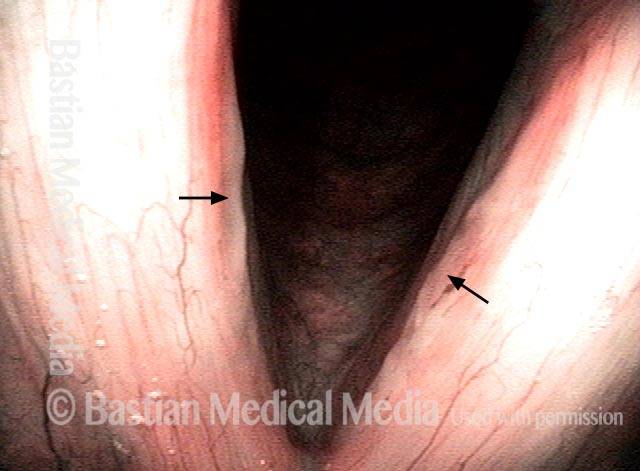
Small chronic swellings that appear in the junction of the middle and anterior thirds of the vocal cord. These swellings, or nodules (nodes), are vibratory injuries caused by vocal overuse.
Symptoms
The most obvious symptom of medium-to-large nodules tends to be hoarseness. The top 5 symptoms for nodules of any size may include:
- Difficulty with high, soft singing;
- Day-to-day variability of vocal capability and clarity;
- A sense of increased effort to produce voice, especially for singing;
- Reduced endurance, so that the voice becomes husky or “tired” after less voice use than formerly;
- Phonatory onset delays, when there is a slight hiss of air before the voice “pops in.”
Etiology
When you overuse your voice, your body tries to cushion the vocal cords by pooling together edema (fluid) beneath the vocal cord mucosa (the surface layer of the cords); this pooled edema is like a small, low-profile blister on your finger. If after a few days you stop overusing your voice, the edema disperses readily, within a few days, and this “blister” on the vocal cords vanishes.
If, however, the amount or manner of voice use remains excessive for many weeks or months, then more chronic swelling materials (no longer just edema fluid) are laid down by the body, and the vocal cords develop true nodules.
Why Nodes Affect the Voice
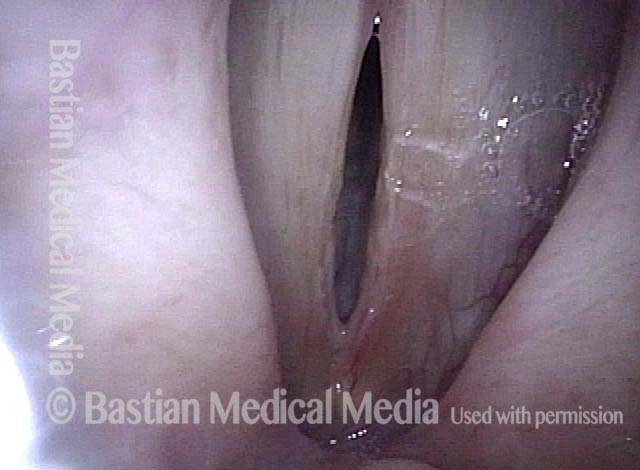
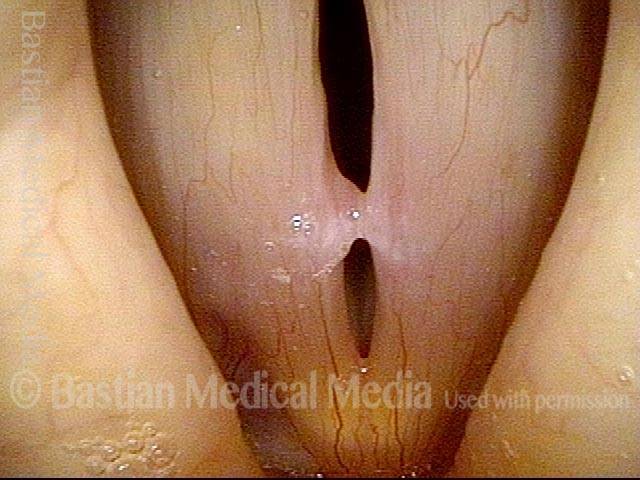
In either case (acute swellings or chronic nodules), this injury to the mucosa can impair the voice in two ways: it reduces the vibratory flexibility of the mucosa, and it interferes with the accurate match of the cords when they come together to produce voice. This impairment causes the voice to be hoarse or, more subtly, to suffer from onset delays, difficulty with high notes, and other similar problems.
Treatment
Nodules will often dissipate, with the help of rest and perhaps speech/voice therapy, over a period of weeks or months. Sometimes, the swellings are so stubborn that microsurgery is required.
![]()
![]()
How Is the Voice after Treatment?
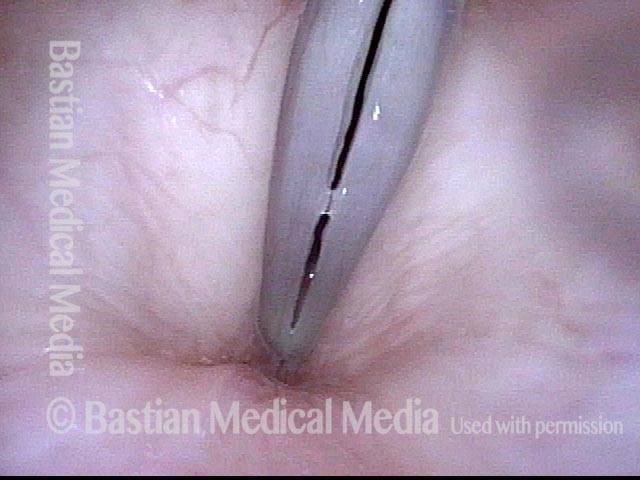
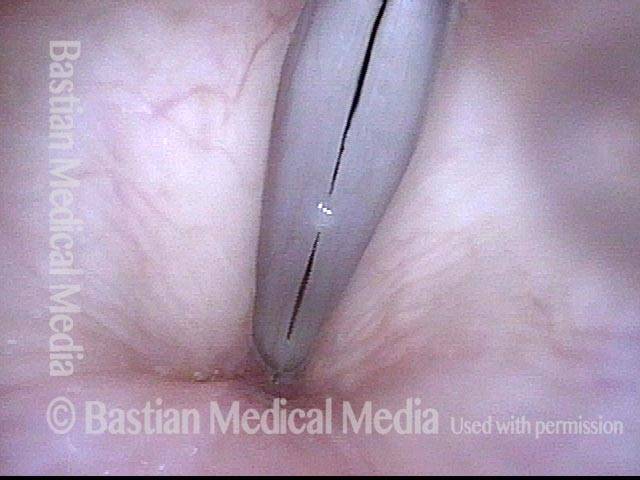
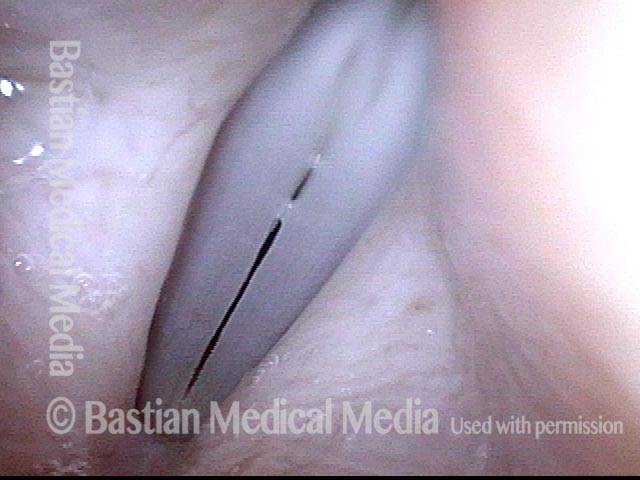
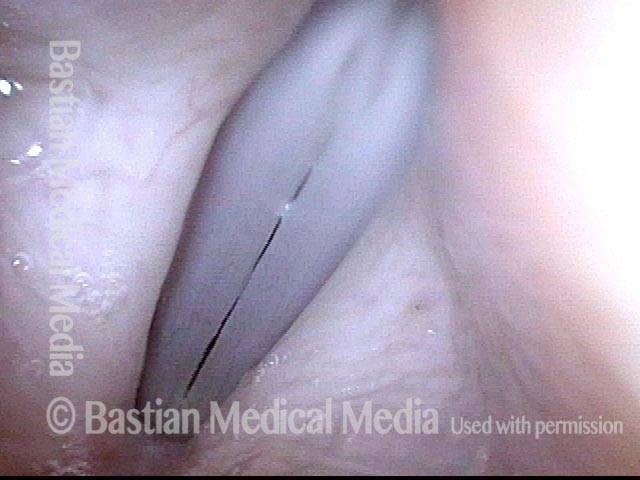
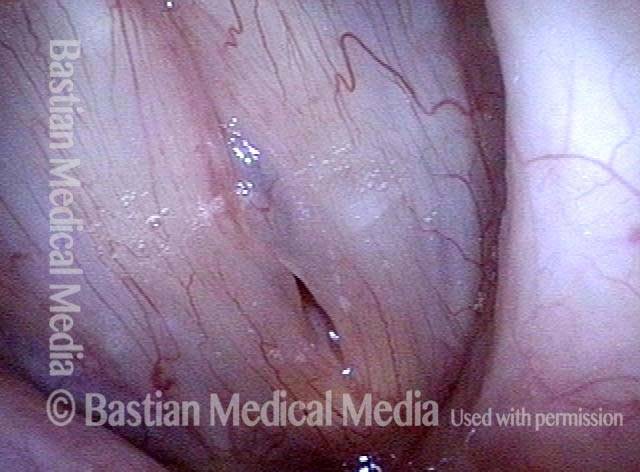
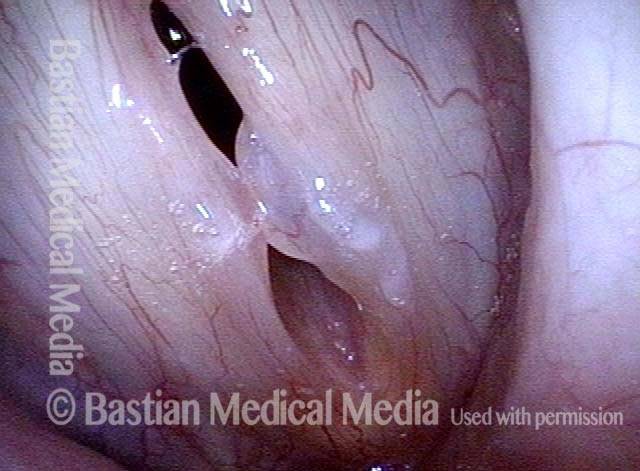
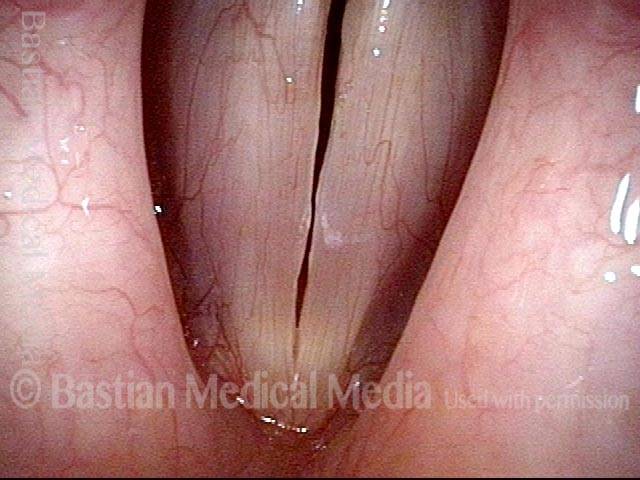
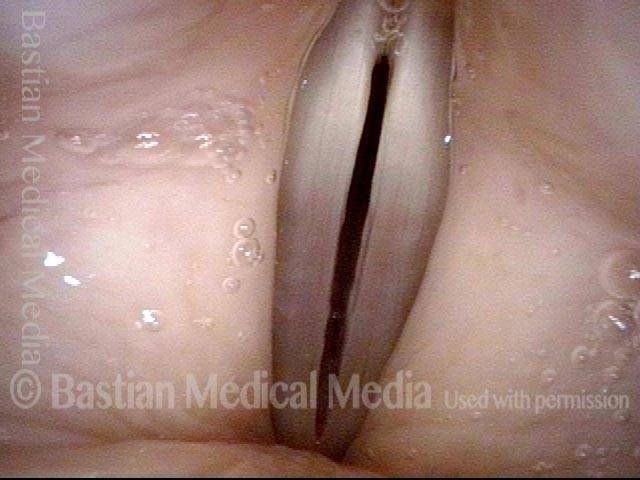
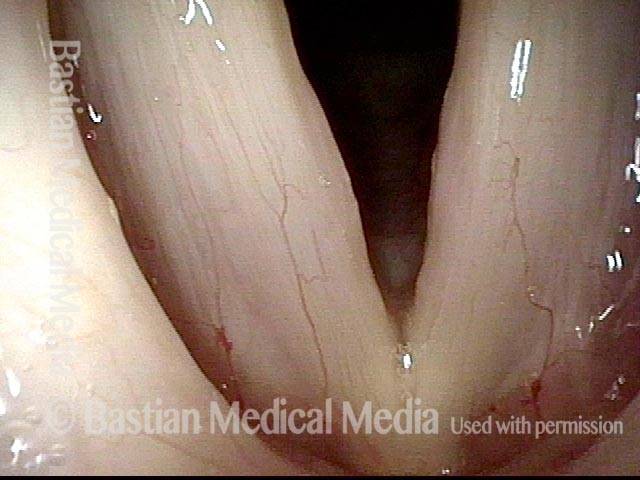
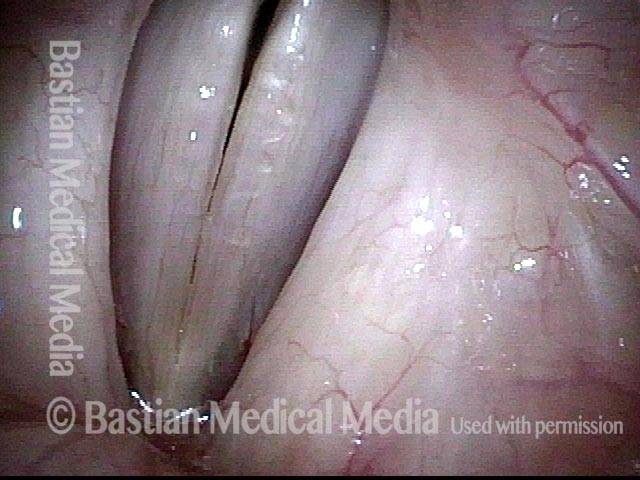
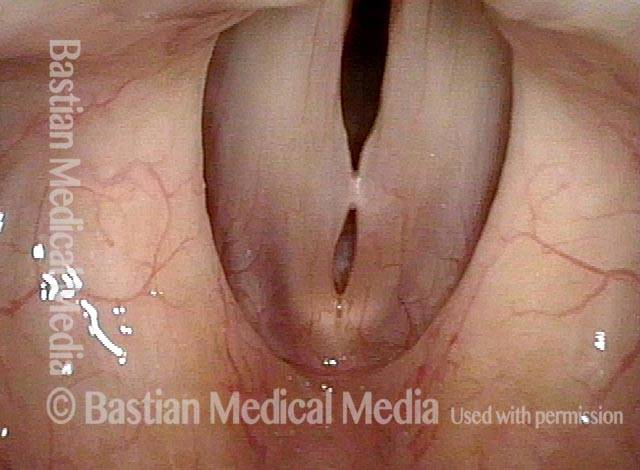
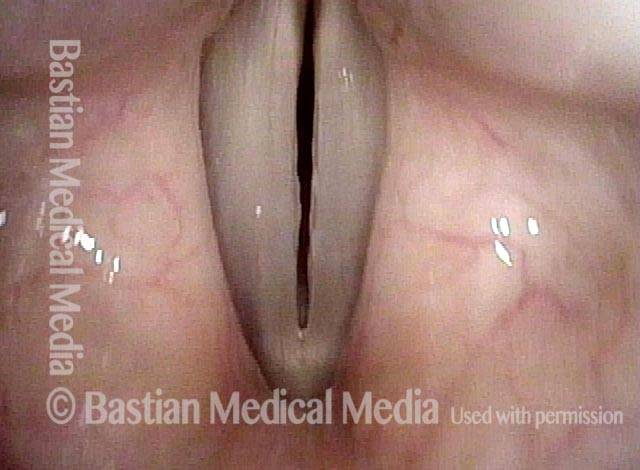
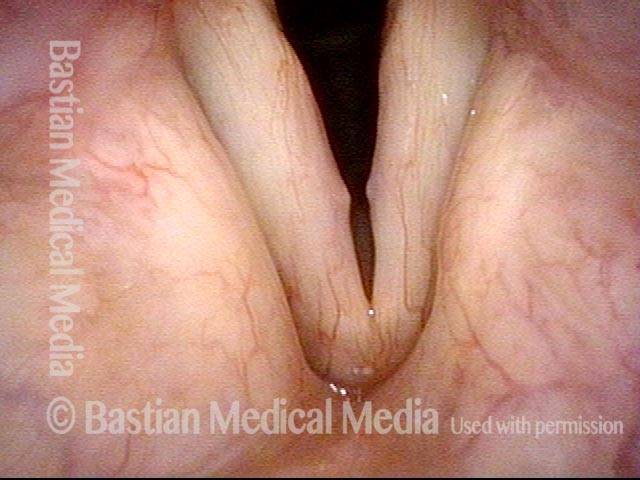
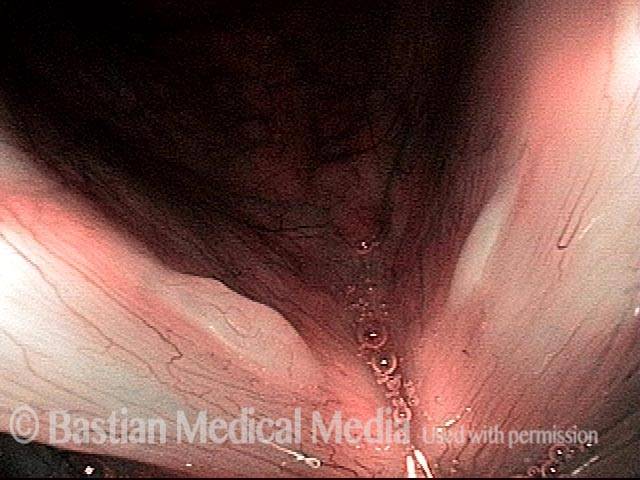
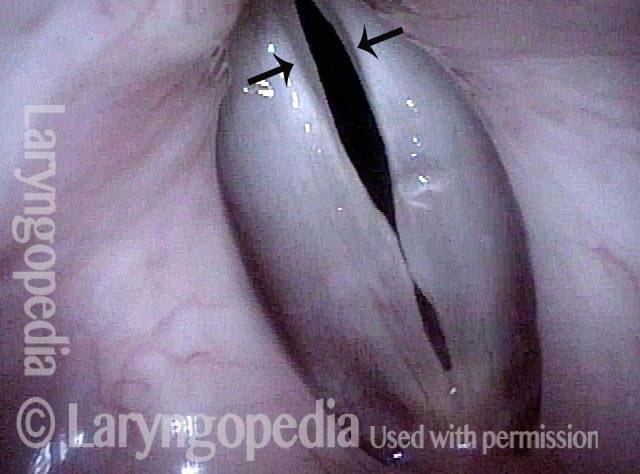
Vocal nodules’ effect on the voice, BEFORE surgical removal (see this patient’s photos just below):
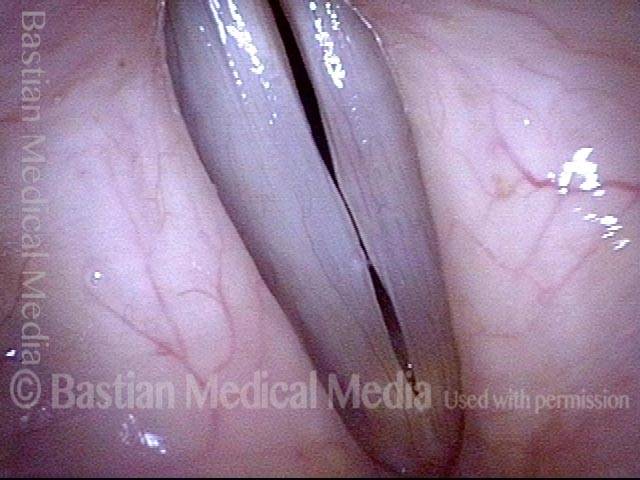
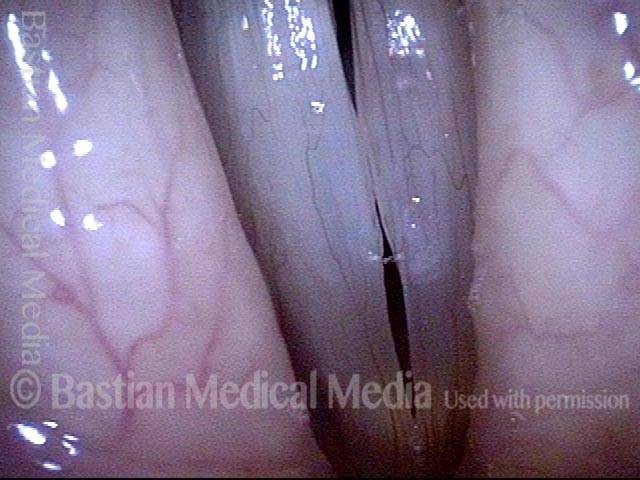
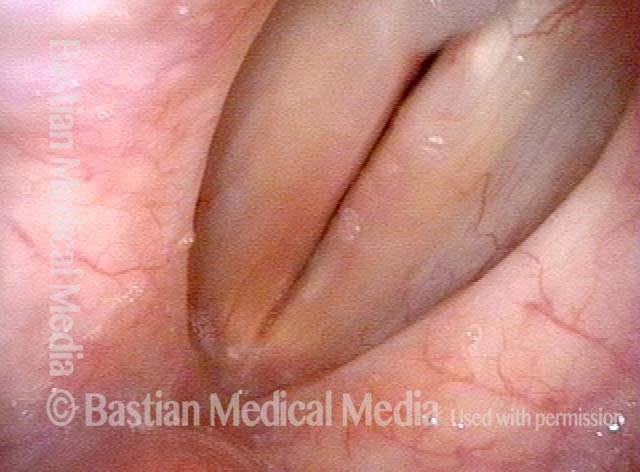
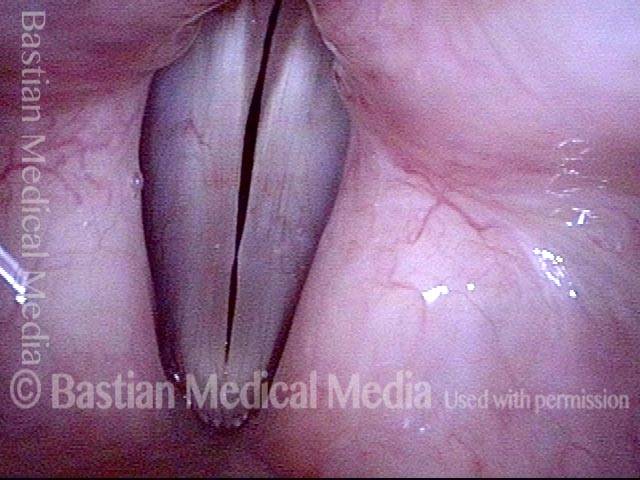
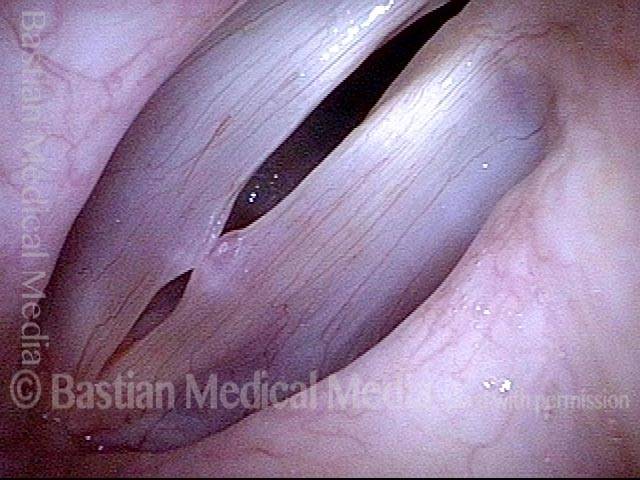
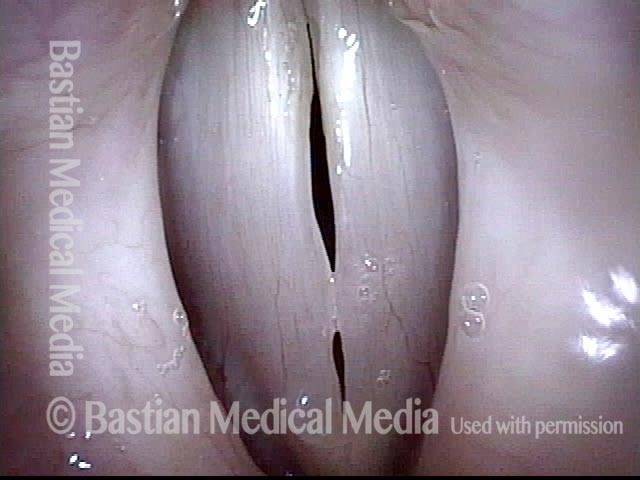
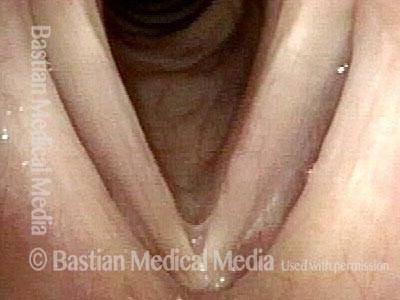
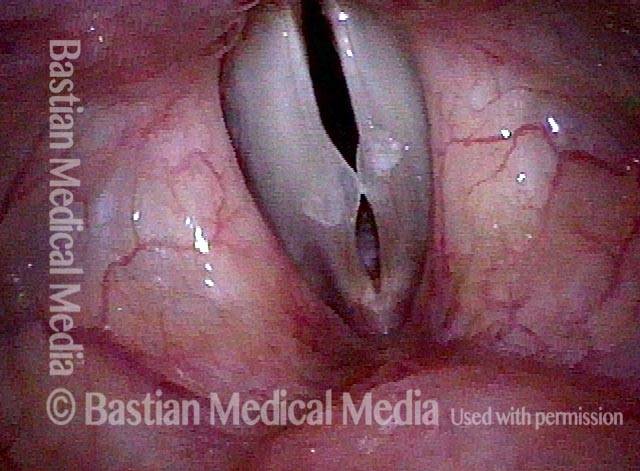
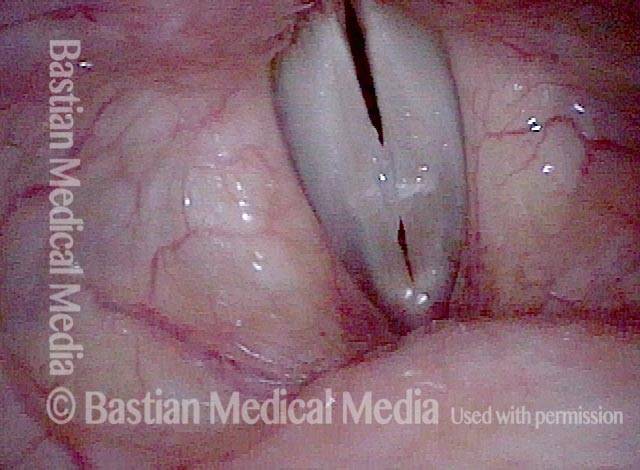
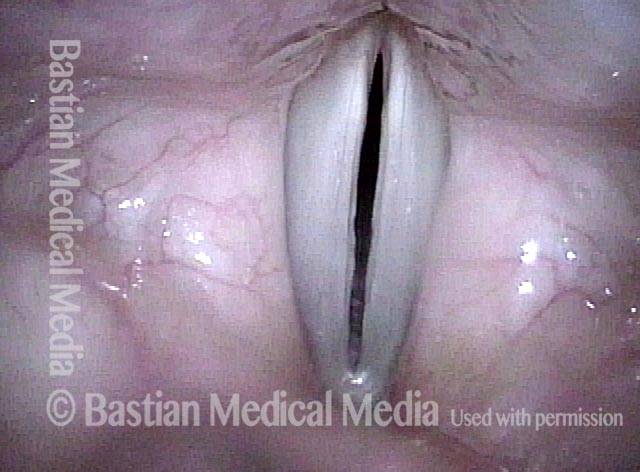
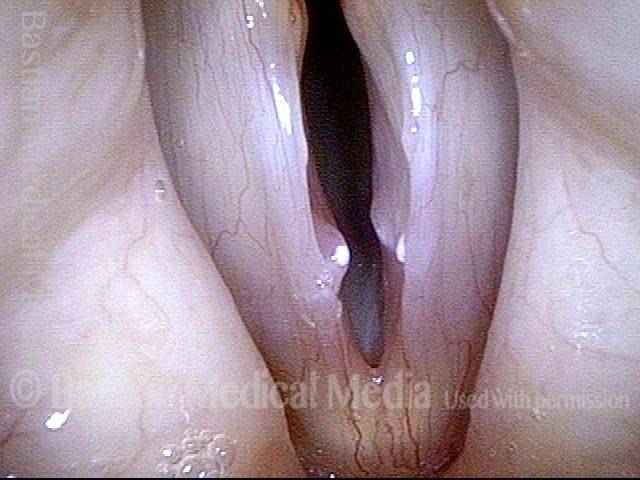
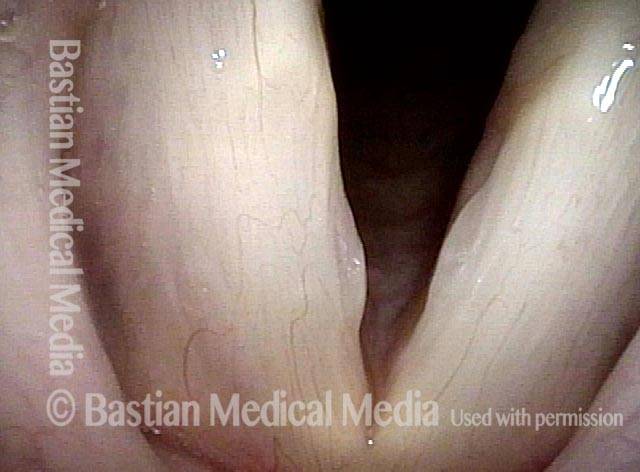
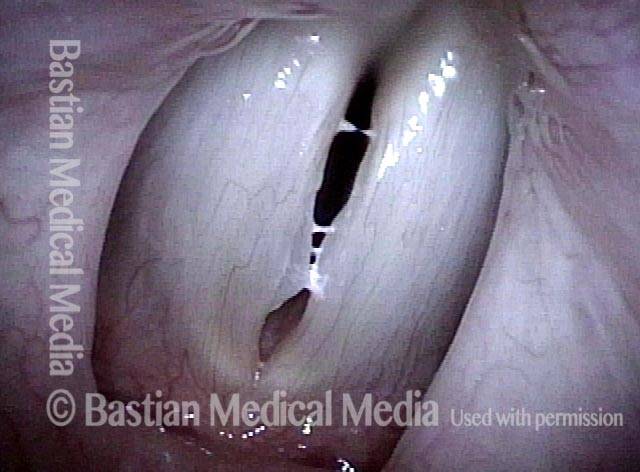
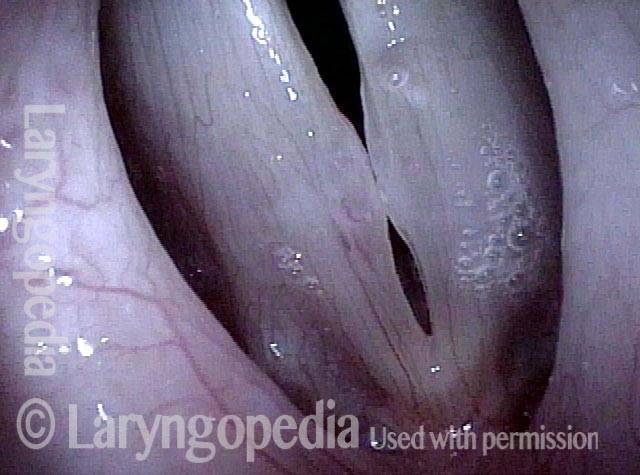
Same patient, seven weeks AFTER surgical removal of the vocal nodules:
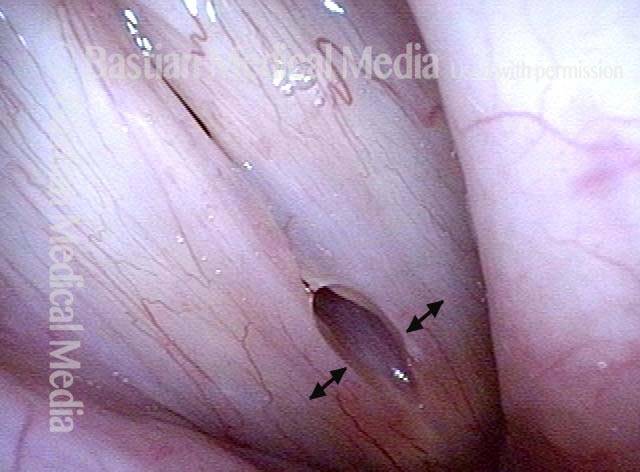
Vocal Nodules, Before and After Surgery
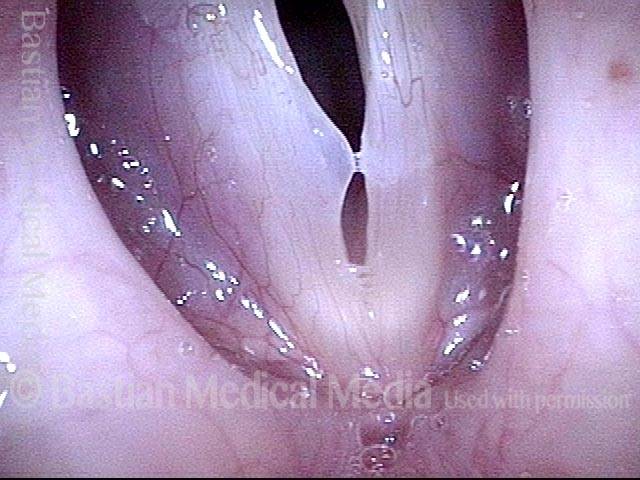
Vocal nodules (1 of 6)

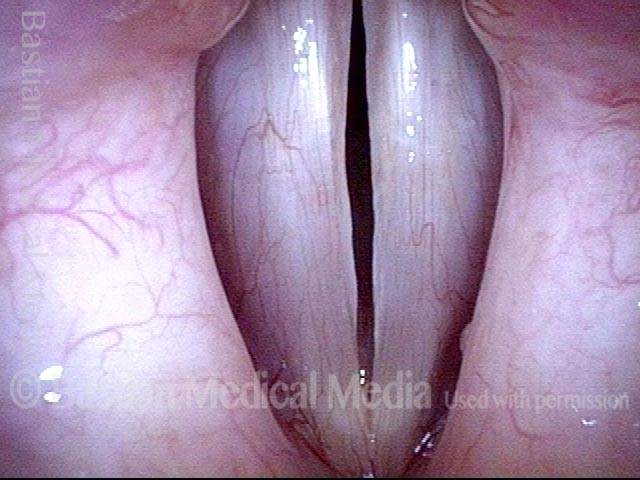
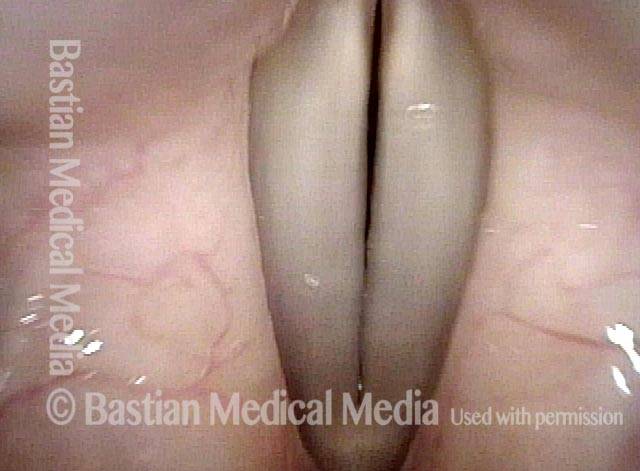
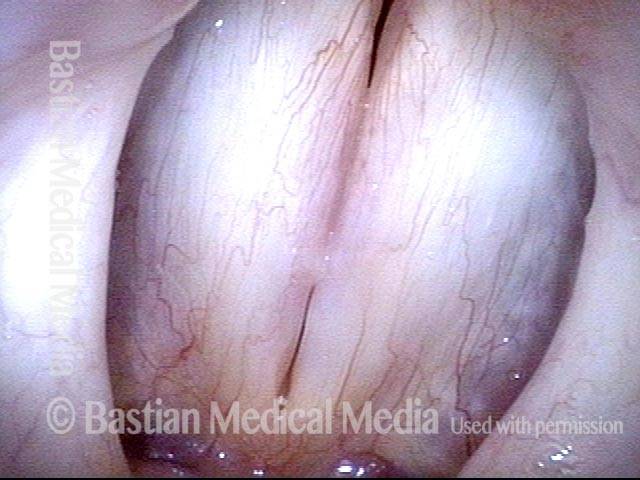
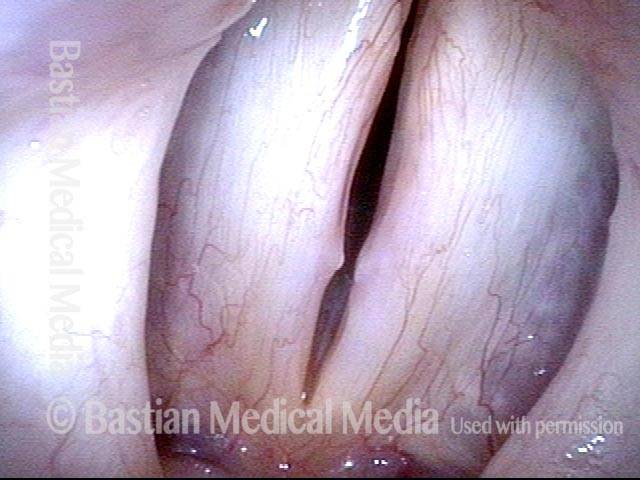
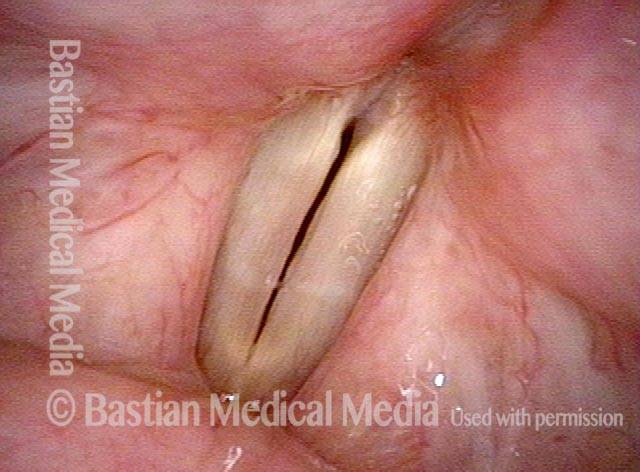
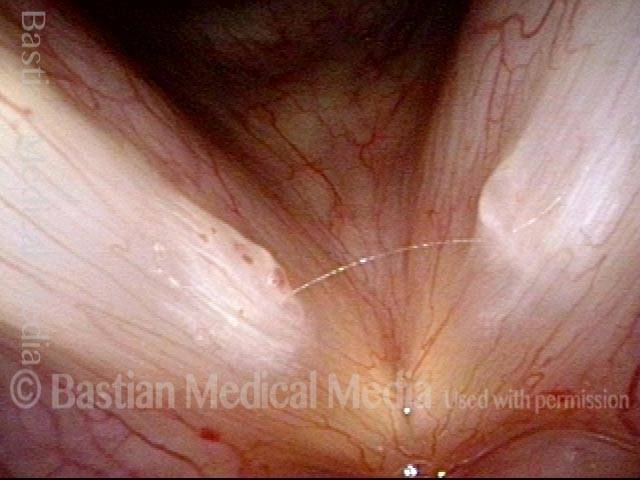
Breathy voice (2 of 6)

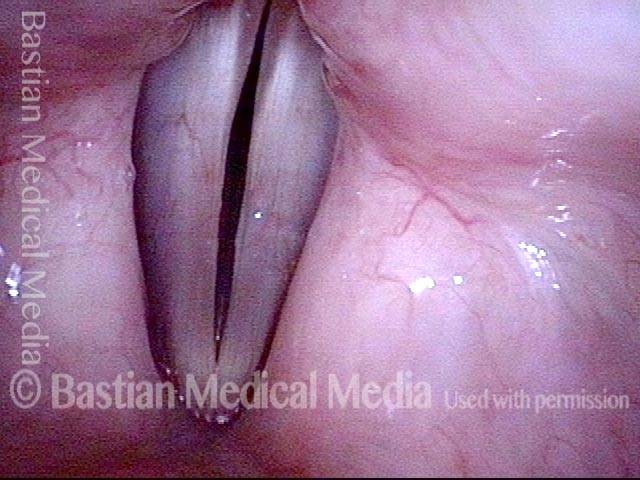
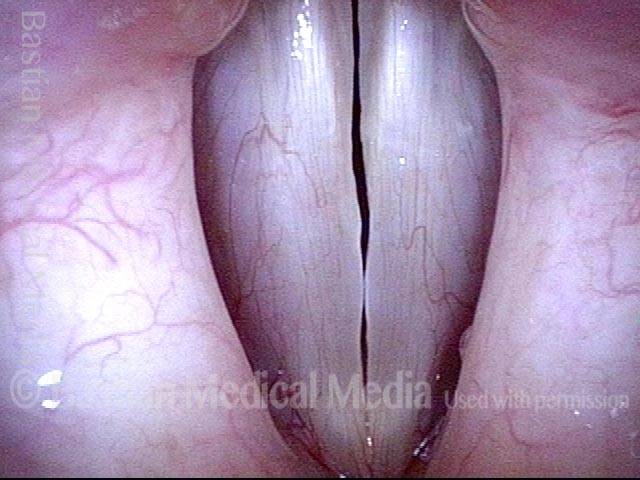
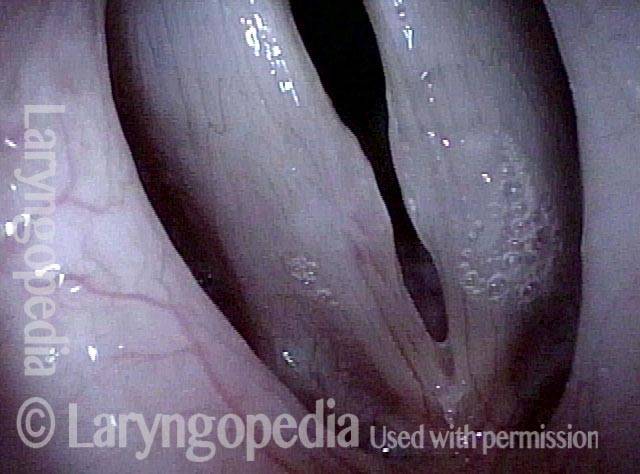
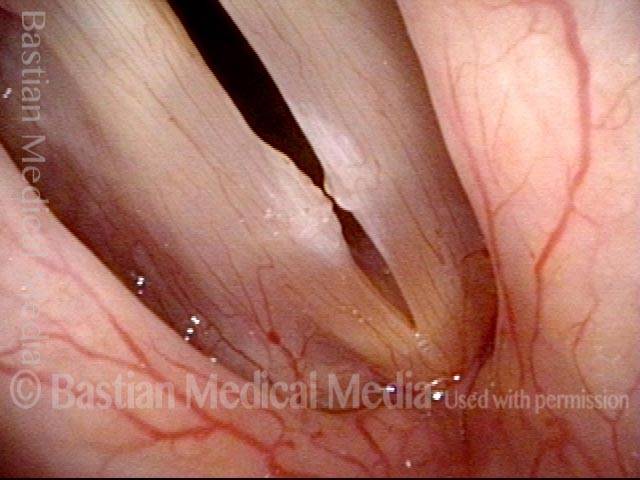
1 week after surgery (3 of 6)
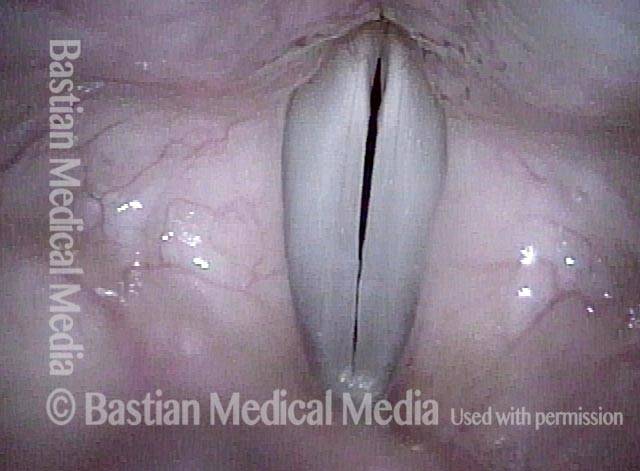
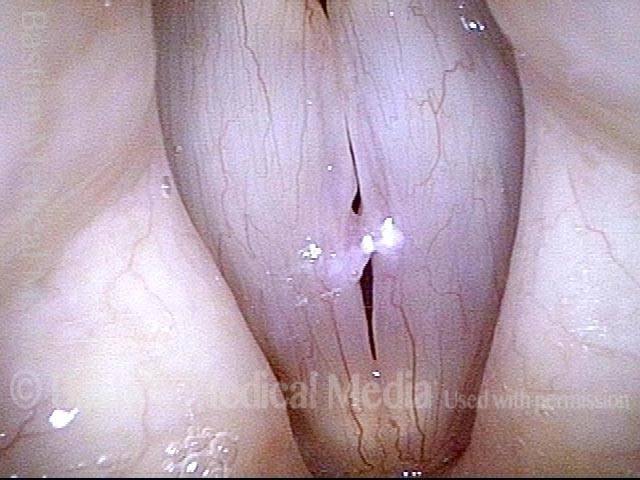
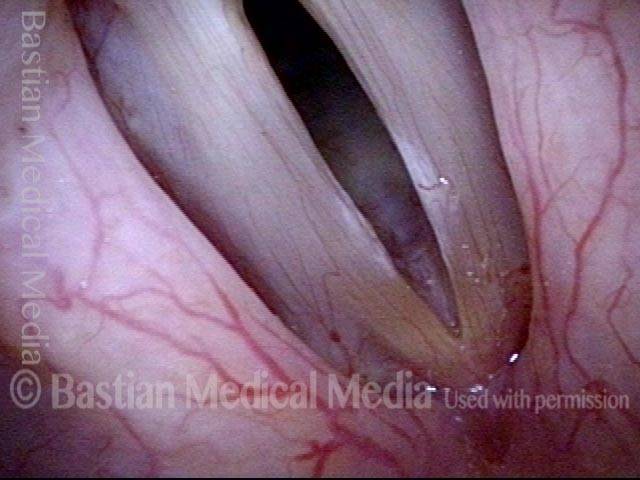
Closed phase (4 of 6)
7 weeks after surgery (5 of 6)
7 weeks after surgery (6 of 6)
 Vocal Cord Mucosa Vibratory Decoupling
Vocal Cord Mucosa Vibratory Decoupling
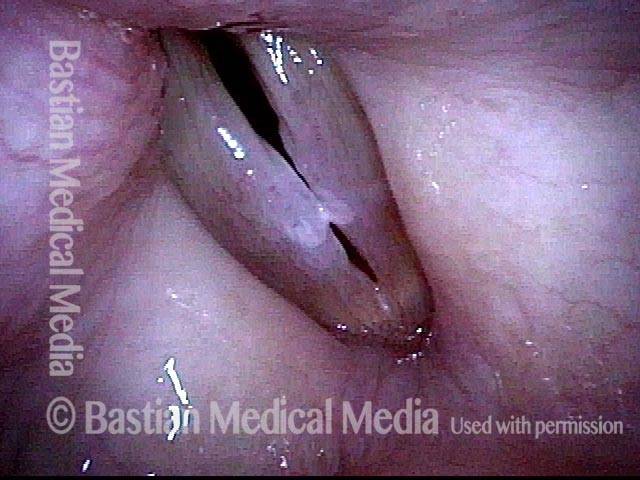
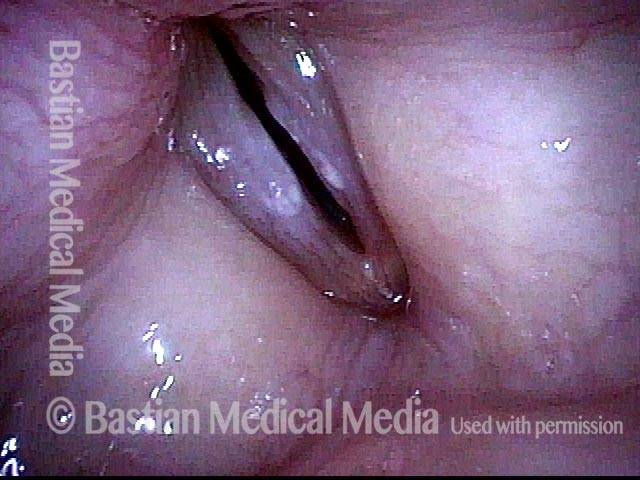
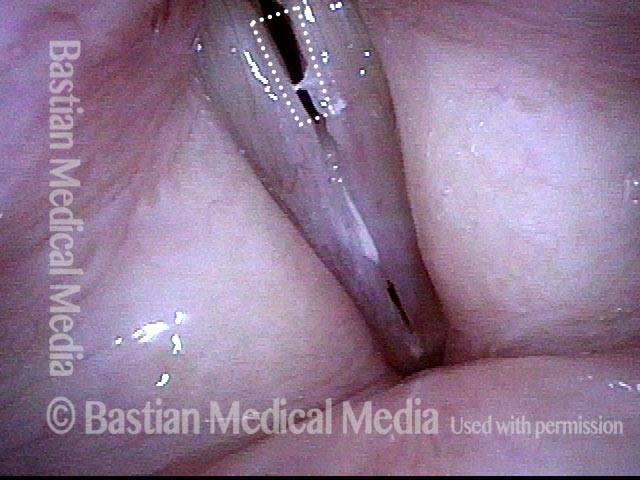
This series is designed to highlight the crucial importance of vocal cord mucosal flexibility—its ability to stretch and move independently of deeper structures. A surgical sequence illustrates this principle:
This singer requires removal of a polypoid nodule that therapy and time would not resolve from her right vocal cord. During the procedure, the polyp is gently grasped and tented away from the underlying vocal ligament and muscle, vividly demonstrating how stretchable the mucosa is.
Think of the way the skin on the back of your hand can be lifted without moving the hand itself. Another analogy is the classic child’s paddleball toy: the wooden paddle represents the muscle and vocal ligament, the red rubber ball corresponds to the epithelium (the surface layer of cells), and the elastic band connecting them symbolizes the flexible attachment layer to underlying structures that do not vibrate.
In surgery, the goal is to remove not just the superficial epithelium—which easily regenerates—but only a short segment of that elastic “rubber band.” By preserving most of this attachment layer, the newly regenerated epithelium won’t adhere directly to the deeper “paddle.” This maintains the mucosal pliability essential for optimal voice.
Vocal Cord Anatomy — Surgical View (1 of 8)

Mucosal “Stretch” Demonstration (2 of 8)

Skin-Stretch Analogy (3 of 8)

Limited Excision (4 of 8)

Vibratory Blur Analogy (5 of 8)

Post-Excision Result (6 of 8)

To review: Preop (7 of 8)

Final result (8 of 8)

Polypoid Vocal Nodules
Polypoid vocal nodules (1 of 4)

Incomplete closure (2 of 4)
Polypoid vocal nodules (3 of 4)
Polypoid vocal nodules (4 of 4)

Example 2 (Vocal Cord ‘Wounds,’ 2 Hours after Surgery)
Polypoid nodule, open phase (1 of 8)

Polypoid nodule, closed phase (2 of 8)
Polypoid nodule, right and left cords (3 of 8)
Segmental vibration (4 of 8)
Post-surgery wounds (5 of 8)

Post-surgery, closed phase (6 of 8)
Post-surgery, open phase (7 of 8)

Post-surgery, precise match (8 of 8)
Vocal Nodules, Before & After Surgery
Vocal nodules (1 of 10)

Prephonatory instant (2 of 10)

Translucency (3 of 10)

Open phase (4 of 10)
1 week after surgery (5 of 10)

1 week after surgery (6 of 10)
1 week after surgery (7 of 10)
Vocal nodules: 10 weeks after surgery (8 of 10)
10 weeks after surgery (9 of 10)
10 weeks after surgery (10 of 10)
Example 2
Vocal nodules (1 of 4)

Phonation (2 of 4)
After surgery (3 of 4)
After surgery (4 of 4)

Example 3
Vocal nodules, before surgery (1 of 4)
Before surgery (2 of 4)
After surgery (3 of 4)
Vocal nodules, after surgery (4 of 4)
Example 4 (Pre- & 1 Week Post-removal)
Vocal nodules (1 of 8)

Muscular tension dysphonia (2 of 8)
Open phase (3 of 8)
Closed phase (4 of 8)
Post-op, one week (5 of 8)
Phonation (6 of 8)
Open phase (7 of 8)
Closed phase (8 of 8)
Vocal Nodules, Spicule-shaped
Vocal nodules (1 of 3)

During phonation (2 of 3)

Closed phase (3 of 3)

Example 2
Vocal nodules (1 of 4)

Small nodules (2 of 4)
Phonation (3 of 4)
Open phase (4 of 4)
Fibrotic Nodules
Fibrotic nodules (1 of 5)

Fibrotic nodules: full-length vibration at low pitch (2 of 5)
Fibrotic nodules: full-length vibration at low pitch (3 of 5)
Fibrotic nodules: segmental vibration at high pitch (4 of 5)

Fibrotic nodules: segmental vibration at high pitch (5 of 5)
Example 2 (Fibrosis as a Base to Nodules, Before & After Surgery)
Bilateral polypoid nodules (1 of 8)
Narrow-band lighting (2 of 8)

Closed phase (3 of 8)

Open phase (4 of 8)

Two weeks after surgery (5 of 8)

Phonation (6 of 8)

Margin fibrosis (7 of 8)

Open phase (8 of 8)
More Examples of Vocal Nodules
Vocal nodules (1 of 4)
Prephonatory instant (2 of 4)
Open phase of vibration (3 of 4)
Closed phase of vibration (4 of 4)
Example 2
Vocal nodules (1 of 2)

Vocal nodules (2 of 2)

Example 3
Vocal nodules (1 of 1)
Example 4
Vocal nodules (1 of 1)
Example 5 (Vocal Nodule Postop Irregularity yet Match & Flexibility)
Large vocal nodules (1 of 8)
Narrow band light (2 of 8)

At B2 (3 of 8)
At A5 (4 of 8)

One week after surgery (5 of 8)
Prephonatory instant (6 of 8)
Closed phase (8 of 8)

Open phase (7 of 8)

Search not Only for Nodules, but Also for Segmental Vibration and Look at the Posterior Commissure for MTD
Open phase (1 of 4)
Closed phase (2 of 4)
Segmental vibration (3 of 4)

Posterior commissure (4 of 4)
Ask Both Voice (via vocal phenomenology) and Larynx (via a motivated examination) to Give up their Secrets
Obvious mucosal injury (1 of 3)

Vocal nodules (2 of 3)

Capillary ectasia (3 of 3)

Mottled Vocal Cord Mucosa May Hide Glottic Sulci
Vocal cord swelling and mucosa (1 of 4)

Same view under strobe light (2 of 4)

Closed phase (3 of 4)

Glottic sulcus is visible (4 of 4)

Vocal Nodules, Leukoplakia, & Capillary Ectasia
Vocal nodules, leukoplakia, and capillary ectasia (1 of 4)
Vocal nodules, leukoplakia, and capillary ectasia (2 of 4)
Vocal nodules, leukoplakia, and capillary ectasia: 6 months later (3 of 4)
Vocal nodules, leukoplakia, and capillary ectasia: 6 months later (4 of 4)