Un disturbo in cui tumori simili a verruche o altre lesioni crescono in modo ricorrente all’interno delle vie aeree di una persona. Queste escrescenze sono causate dal papillomavirus umano (HPV) e possono verificarsi ovunque nelle vie aeree di una persona, come sulle corde vocali (di gran lunga il sito più comune), nella laringe sopraglottica o nella trachea. Se queste escrescenze vengono rimosse, ricresceranno quasi sempre o si ripresenteranno; quindi, “papillomatosi respiratoria ricorrente”.
Sintomi e rischi di papillomatosi respiratoria ricorrente
La RRP può essere pericolosa per la vita nei bambini piccoli, se non seguita e trattata attentamente, poiché le vie aeree di un bambino sono relativamente strette e possono potenzialmente essere completamente ostruite dalle escrescenze proliferative della malattia; inoltre, la RRP nei bambini tende a crescere ea ripresentarsi in modo più aggressivo.
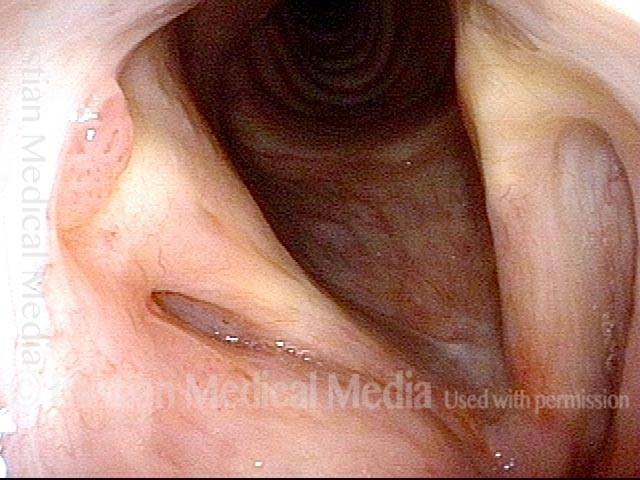
Negli adulti, la RRP di solito compromette solo la funzione vocale (quando le escrescenze si verificano sulle corde vocali), sebbene possa anche compromettere la respirazione nei casi più gravi. Occasionalmente, la RRP può anche progredire verso il cancro, e quindi i pazienti che risultano essere ad alto rischio per questo (vedi sotto) devono essere monitorati attentamente.
Caratteristiche delle crescite
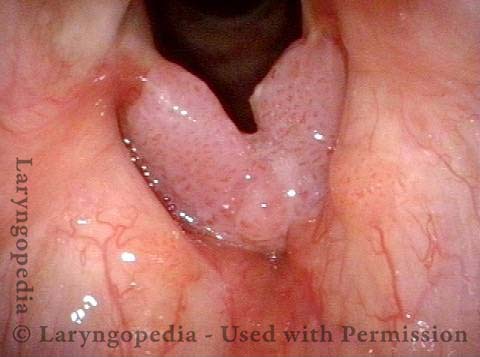
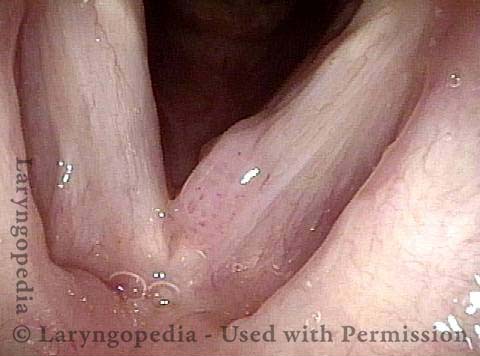
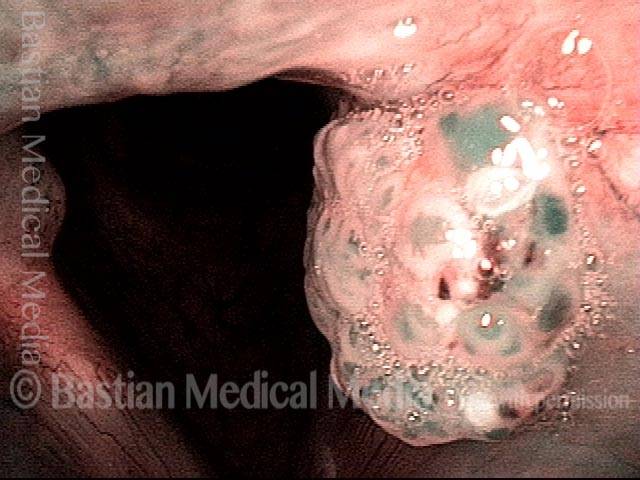
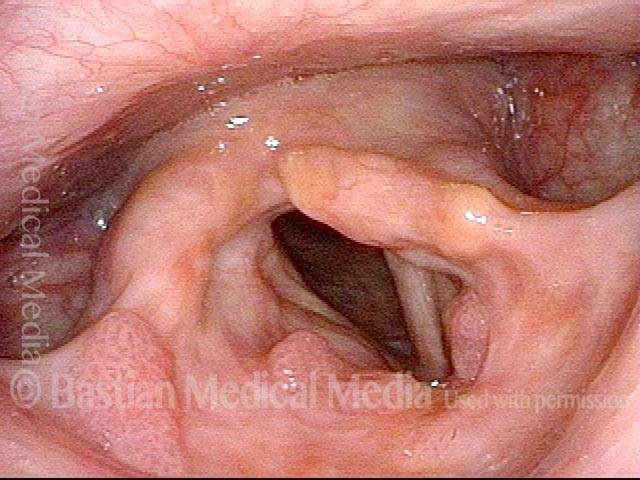
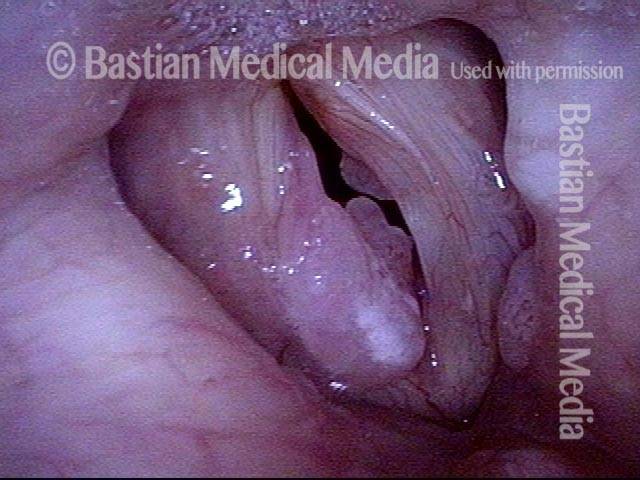
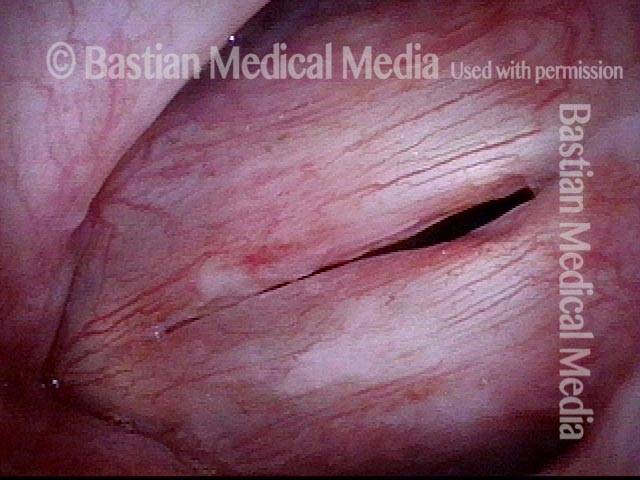
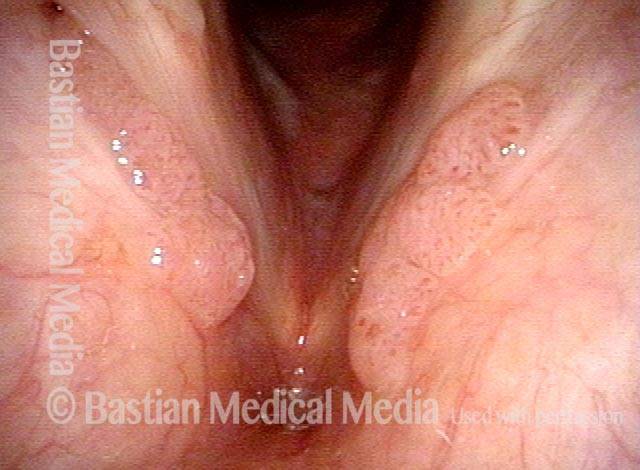
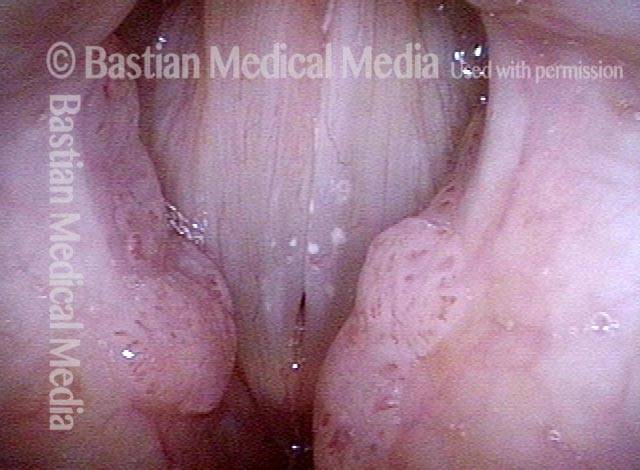
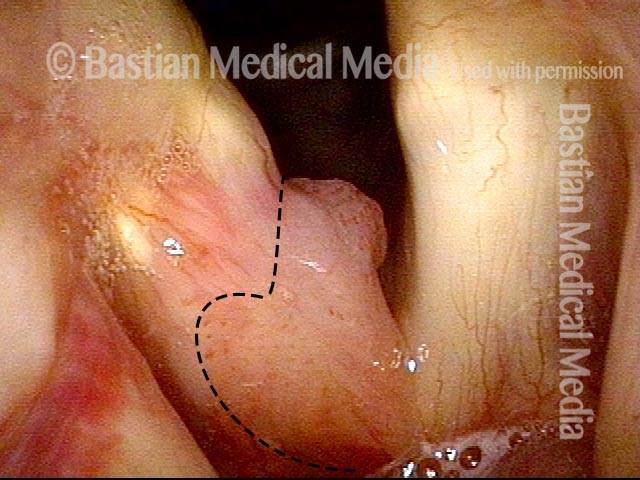
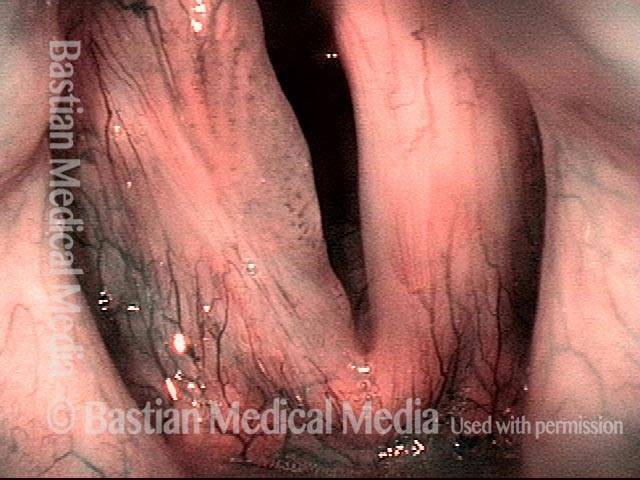
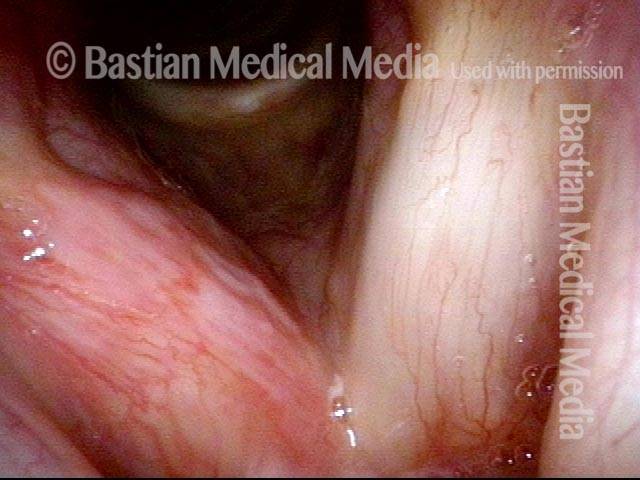
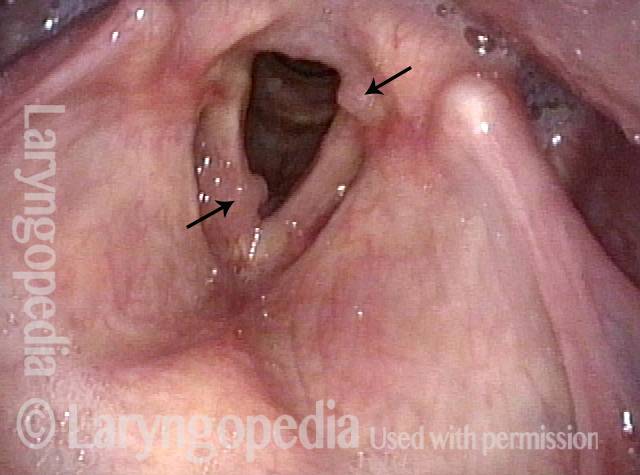
Le escrescenze solitamente associate a RRP sono tumori simili a verruche, o papillomi, che sporgono in modo evidente dalla superficie su cui crescono, spesso in grappoli simili a grappoli. Questi tipi di papillomi si osservano solitamente in pazienti con sottotipi di HPV 6 o 11, che sono entrambi sottotipi a basso rischio di contrarre il cancro.
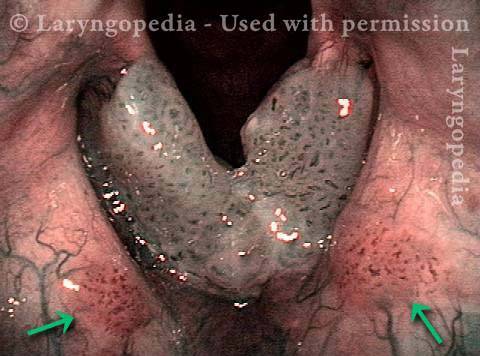
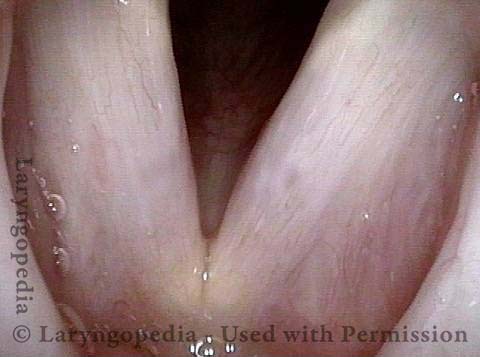
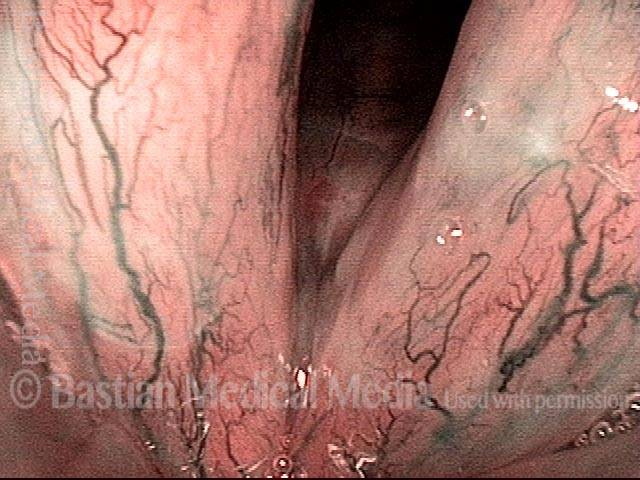
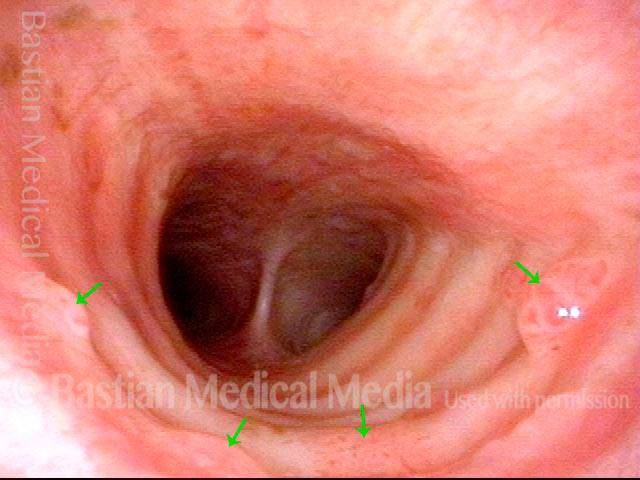
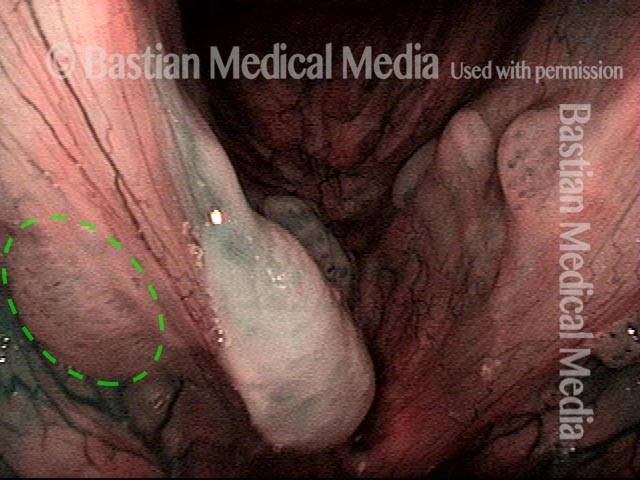
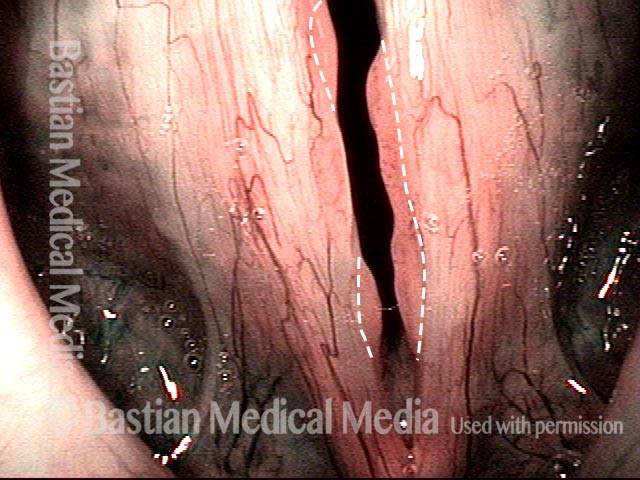
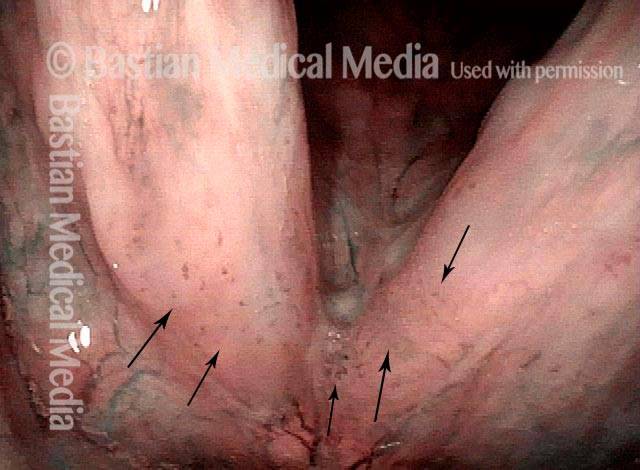
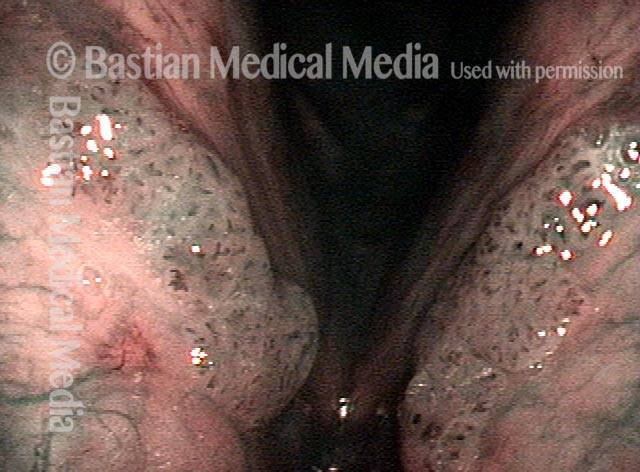
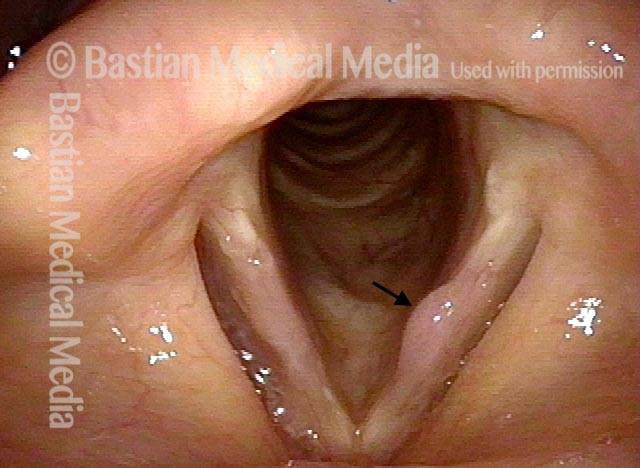
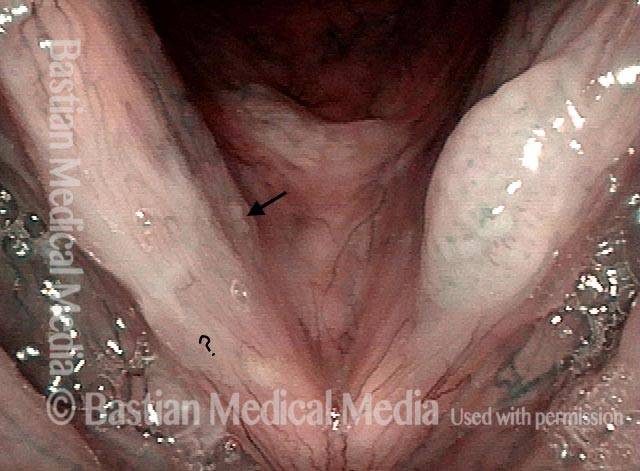
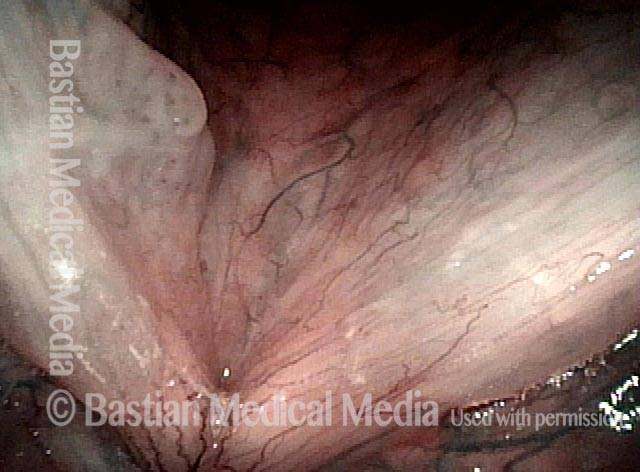
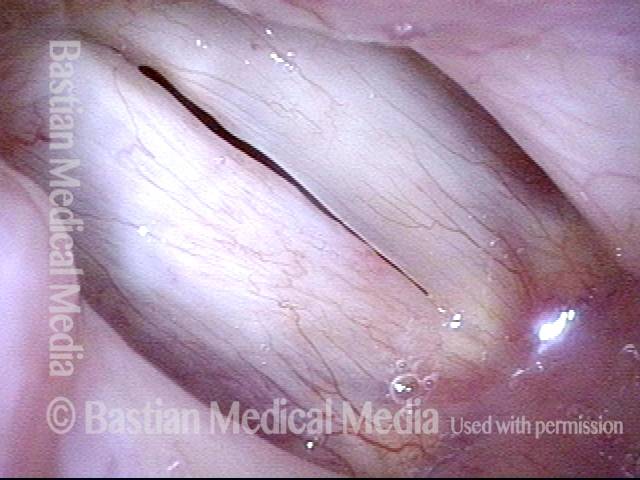
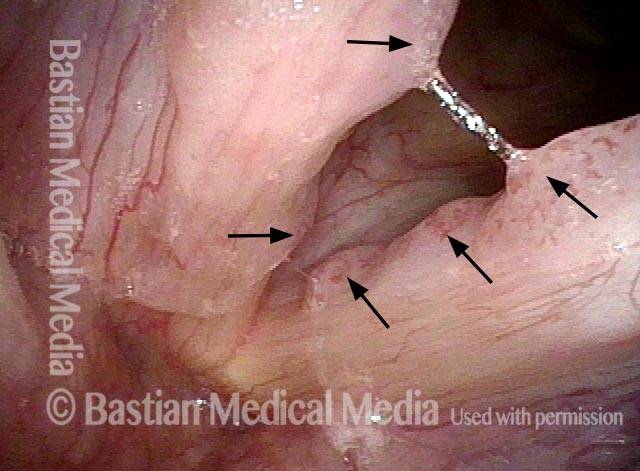
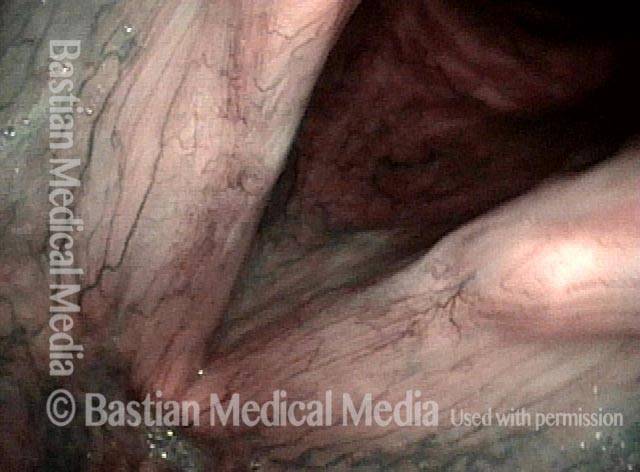
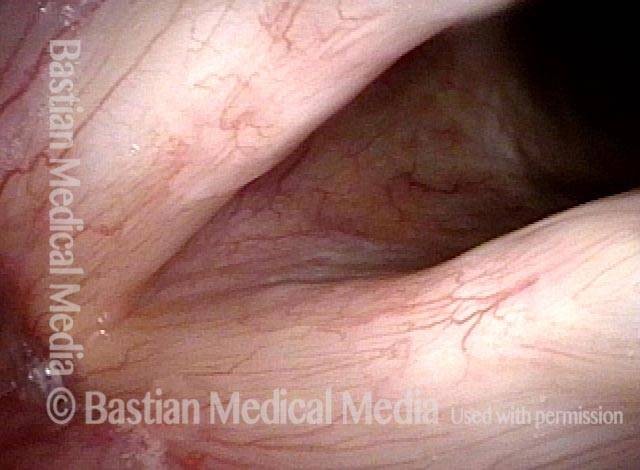
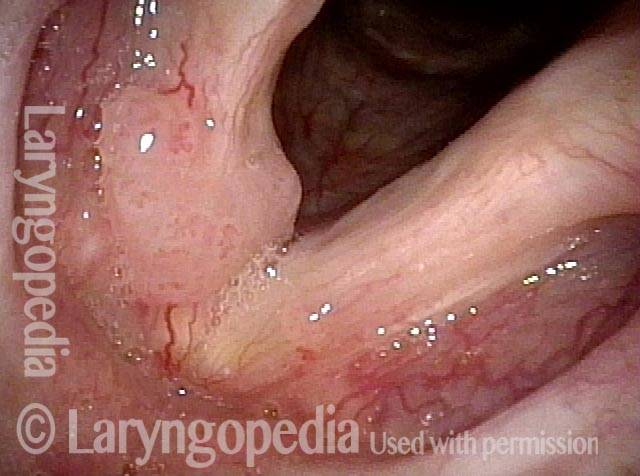
Ci sono alcuni pazienti HPV, tuttavia, che manifestano la loro infezione da HPV con escrescenze più sottili e vellutate all’interno delle vie aeree, escrescenze “varianti a tappeto”, per così dire. Sebbene queste escrescenze “varianti a tappeto” non abbiano l’aspetto simile a una verruca dei papillomi tipicamente associati a RRP, ci sono almeno alcuni punti chiave di somiglianza:
- Both the “carpet-variant” and wart-like growths are lesions that sometimes appear, either independently or together, in patients who have HPV;
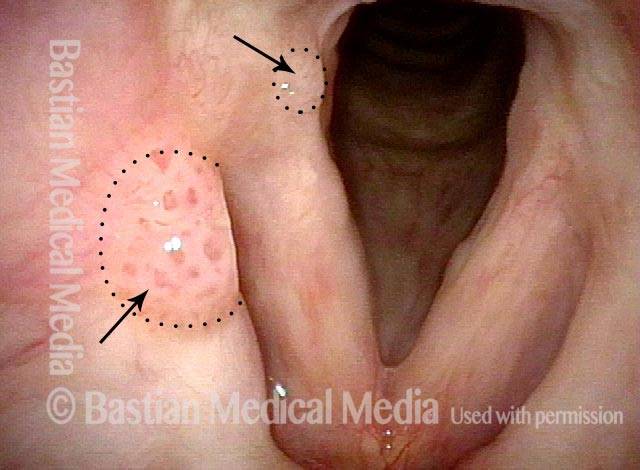
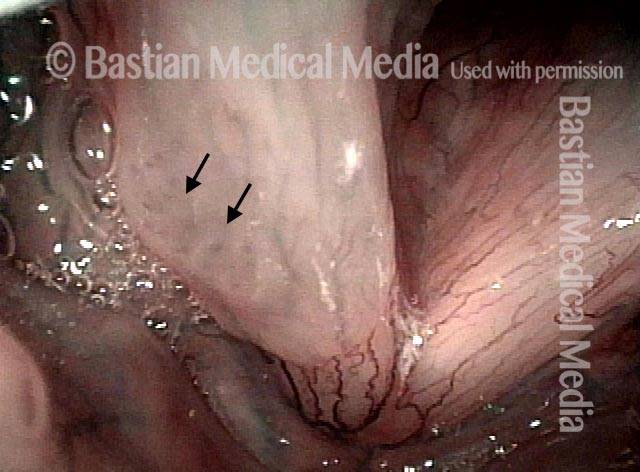
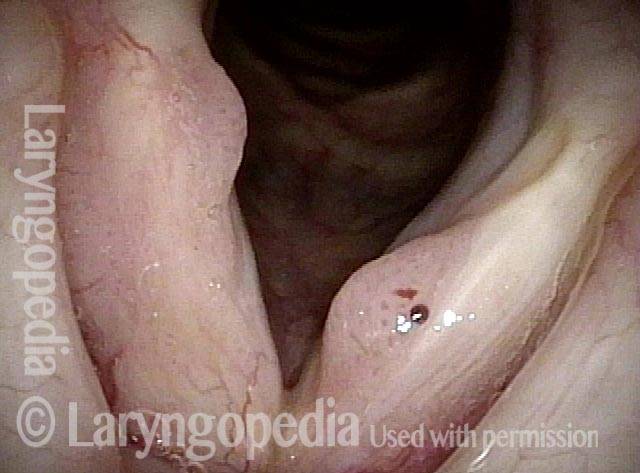
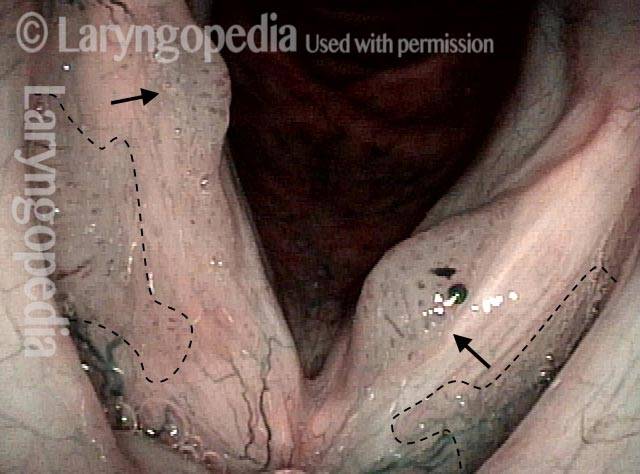
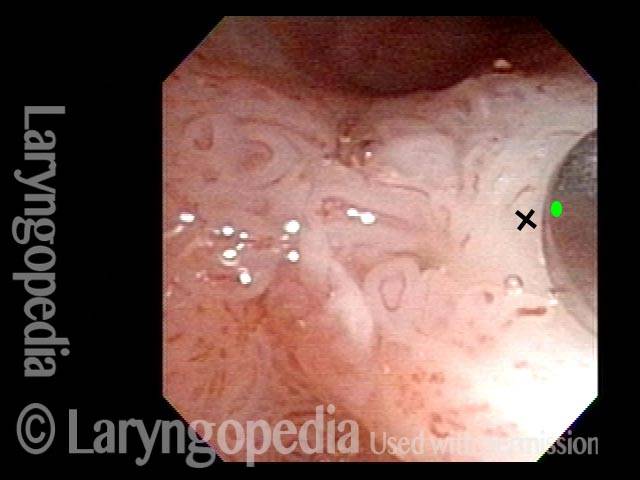
- Both the “carpet-variant” and wart-like growths are stippled with polka-dot vascular markings, because each “loop” in the “carpet” or each “grape” in the wart-like cluster has its own fibrovascular core, seen as a red dot;
- Both the “carpet-variant” and wart-like growths can disrupt voice function;
- Both the “carpet-variant” and wart-like growths usually recur if they are removed.
Because of these similarities, we consider these “carpet-variant” growths, even when the sole expression of the infection, to be at least a cousin to RRP, within the family of HPV-induced lesions. Many patients with this “carpet-variant” condition have HPV subtypes such as 16 or 18 that are higher-risk for cancer; such patients need to be monitored with particular care.
Trattamento della papillomatosi respiratoria ricorrente
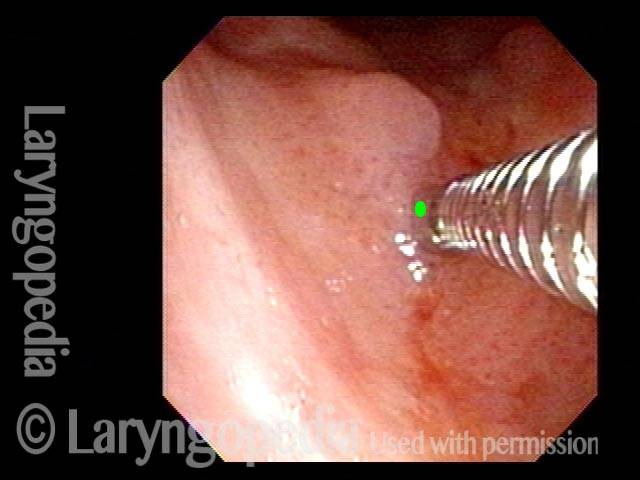
Il trattamento primario per RRP e altre lesioni indotte da HPV è la rimozione chirurgica attenta e conservativa delle escrescenze. Poiché queste escrescenze si ripresentano quasi sempre, l’intervento chirurgico di solito deve essere eseguito su base ripetuta, ogni poche settimane nei bambini, ma in media molto meno spesso negli adulti. Un intervallo comune tra gli interventi chirurgici per i pazienti adulti è tra ogni sei mesi e ogni due anni, a seconda della velocità con cui la RRP o altra lesione correlata all’HPV si ripresenta e compromette nuovamente la funzione vocale del paziente.
Ci sono anche alcuni trattamenti medici che sono stati utilizzati in aggiunta alla chirurgia, tra cui, tra gli altri, interferone, indolo-3-carbinolo, vaccino intralesionale contro la parotite o MPR (morbillo-parotite-rosolia), cidofovir e bevacizumab.
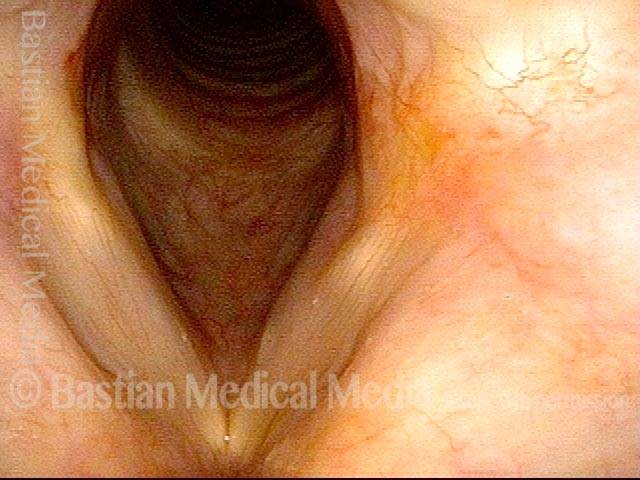
Umiltà davanti al virus HPV: una recidiva di papillomi a dieci anni
L’infezione da HPV è considerata cronica e provoca una crescita ricorrente di papillomi nella laringe. Tuttavia, a volte vediamo quelle che sembrano cure, o almeno remissioni a lungo termine. Questo sembra essere il caso qui. Dopo un intervallo di 8 anni di voce perfetta, il paziente ha avuto un improvviso aumento della raucedine verificatosi nelle poche settimane precedenti l’ultimo esame di seguito. Questo è un esempio del motivo per cui spesso diciamo a un paziente che sembra essere guarito: “Potresti essere guarito, ma di solito diciamo” remissione a lungo termine “. Lo scenario di questo paziente non è raro. La sua remissione a lungo termine di 8 anni è stata dovuta a un meticoloso intervento chirurgico? Cidofovir? La sua risposta immunitaria? È impossibile dire se sia stato uno o tutti questi fattori.
Stippled Vascularity (1 of 8)
HPV infection (2 of 8)
Stippled vascularity (3 of 8)

HPV vascular effect (4 of 8)

16 months later (5 of 8)
Is it long-term remission? (6 of 8)

Recurrent Papilloma (7 of 8)
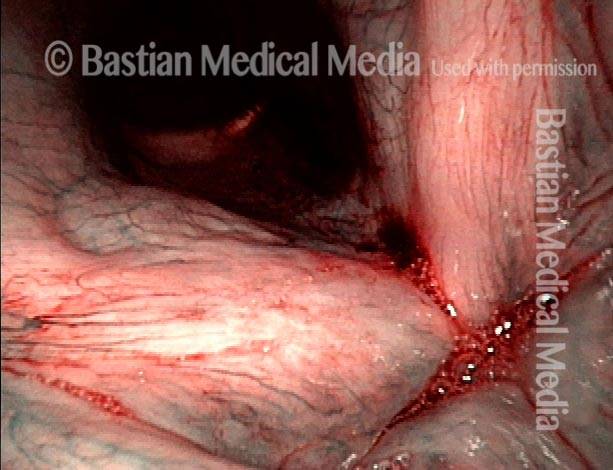
Stippled vascularity (8 of 8)

Papillomi, sottotipo HPV 11, prima e dopo la rimozione
Papillomas: HPV Subtype 11 (1 of 4)

Papillomas: HPV Subtype 11 (2 of 4)
Papillomas, removed: HPV Subtype 11 (3 of 4)
Papillomas, removed: HPV Subtype 11 (4 of 4)

Papillomi, HPV sottotipo 6, prima e dopo la rimozione
Papillomas: HPV Subtype 6 (1 of 4)

Papillomas: HPV Subtype 6 (2 of 4)

Papillomas, removed: HPV Subtype 6 (3 of 4)

Papillomas, removed: HPV Subtype 6 (4 of 4)
Papillomi, HPV sottotipo 11
Papillomas: HPV Subtype 11 (1 of 3)
Papillomas: HPV Subtype 11 (2 of 3)
Papillomas: HPV Subtype 11 (3 of 3)

Esempio 2
Papillomas: HPV Subtype 11 (1 of 2)

Papillomas: HPV Subtype 11 (2 of 2)
Lesioni da HPV
Lesions of HPV Subtype? (1 of 2)

Lesions of HPV Subtype? (2 of 2)

Lesioni e papillomi da HPV, prima e dopo la rimozione e l’iniezione adiuvante
Lesions and papillomas of HPV subtype? (1 of 8)

Subtle lesion (2 of 8)
Open phase (3 of 8)
1 week after removal (4 of 8)

1 week after removal (5 of 8)
Injecting adjuvant (6 of 8)
After injecting adjuvant (7 of 8)
After final adjuvant injection (8 of 8)

Papillomi, sottotipo HPV 55, in fase di remissione
Papillomas: HPV Subtype 55 (1 of 4)

Papillomas: HPV Subtype 55 (2 of 4)

Papillomas, in remission: HPV Subtype 55 (3 of 4)

Papillomas, in remission: HPV Subtype 55 (4 of 4)
Papillomi, HPV sottotipo 31, andando in remissione
Papillomas: HPV Subtype 31 (1 of 4)
Papillomas: HPV Subtype 31 (2 of 4)
Papillomas, in remission: HPV Subtype 31 (3 of 4)
Papillomas, in remission: HPV Subtype 31 (4 of 4)

Papillomi, HPV
Papillomas: HPV Subtype? (1 of 2)

Papillomas: HPV Subtype (2 of 2)

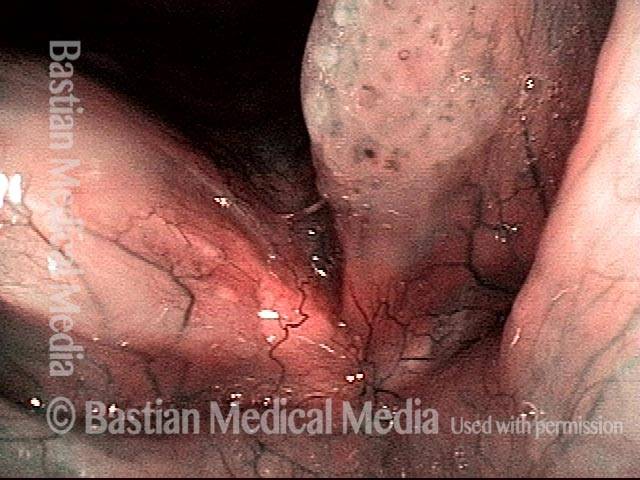
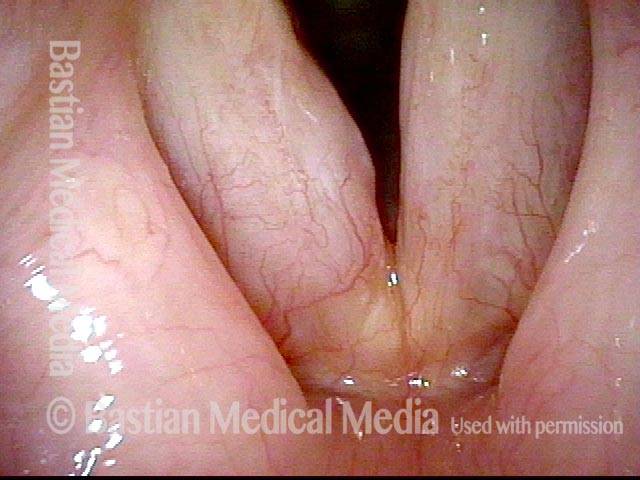
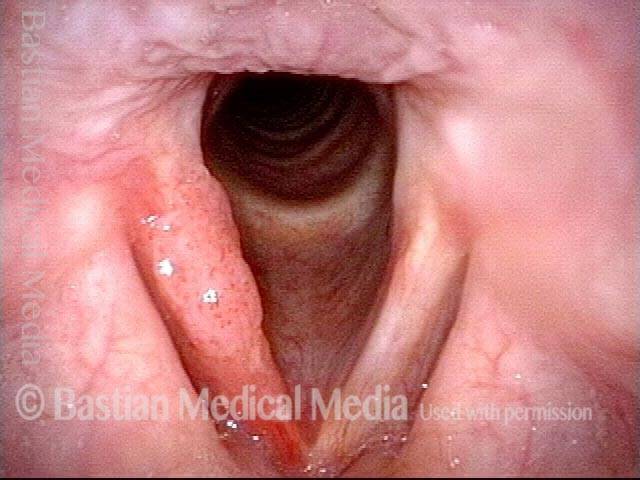
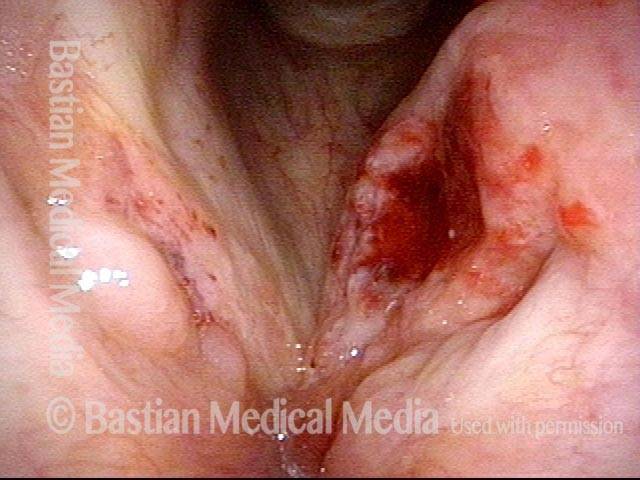
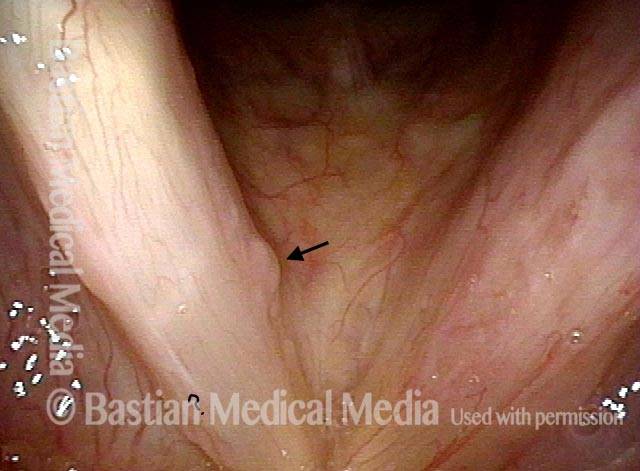
Superare le false piste per trovare il vero problema
Obvious lesion not important (1 of 3)

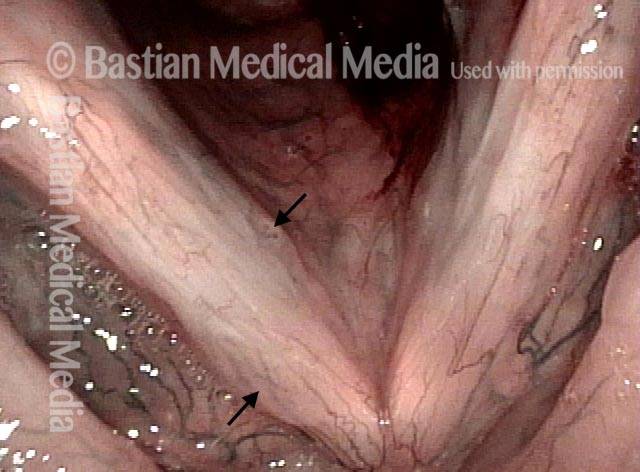
Granuloma (2 of 3)

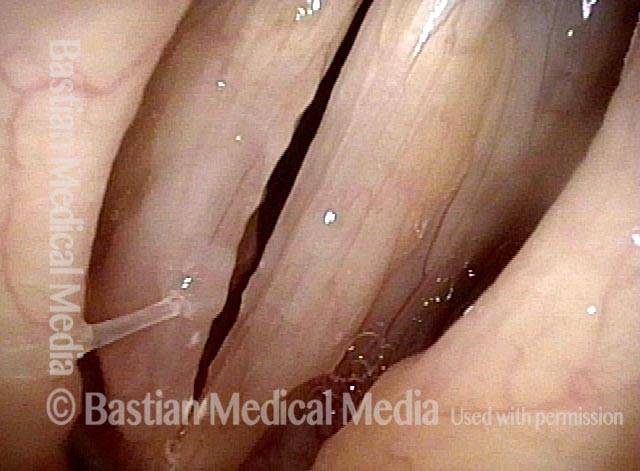
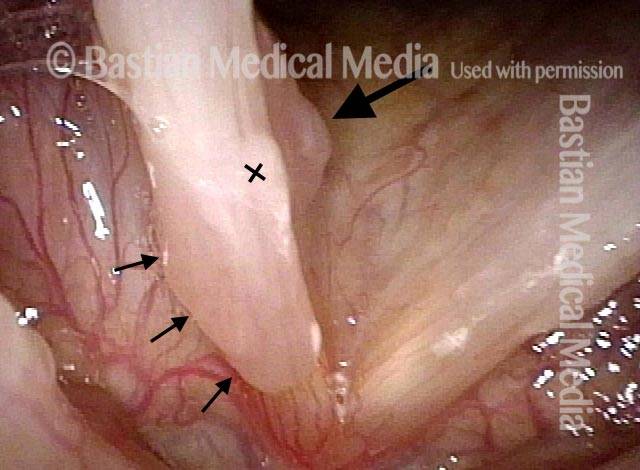
Carpet-varient papilloma (3 of 3)

Papillomi, sottotipo HPV 18 o 45
Papillomas: HPV Subtype 18 or 45 (1 of 2)
Papillomas: HPV Subtype 18 or 45 (2 of 2)

Lesioni di HPV sottotipo 16
Lesions of HPV Subtype 16 (1 of 3)

Lesions of HPV Subtype 16 (2 of 3)

Lesions of HPV Subtype 16 (3 of 3)

Cancro, HPV sottotipo 16, prima e dopo la radiazione
Cancer: HPV Subtype 16 (1 of 5)
Cancer: HPV Subtype 16 (2 of 5)
Cancer: HPV Subtype 16, after radiation therapy (3 of 5)

Cancer: HPV Subtype 16, after radiation therapy (4 of 5)
Cancer: HPV Subtype 16, after radiation therapy (5 of 5)
Papillomi, HPV sottotipo 45
Papillomas: HPV Subtype 45 (1 of 2)
Papillomas: HPV Subtype 45 (2 of 2)

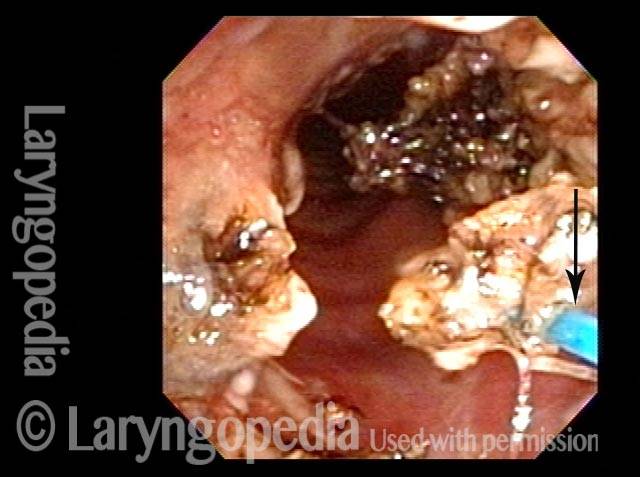
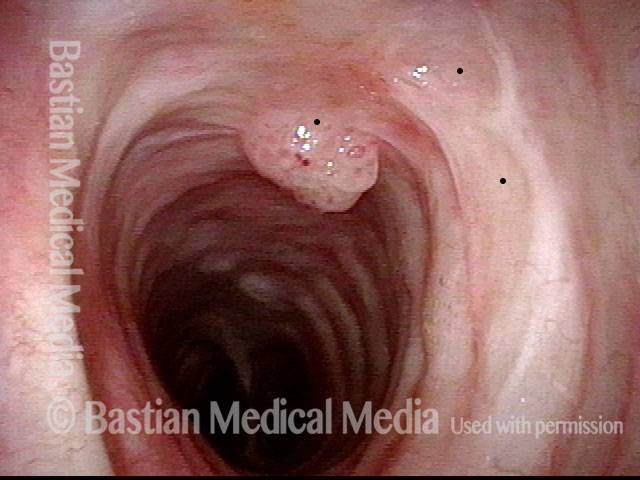
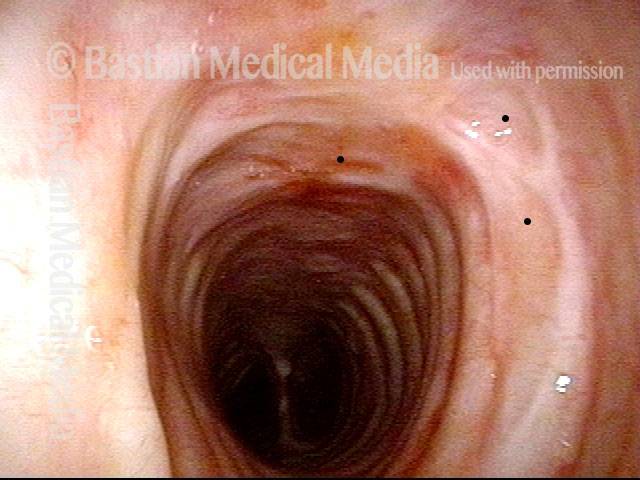
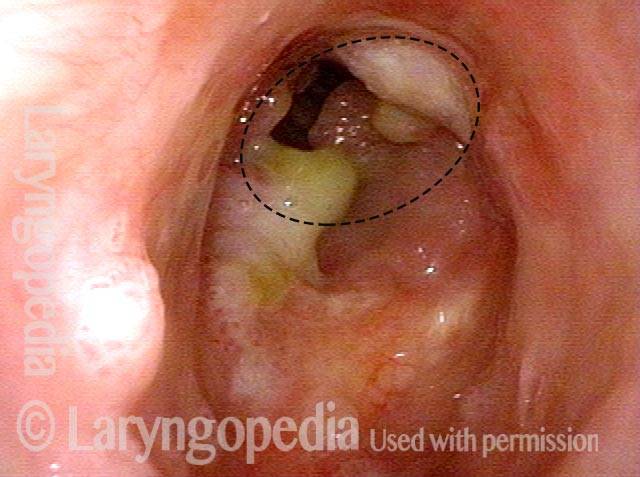
Papilloma medio-tracheale, trattato con laser al tulio
Mid-tracheal papilloma, being treated by thulium laser (1 of 5)
Months after treatment: no papilloma (5 of 5)
Mid-tracheal papilloma, being treated by thulium laser (2 of 5)
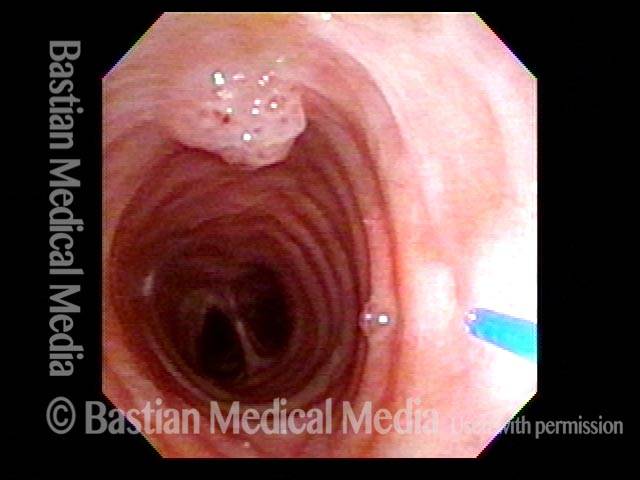
Mid-tracheal papilloma, being treated by thulium laser (3 of 5)

Mid-tracheal papilloma, being treated by thulium laser (4 of 5)

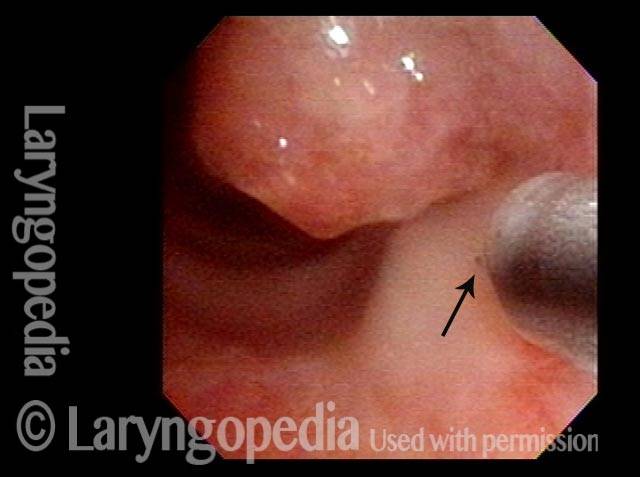
Papillomi sottili, HPV sottotipo 6
Subtle papillomas, HPV subtype 6 (1 of 3)
Subtle papillomas, HPV subtype 6 (2 of 3)

Subtle papillomas, HPV subtype 6 (3 of 3)
Effetto vascolare dell’HPV
Two papillomas (1 of 3)
Stippled vascularity (2 of 3)

HPV vascular effect (3 of 3)
Papillomi laringei Raramente possono essere trovati da … Accident
Papilloma finding (1 of 4)
Narrow band light (2 of 4)
Closed phase (3 of 4)
Open phase (4 of 4)

Vincere le battaglie contro il papilloma, ma non vincere la guerra… Ancora
Left vocal cord lesion (1 of 8)
Narrow band light (2 of 8)
One week after removal (3 of 8)
2 months after removal (4 of 8)
7 months after removal (5 of 8)
Papilloma and mucus (6 of 8)
Stippled vascularity (7 of 8)
HPV disease (8 of 8)
Cosa ha “guarito” questo caso di RRP? Chirurgia? Cidofovir? Il sistema immunitario del paziente? Tutti e tre?
Papilloma (1 of 8)
Stippling (2 of 8)

One week after surgical removal (3 of 8)

Cidofovir injection (4 of 8)
Six months after surgical removal (5 of 8)
One week after second removal (6 of 8)
4 months later, healed (7 of 8)

3 years later, no sign of papilloma (8 of 8)
Cura RRP? O solo remissione a lungo termine?
Chronic hoarseness (1 of 4)
4 months later (2 of 4)
8 months from start of treatment (3 of 4)
Narrow band lighting (4 of 4)

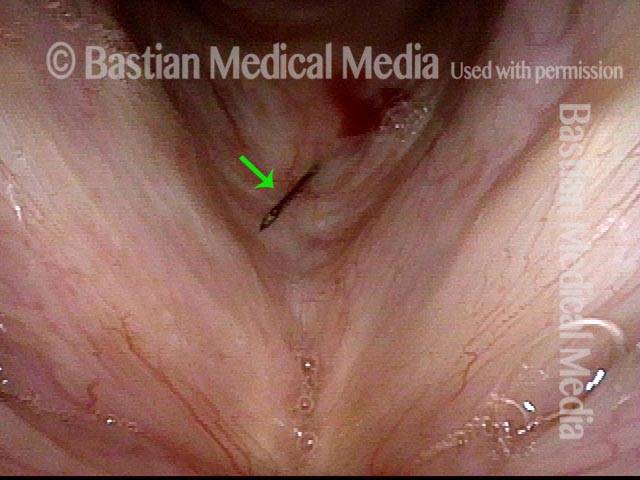
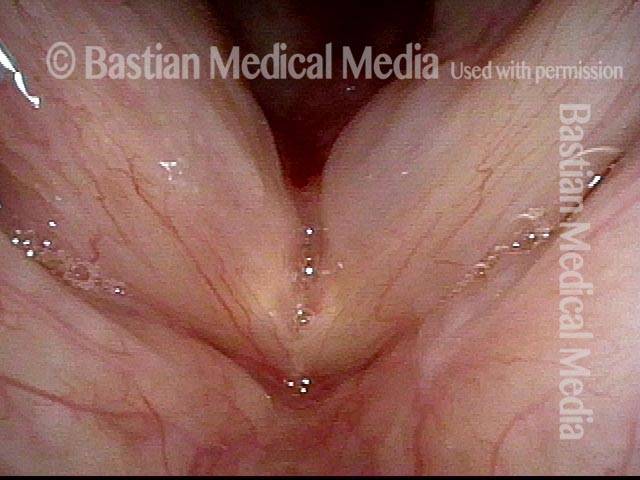
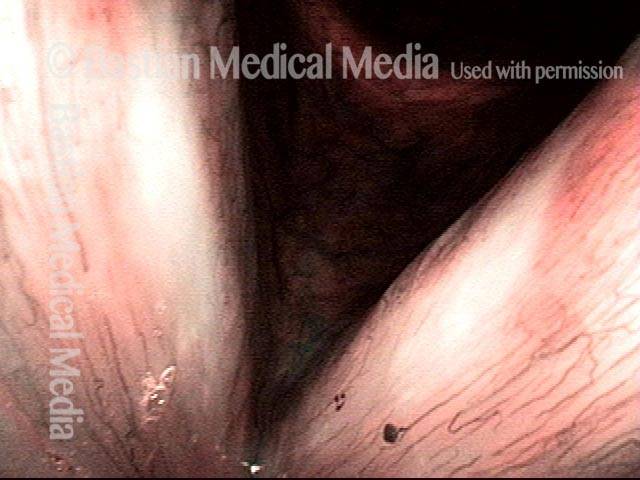
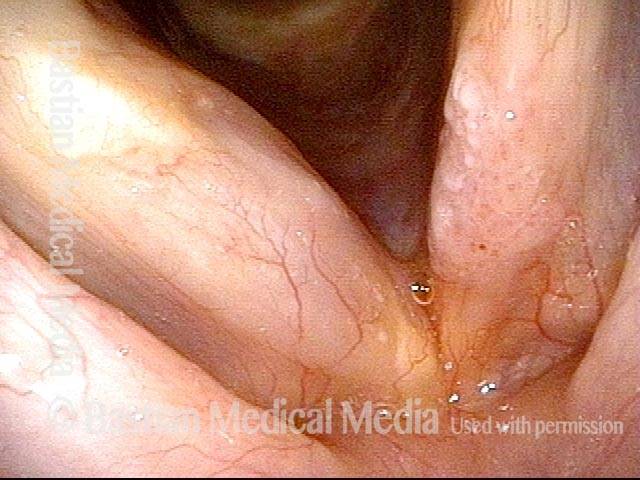
I polipi hanno bisogno di uno sguardo da vicino: ecco uno dei motivi per cui
“Polyps” diagnosis (1 of 4)

Papillomas (2 of 4)
Vascular stippling (3 of 4)
Prephonatory instant (4 of 4)

Remissione a lungo termine o addirittura “cura” di RRP/papilloma laringeo
Chronic hoarseness (1 of 6)
Narrow band light (2 of 6)

Higher magnification (3 of 6)
Higher magnification, narrow band lighting (4 of 6)

Post-operation (5 of 6)

Post-operation, narrow band lighting (6 of 6)

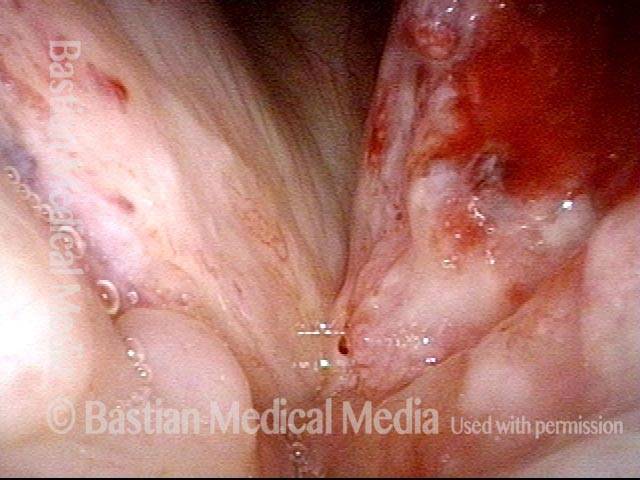
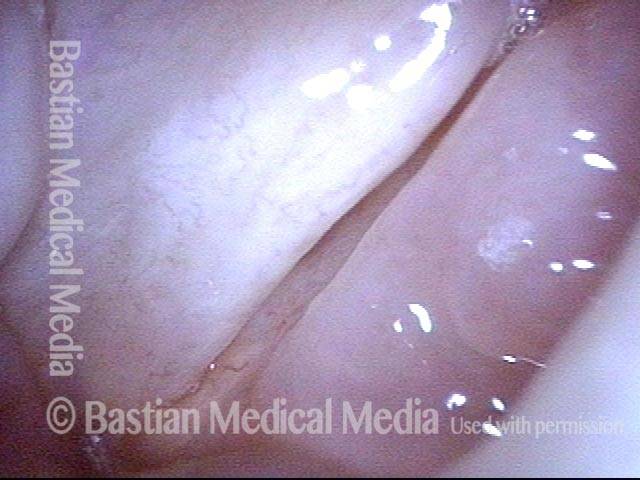
Anestetico locale iniettato provoca sbiancamento
Infiltrating anesthetic (1 of 3)

Blanching (2 of 3)
Subglottis being injected (3 of 3)
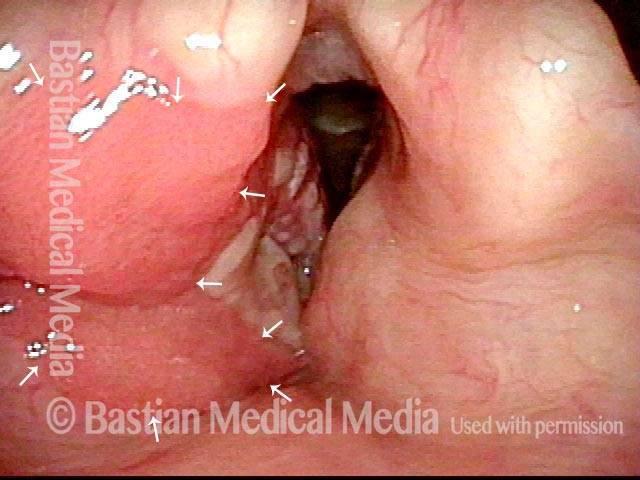
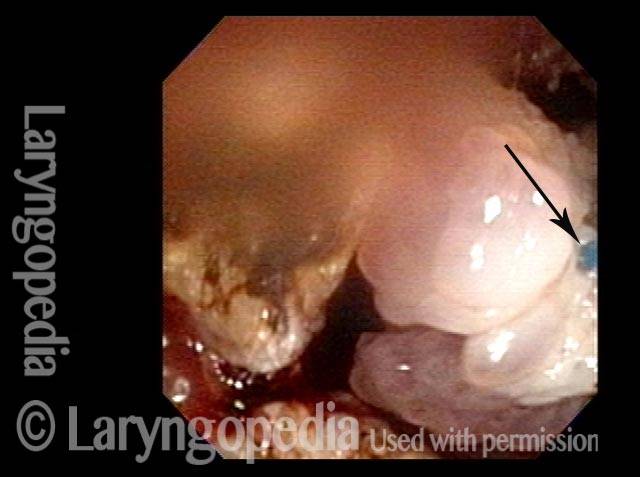
L’anestesia locale piuttosto che quella topica può consentire un intervento chirurgico tracheale abbastanza importante
Obstructive papillomas (1 of 4)
Local injections (2 of 4)
Removal of papilloma (3 of 4)
Improved breathing with papilloma removal (4 of 4)