
Paralisi delle Corde Vocali Definita dalla Denervazione di 3 Muscoli Individuali Piuttosto che dalla Mancata Funzionalità del Nervo Ricorrente
La paralisi delle corde vocali è solitamente definita come una corda immobile e il pensiero corre direttamente alla lesione del nervo ricorrente. La “definizione” visiva più universalmente utilizzata è la perdita di abduzione (sebbene vi sia anche una perdita di compressione mediale). In altri termini, tendiamo a pensare che il nervo ricorrente sia “fuori uso”, ma non che i tre muscoli individuali siano denervati di conseguenza. Al contrario, la paresi è definita dalla denervazione di uno (o due) dei seguenti muscoli:
- Cricoaritenoide posteriore (PCA)
- Cricoaritenoide laterale (LCA)
- Tiroaritenoide (TA)
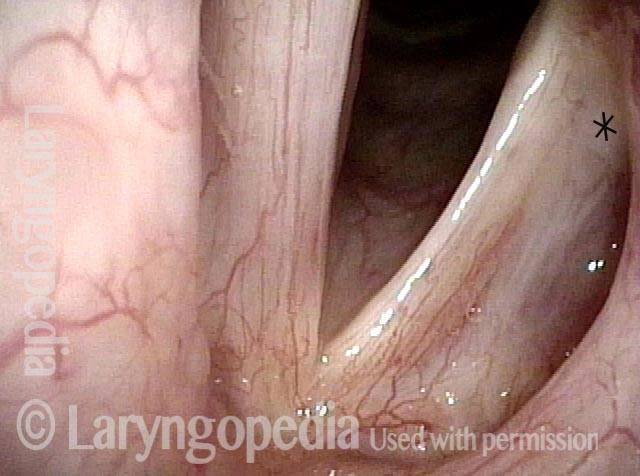
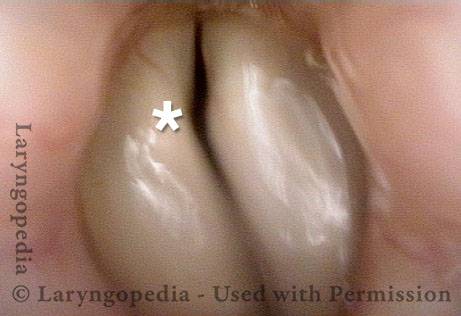
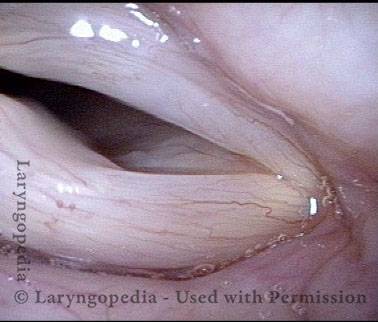
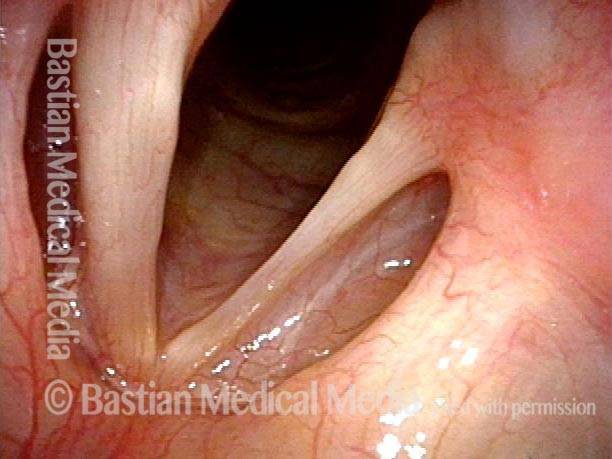
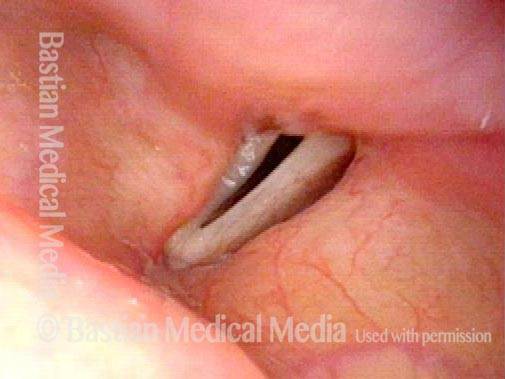
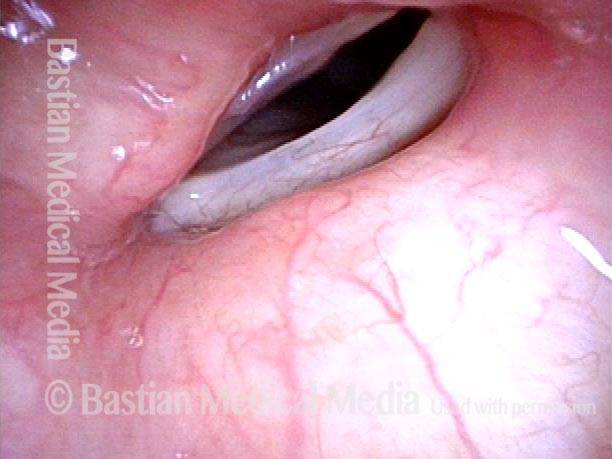
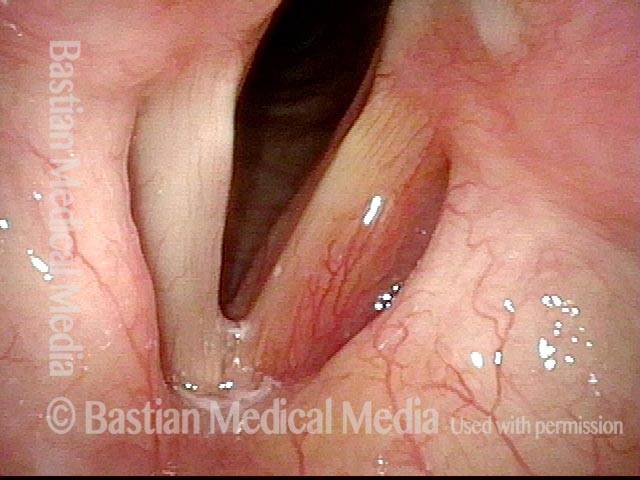
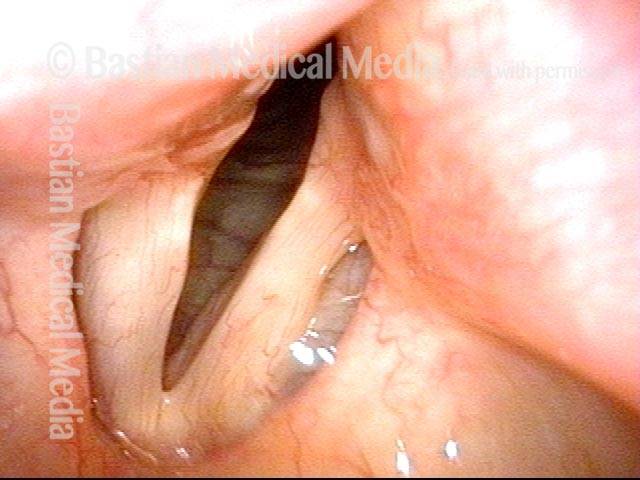
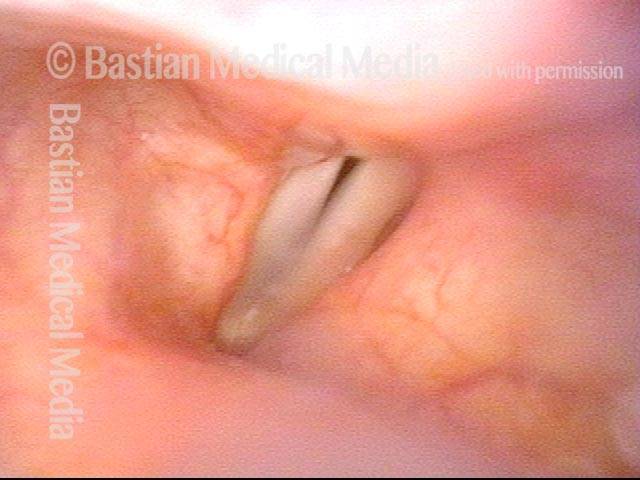
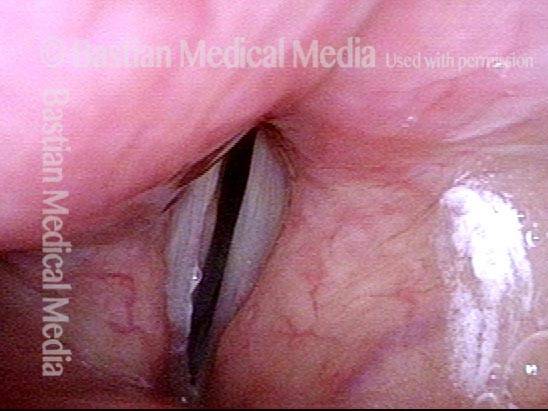
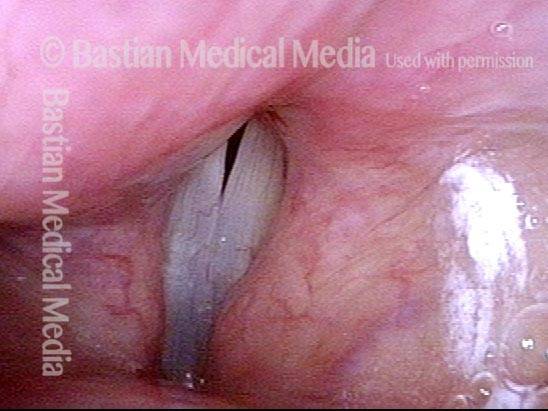
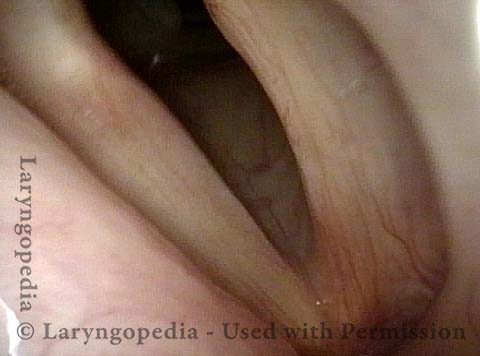
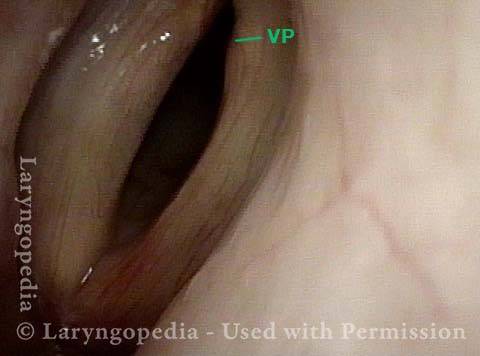
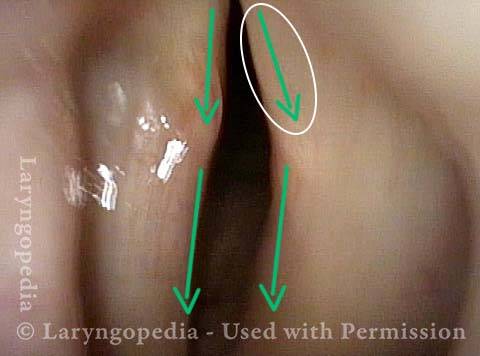
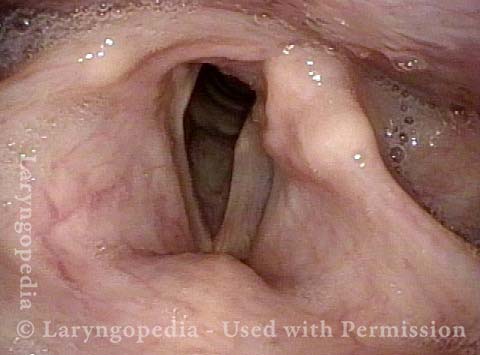
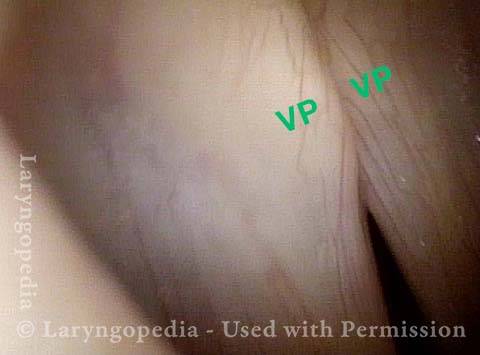
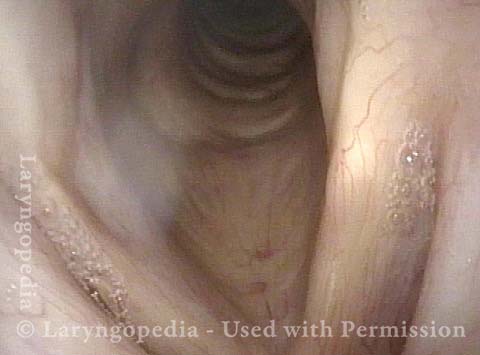
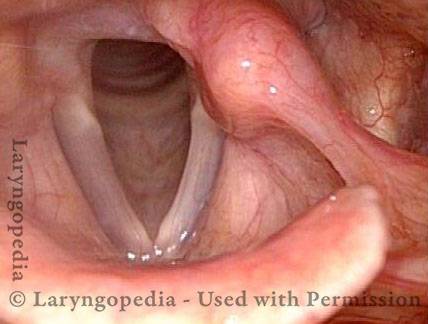
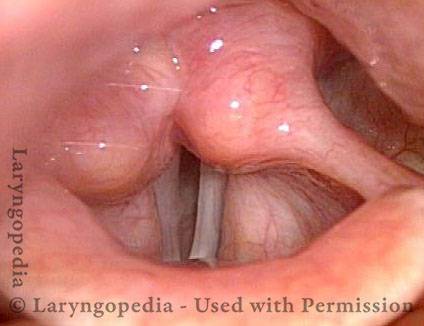
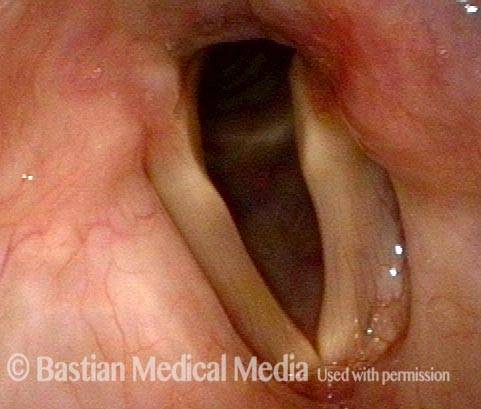
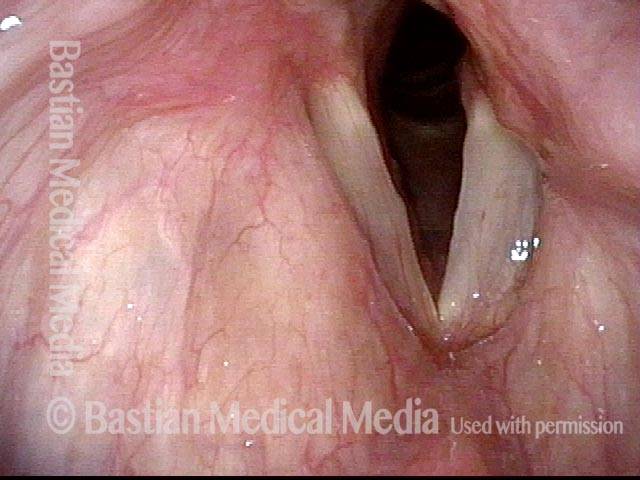
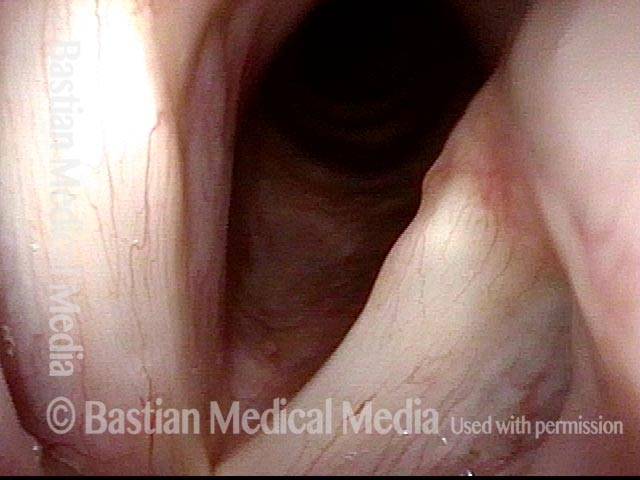
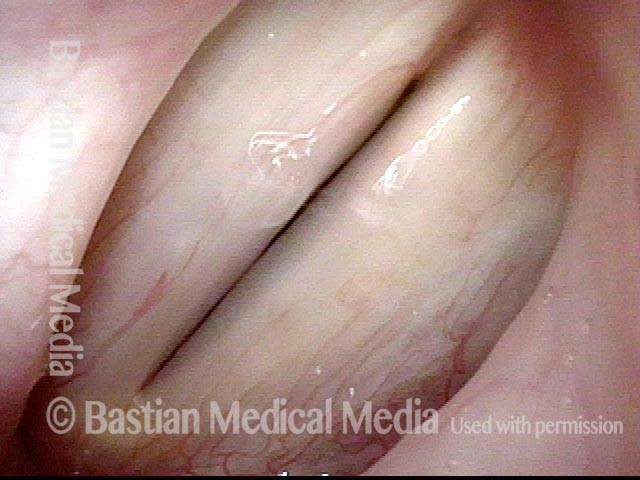
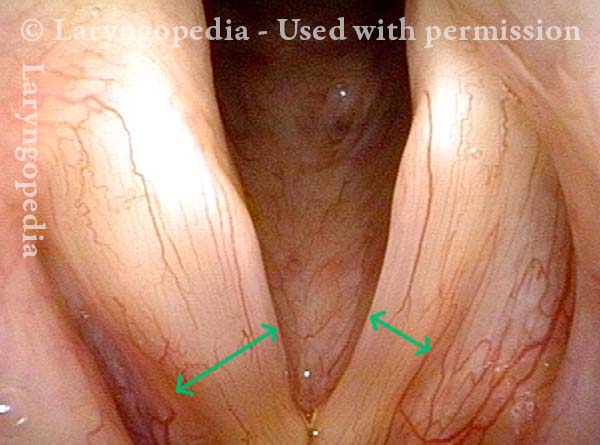
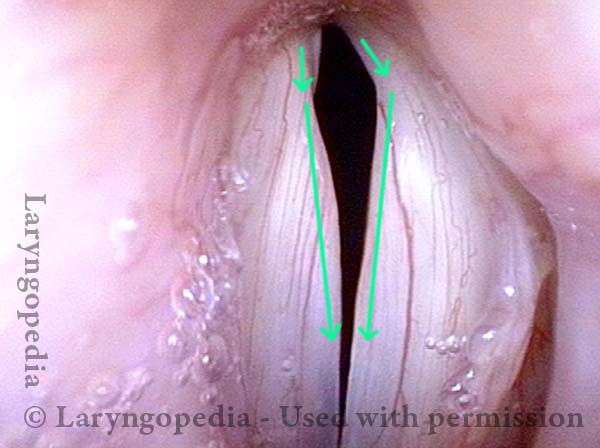
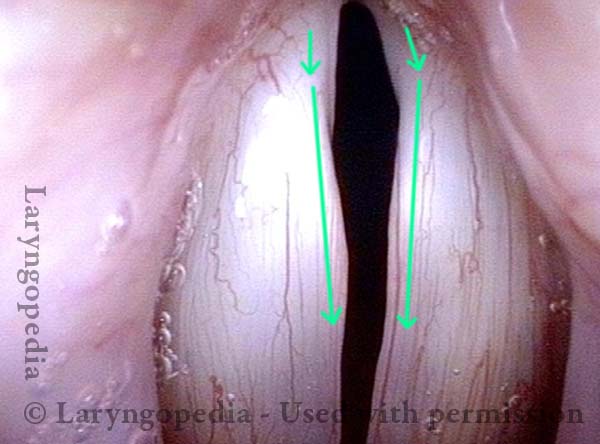
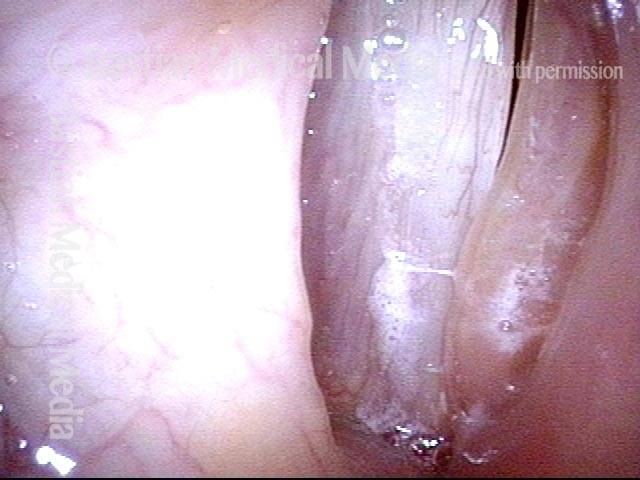
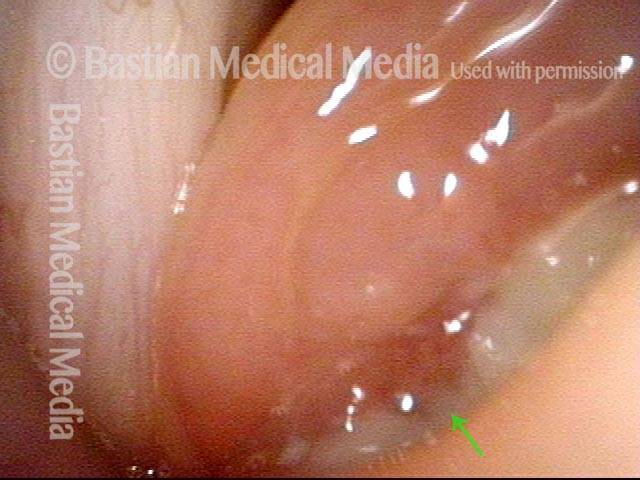
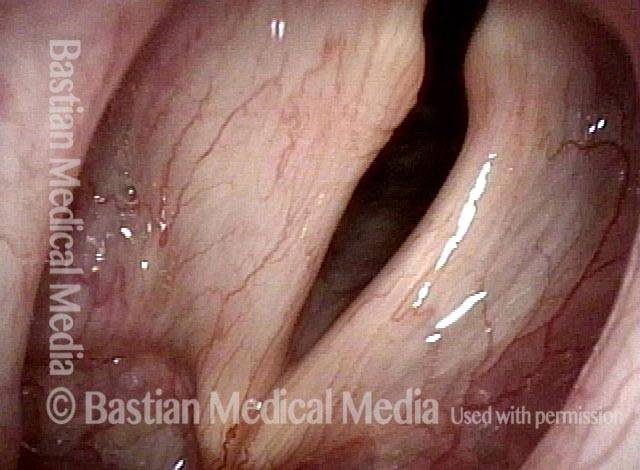
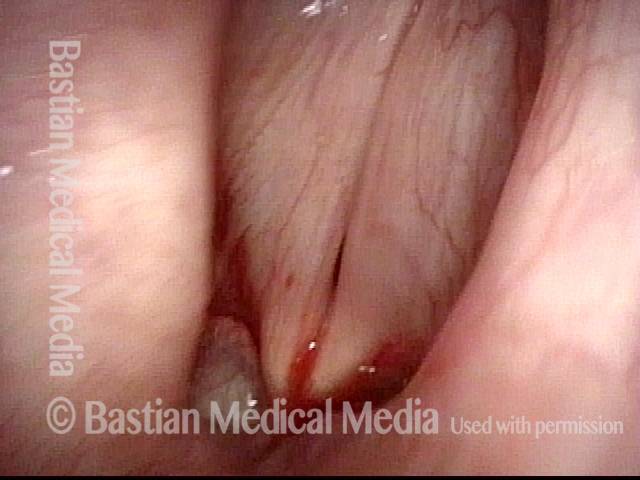
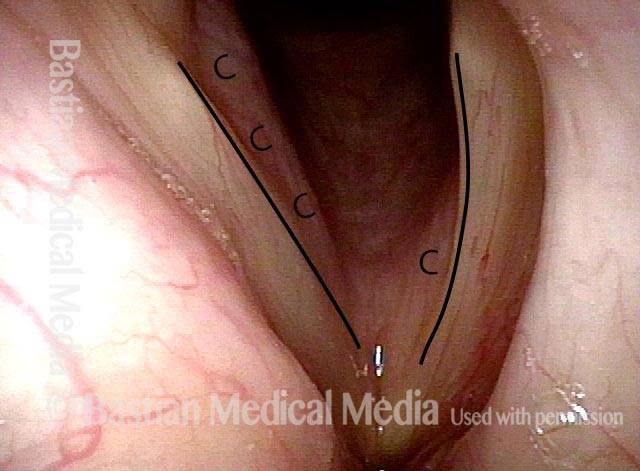
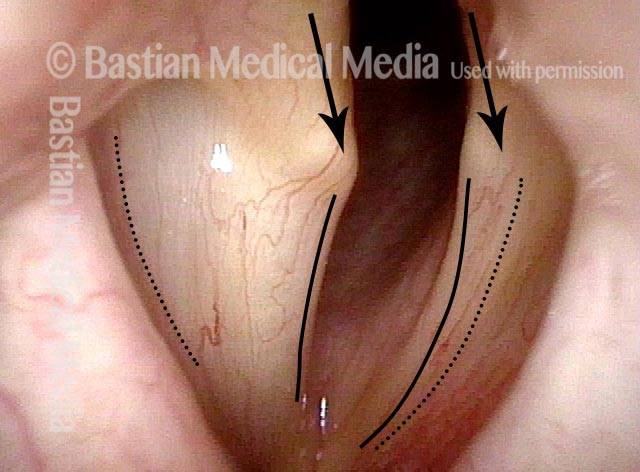
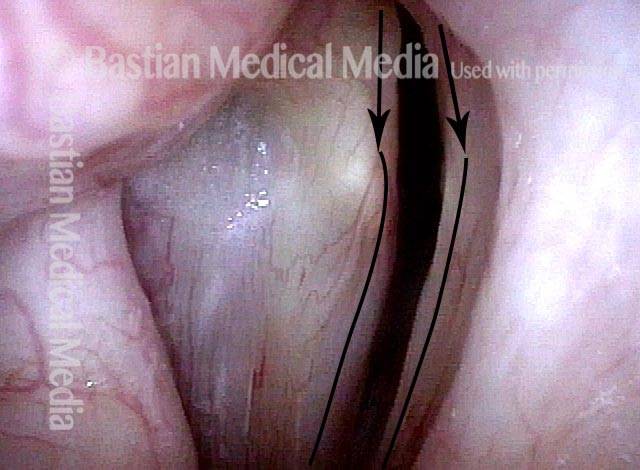
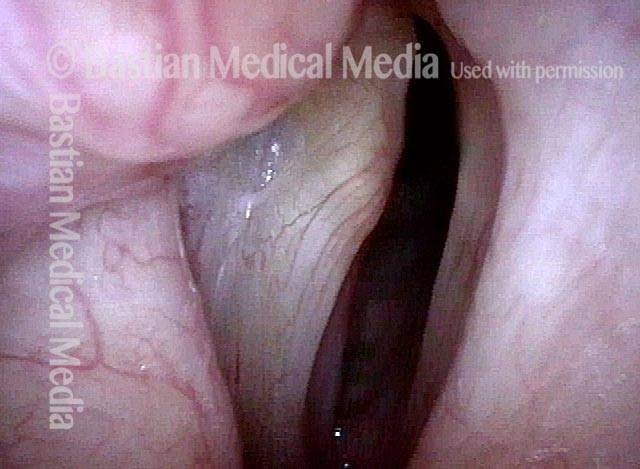
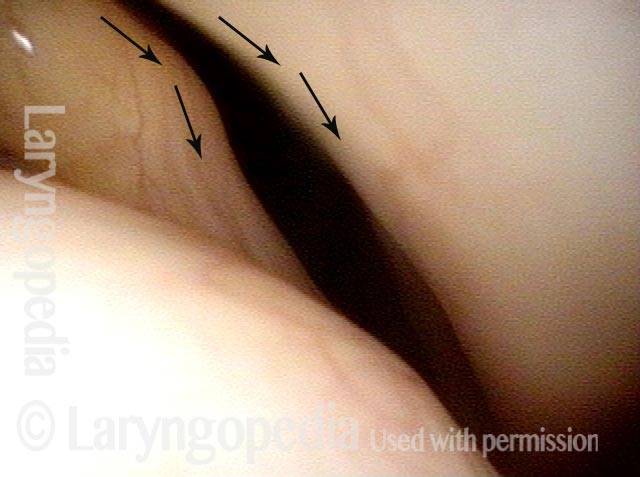
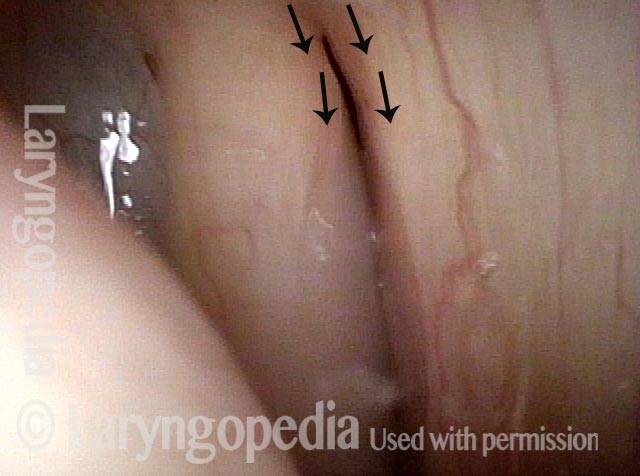
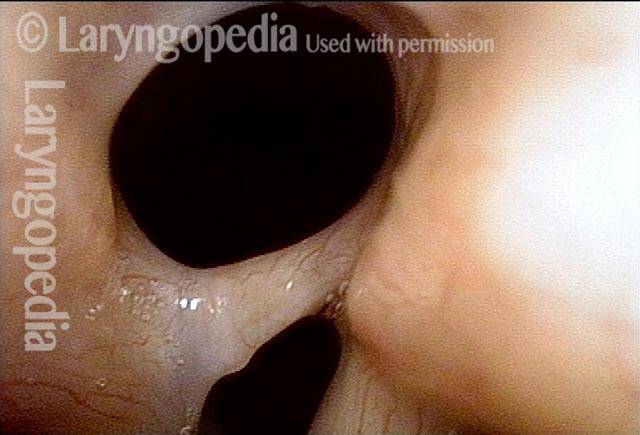
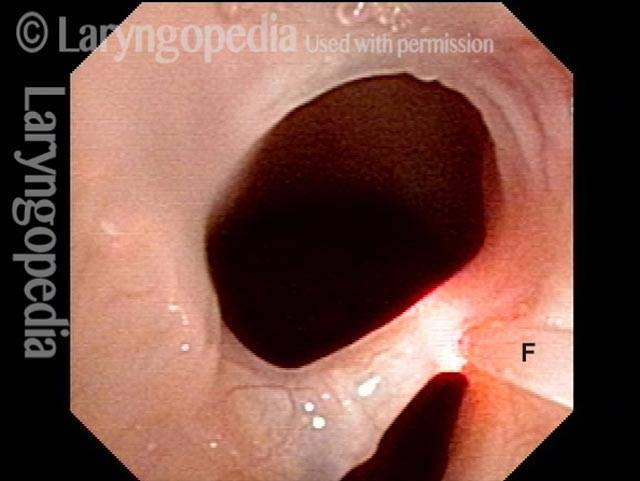
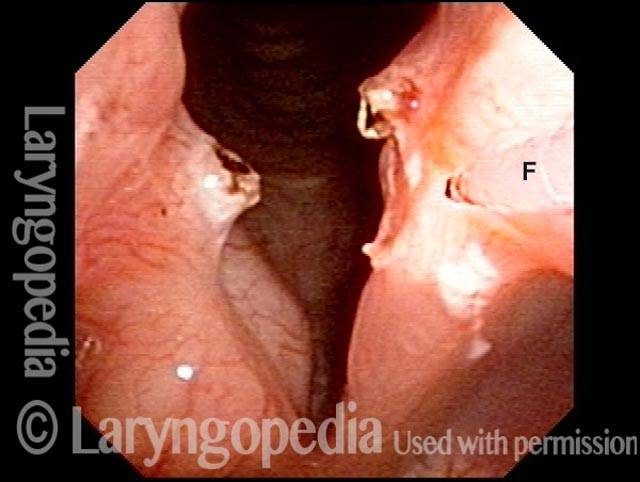
Tornando al termine “paralisi”, si potrebbe definire come la denervazione di tutti e tre i muscoli: PCA, LCA e TA. Questo è chiaramente mostrato nella seguente serie di immagini. Si noti che in genere omettiamo il muscolo interaritenoideo (IA) perché è innervato bilateralmente e non sembra spesso essere presente nella paralisi delle corde vocali.
Paralisi delle Corde Vocali Definita dalla Denervazione di 3 Muscoli Individuali Piuttosto che dalla Mancata Funzionalità del Nervo Ricorrente
La paralisi delle corde vocali è solitamente definita come una corda immobile e il pensiero corre direttamente alla lesione del nervo ricorrente. La “definizione” visiva più universalmente utilizzata è la perdita di abduzione (sebbene vi sia anche una perdita di compressione mediale). In altri termini, tendiamo a pensare che il nervo ricorrente sia “fuori uso”, ma non che i tre muscoli individuali siano denervati di conseguenza. Al contrario, la paresi è definita dalla denervazione di uno (o due) dei seguenti muscoli:
- Cricoaritenoide posteriore (PCA)
- Cricoaritenoide laterale (LCA)
- Tiroaritenoide (TA)
Tornando al termine “paralisi”, si potrebbe definire come la denervazione di tutti e tre i muscoli: PCA, LCA e TA. Questo è chiaramente mostrato nella seguente serie di immagini. Si noti che in genere omettiamo il muscolo interaritenoideo (IA) perché è innervato bilateralmente e non sembra spesso essere presente nella paralisi delle corde vocali.



Evoluzione della Paralisi delle Corde Vocali: Paresi Solo della PCA
Per alcuni foniatri, la misurazione è considerata più importante dell’osservazione. Entrambe sono legittime, ovviamente, tuttavia la comprensione visiva (osservazione) della paralisi e della paresi rimane molto più utile delle misurazioni EMG, acustiche o aerodinamiche. Questo caso illustra chiaramente questo punto.
Questo uomo anziano è stato sottoposto a un intervento chirurgico toracico, ma a causa di complicazioni è stato anche intubato per gran parte di due giorni. Subito dopo il risveglio, la sua voce era alterata. Ha affermato di essere solo sussurrata.
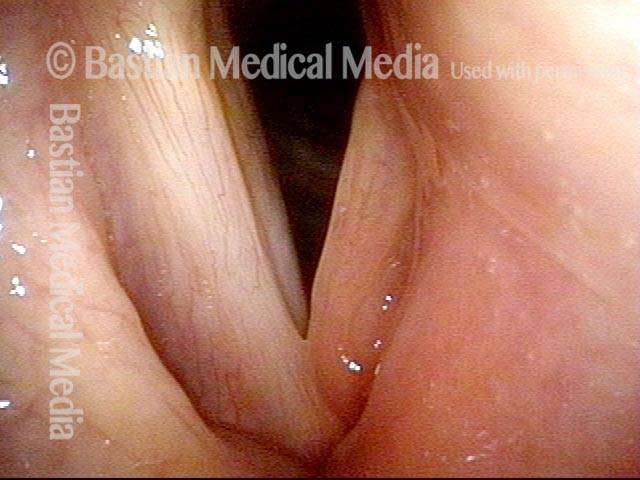
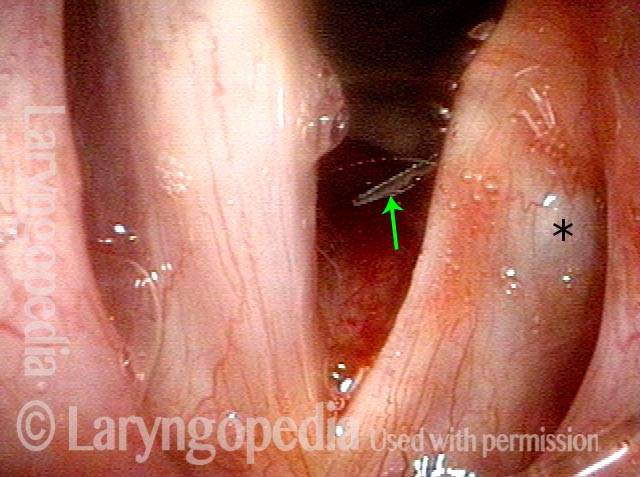
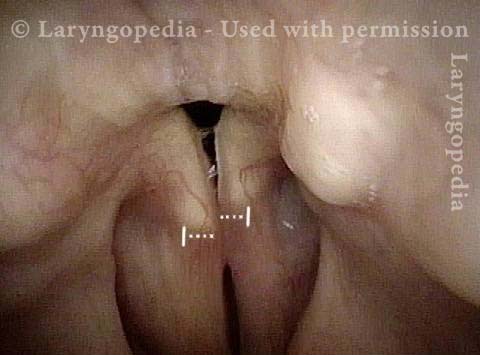
Alla sua prima visita ambulatoriale, un mese dopo, pensava che la sua voce fosse migliorata al “10%” e l’esame ha mostrato una paralisi della corda vocale sinistra (muscoli TA, LCA e PCA tutti non funzionali). Tre mesi dopo, la sua voce era, secondo la sua descrizione, al 40% e migliorava ulteriormente di settimana in settimana. All’ottavo mese post-operatorio, verificato a 18 mesi, riteneva che la sua voce fosse recuperata al “99%”; l’esame ha mostrato il recupero di TA e LCA, ma non del muscolo PCA.
Diagnosi finale: paresi solo della PCA sinistra. Invece di essere completamente "fuori uso", la PCA sembra solo debole.





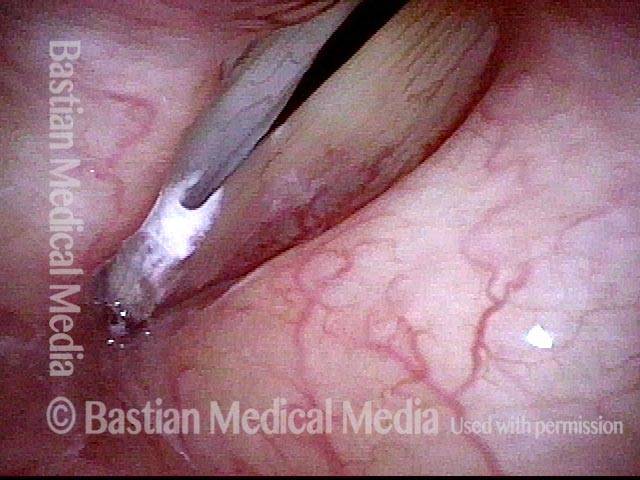
Laringoplastica Iniettiva con gel Temporaneo


Esempi di Paralisi

Esempio 2


Paralisi del Nervo Ricorrente del Ramo Anteriore
Estrusione dell’Impianto della Corda Vocale
Gel Vocale per un Aiuto Immediato


55 Anni di Paralisi con Ogni Scoperta Classica
La Laringoplastica di Medializzazione in Genere non Risolve il “Reperto” dell’LCA


Iniezione di Gel Vocale per la Paralisi delle Corde Vocali


La Discrepanza Aritenoidea che Causa una Qualità della Voce Roca è Difficile da Risolvere in Alcuni Casi di Paralisi delle Corde Vocali




Sinechie della Commissura Posteriore



Quick Fixes to Bring Back Damaged Voices
BVI utilizza procedure come iniezioni di gel per aiutare i pazienti a ripristinare le corde vocali ferite...