Introduction
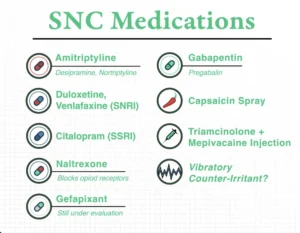
In recent years, a neurogenic form of chronic cough has been described in the literature, referred to variously as “sensory neuropathy presenting as chronic cough”1, “sensory neuropathic cough”2,3, “laryngeal sensory neuropathy”4, or simply “refractory chronic cough”5. It has been shown that sensory neuropathic cough (SNC) can be treated with certain neuralgia medications1,4,5,6,7,8.
What has not yet been described, however, is the use of capsaicin spray as a possible treatment for SNC patients—an approach that may seem counter-intuitive, given that capsaicin is known in the pulmonary medicine literature as a means for provoking coughing for diagnostic or research reasons.
The Genesis of the Idea
In 2005, a desperate patient traveled a considerable distance to consult regarding her terrible intractable cough. She described the typical abrupt, intense tickle at the start of each cough; she also noted the trigger phenomena previously described as a part of SNC2. For many years, she had experienced dozens of coughing episodes per day. Many of her episodes lasted a minute or more and, due to the violence of her attacks, led to public humiliation; she suffered from retching, occasional vomiting, and frequent stress incontinence.
Based upon this history alone, as well as a negative examination, the criteria for a diagnosis of SNC were met.
In addition, she had been previously treated for years for the “usual suspects”—cough-variant asthma, acid reflux, allergy, and post-nasal drip; none of the many medications she had tried for these conditions had helped at all.
Unfortunately, this patient’s case was unusually refractory to our list of SNC medications—in this case, amitriptyline, gabapentin, and oxcarbazepine (later on, she also tried pregabalin). After we managed our customary protocol for each of these medicines by phone across the next few months, we learned together that her cough could be diminished (by as much as 40%), but only if she took high doses of medication, to the point of experiencing unacceptable side effects.
In casting about for additional treatment options, we focused on the fact that her particular stereotyped cough-inducing sensory disturbance was an irresistible tickle at the level of the thyroid cartilage on the left side.
To continue the search for a solution, it seemed logical to infiltrate lidocaine with epinephrine into the area of the left superior laryngeal nerve. Such a nerve block should linger for at least an hour, and since her coughing occurred at least a few times per hour, it seemed that the assessment of benefit, if any, would be easy. After the first injection, the patient reported that she did not cough at all for two days. She was thrilled. Two additional injections were planned in order to validate the benefit of the first injection. Unfortunately, the second injection did not help.
In response to my many questions trying to make sense of the difference between the two injections, the patient commented that the first injection had left her visibly bruised, sore, and somewhat swollen. The second (ineffective) injection did not cause any of these side effects. She in fact requested a third injection that would intentionally make her bruised and sore, as the first one had.
This patient’s story triggered a rapid-fire series of thought experiments: the use of a laser burn as a kind of long-lasting counter-irritant, or the use of extremely powerful mint, or, the use of capsaicin. At that time, capsaicin had been used in topical skin creams to treat various kinds of pain9, and also as an intranasal spray for headaches10.
This patient initially used capsaicin spray obtained for her from a compounding pharmacy, prepared at 0.03% strength. Without any available guidelines, and wanting an answer quickly, I suggested that she use the capsaicin as often as 10 times per day. This gave her heartburn (predictably) and markedly increased her tolerance of hot food. Later, she stepped down to using the capsaicin four times per day. Unfortunately, the capsaicin only helped her cough somewhat. She used it for some time, but then dropped it.
From 2005 to the present, we have tried capsaicin spray in well over a hundred patients. It is typically the fourth approach we try, and only after failure of three different neuralgia medications such as the medications mentioned above, as well as citalopram and desipramine. A small percentage of patients who try capsaicin have experienced major relief. This is why we continue to suggest it as a fourth option.
Possible Kinds of Relief
There appear to be at least three different ways in which capsaicin might relieve an SNC patient’s coughing symptoms. When a patient is supplied his or her first bottle of the spray from us, we explain that we want them to test for the following three potential benefits:
- May reduce the frequency and severity of coughing attacks. At the outset of our use of capsaicin, our theory was that, if this benefit were to occur, it would be as a counter-irritant, as suggested by the patient anecdote above. Subsequently, we thought that this benefit might occur because of desensitization, via gradual depletion of substance P, a neurotransmitter found in the mucosa11. However, more recent information suggests that capsaicin desensitizes primarily through a process called “defunctionalization” of thermal, mechanical, chemical, and other sensory nerve endings12. To test capsaicin’s potential to “defunctionalize” nociceptors, we suggest a trial of at least two weeks, using the spray four times per day. The person is told that use of capsaicin can trigger a bout of coughing, much as asthma inhalers that were prescribed by prior physicians often do, and that they must simply carry on with the capsaicin trial for a minimum of two weeks, even in the face of this obnoxious impediment. A number of patients have obtained relief in this way.
- May act as a counter-irritant to abort or truncate bad attacks. This idea came up because one early patient commented that she was pleased with capsaicin even though her cough frequency was unchanged. She explained that she could tell when an attack was going to be unusually severe and prolonged, often by the “urgency” of the preceding tickle. If she could spray her throat immediately after such an urgent sensation, the attack was shortened. She said that, instead of a typical two-minute duration, the coughing spell might be over in 20 seconds. It is of course impossible to conclude anything from this anecdote, but for what it is worth, other patients have said this works for them, too.
- May serve as a “cough scheduler” by providing temporary relief from coughing after a capsaicin-induced attack. This idea was contributed by a patient who said that, though capsaicin did not help his coughing problem in either of the two ways mentioned above, he was happy with a different benefit he had discovered: if he used the capsaicin to induce an attack of coughing, he would then enjoy an unusually extended period of time without cough. For example, if he were going to see a play, he would spray his throat just before the play started, have a vigorous attack of coughing as a result, but then be able to get to the intermission without coughing. During the intermission, he would again spray his throat (in the bathroom or outside the theater); a second major episode of coughing would occur, but then he could get through the second half of the performance also without coughing.
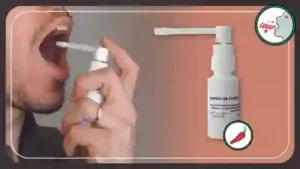
How to Apply the Capsaicin
These are the instructions we give our patients for applying the capsaicin spray:
- Stand in front of your bathroom mirror, open your mouth widely, and try to look as far back into your mouth as possible.
- Depress your tongue so that, if possible, you see the back wall of your throat, and not just your tongue or palate.
- Take a deep breath, hold it in, and aim the capsaicin spray straight back, attempting to hit the back wall of the throat, and not the front of the mouth. Immediately after spraying, exhale and swallow. You will feel the “heat” of the capsaicin for at least 5 minutes.
- Do not eat or drink anything for a minimum of 10 minutes before or after using the spray. This is so that ingested substances do not inadvertently “neutralize” the capsaicin (particularly milk, citrus, salt, etc.).
- Repeat this routine four times a day for a minimum of two weeks (three is better), before deciding whether or not capsaicin is a worthwhile option.
Going Forward
Our sense is that perhaps no more than one in ten patients who try capsaicin after “failing” the usual neuralgia medications (such as amitriptyline, gabapentin, and several others) end up finding capsaicin to be beneficial, in one or more of the three ways described above13. We hope to provide a more formal report of our experience with capsaicin in the near future.
- Lee B, Woo P. Chronic cough as a sign of laryngeal sensory neuropathy: diagnosis and treatment. Ann Otol Rhinol Laryngol. 2005; 114: 253-257. [↩]
- Bastian RW, Vaidya AM, Delsupehe KG. Sensory neuropathic cough: a common and treatable cause of chronic cough. Otolaryngol Head and Neck Surg. 2006; 135(1): 17-21. [↩]
- Gibson PG, Ryan NM. Cough pharmacotherapy: Current and future status. Expert Opin Pharmacother. 2011; 12(11): 1745-1755. [↩]
- Halum SL, Sycamore DL, McRae BR. A new treatment option for laryngeal sensory neuropathy. Laryngoscope. 2009; 119:1844-1847. [↩]
- Ryan NM, Birring SS, Gibson PG. Gabapentin for refractory chronic cough: a randomized, double-blind, placebo-controlled trial. Lancet. 2012; 380(9853): 1583-9. [↩]
- Jeyakumar A, Brickman TM, Haben M. Effectiveness of amitriptyline versus cough suppressants in the treatment of chronic cough resulting from postviral vagal neuropathy. Laryngoscope. 2006; 116: 2108-2112. [↩]
- Van de Kerkhove C, Goeminne PC, Van Bleyenbergh P, Dupont LJ. A cohort description and analysis of the effect of gabapentin on idiopathic cough. Cough. 2012; 8(9). [↩]
- Norris BK, Schweinfurth JM. Management of recurrent laryngeal sensory neuropathic symptoms. Ann Otol Rhinol Laryngol. 2010; 119(3): 188-191. [↩]
- Mason L, Moore A, Derry S, Edwards JE, McQuay HJ. Systematic review of topical capsaicin for the treatment of chronic pain. Br Med J. 2004; 328:991–997. [↩]
- Rapoport AM, Bigal ME, Tepper SJ, Sheftell FD. Intranasal medications for the treatment of migraine and cluster headache. CNS Drugs. 2004; 18(10): 671-85. [↩]
- Burks TF, Buck SH, Miller MS. Mechanisms of depletion of substance P by capsaicin. Fed Proc. 1985; 44(9):2531-4. [↩]
- Anand P, Bley K. Topical capsaicin for pain management: therapeutic potential and mechanisms of action of the new high-concentration capsaicin 8% patch. Br J Anaesth. 2011; 107(4):490-502. [↩]
- Bastian ZJ, Bastian RW. (2015) The use of neuralgia medications to treat sensory neuropathic cough: our experience in a retrospective cohort of thirty-two patients. PeerJ 3:e816 https://peerj.com/articles/816/ [↩]