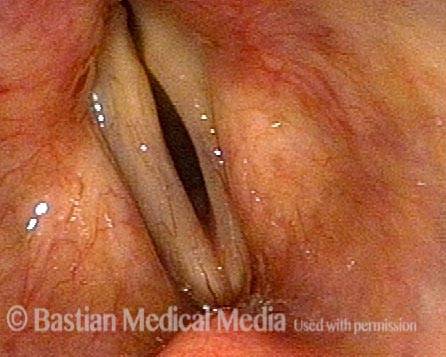
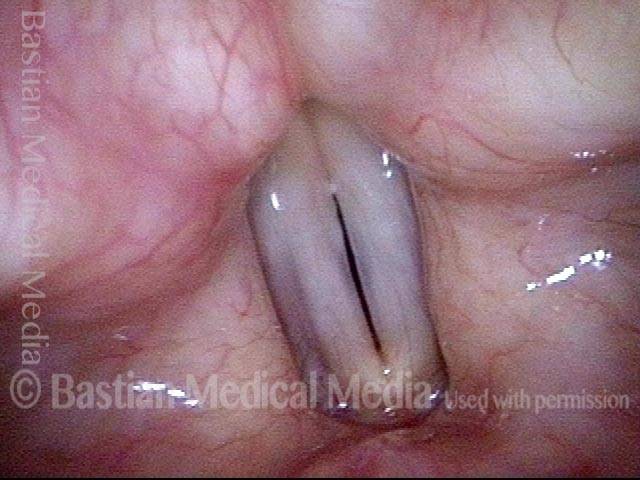
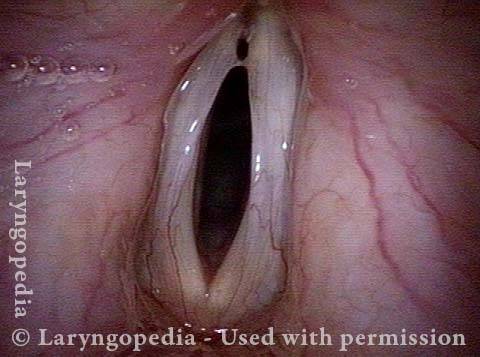
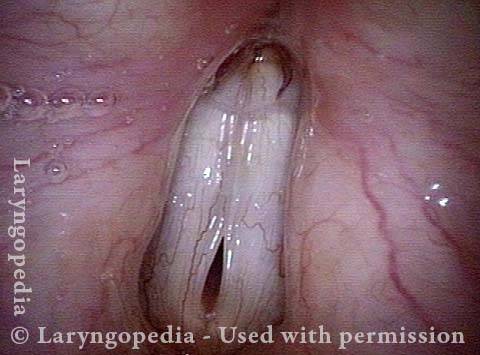
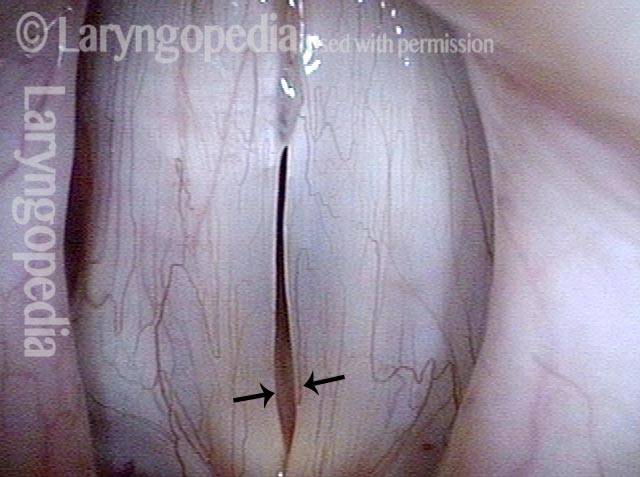
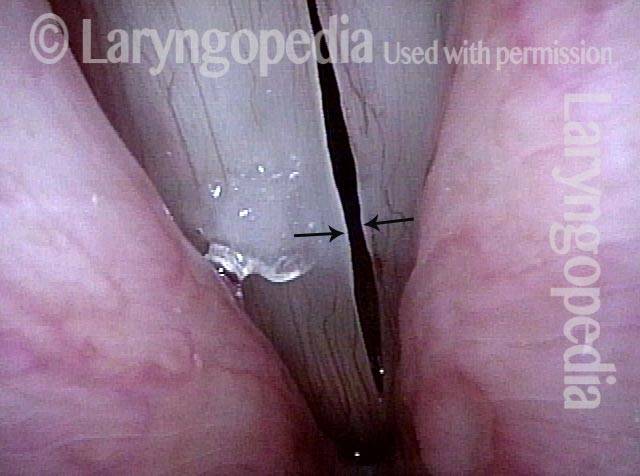
Vocal cord bowing is a descriptive term to specify that the vocal cords are not matching in a straight line, with only a thin dark line between them at the moment of pre-phonation. Instead, the cords become gently concave or bowed outwards. At the moment of pre-phonation, there is a wider, oval slit between the cords.
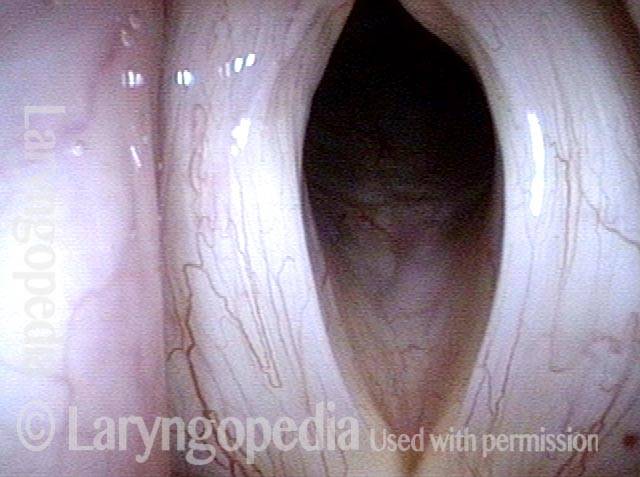
Bowing can be physiologic, asymptomatic, and a genetic “given.” In this physiologic type, the bowing will be subtle to mild and there will be good vibratory pattern. When moderate or severe, bowing may more likely be the result of aging, vocal disuse, Parkinson’s disease, or other conditions.
Moderate and severe bowing correlate with a degree of vocal cord atrophy and the vibratory pattern can be more flaccid. The voice tends to have a soft-edged quality, a little higher in pitch than normal, and can fade with use. Voice building is the primary treatment, but very occasionally severe bowing is treated with bilateral vocal cord implants.
Vocal Cord Bowing
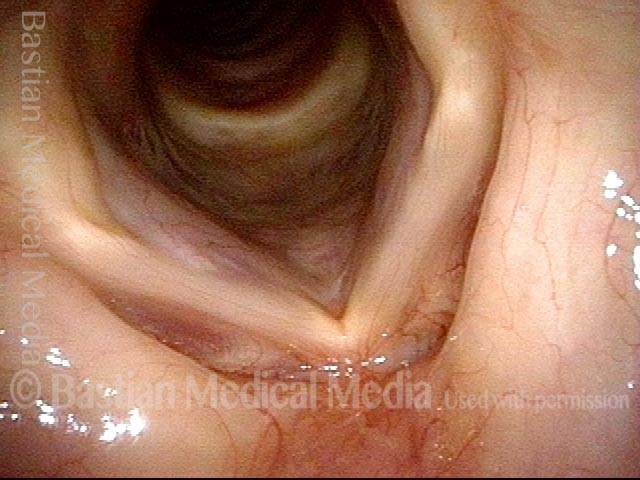
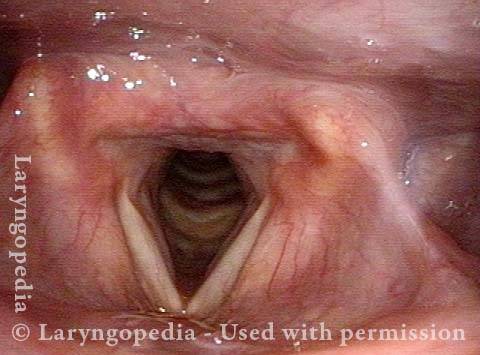
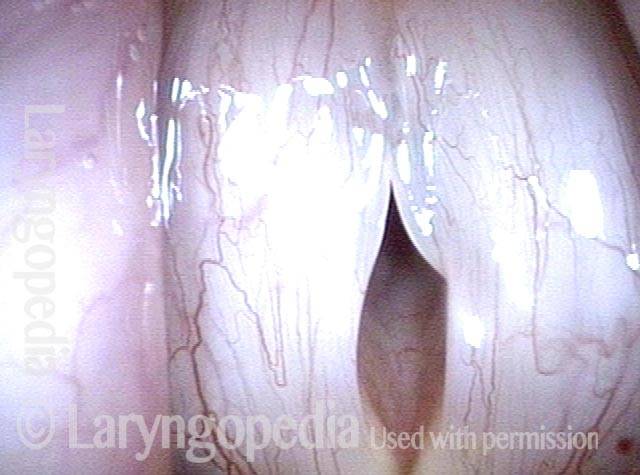
Wide lateral excursions (1 of 4)
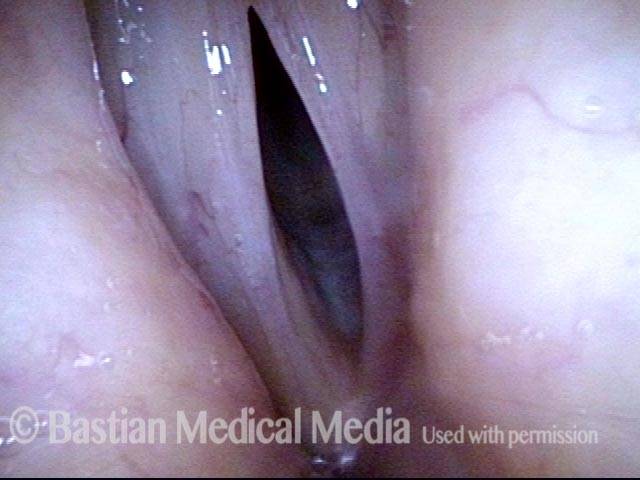
Anterior cords are more flaccid (2 of 4)
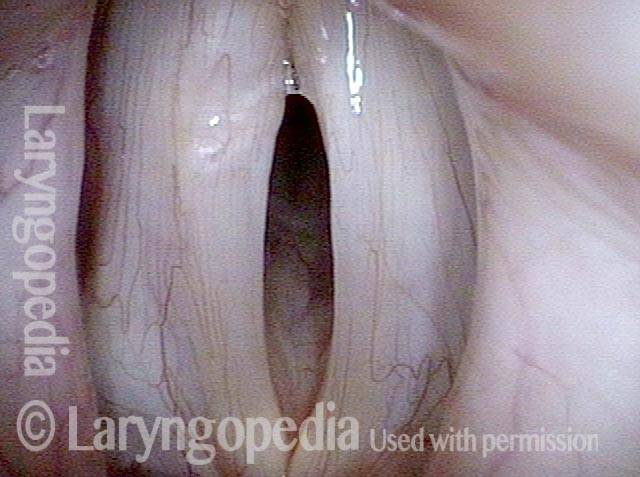
Vocal cord bowing (3 of 4)
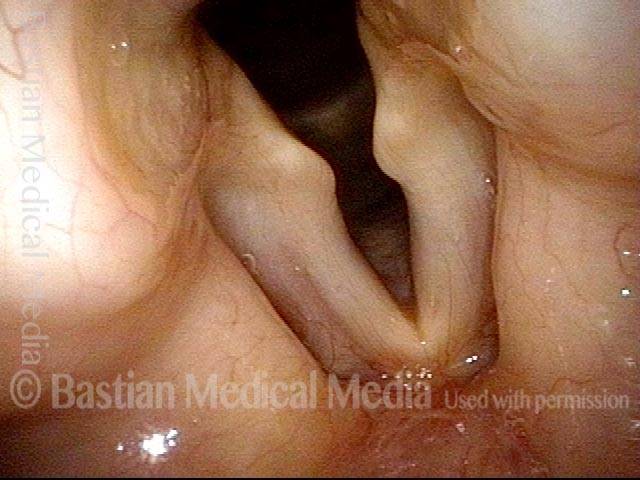
Vocal cord bowing (4 of 4)

Example 2
Glottic gap (1 of 3)

Vibratory blur (2 of 3)

Wide lateral excursion (3 of 3)
Example 3
Vocal cord bowing (1 of 2)
Vocal cord bowing (2 of 2)

Example 4
Vocal cord bowing (1 of 4)

Vocal cord bowing (2 of 4)
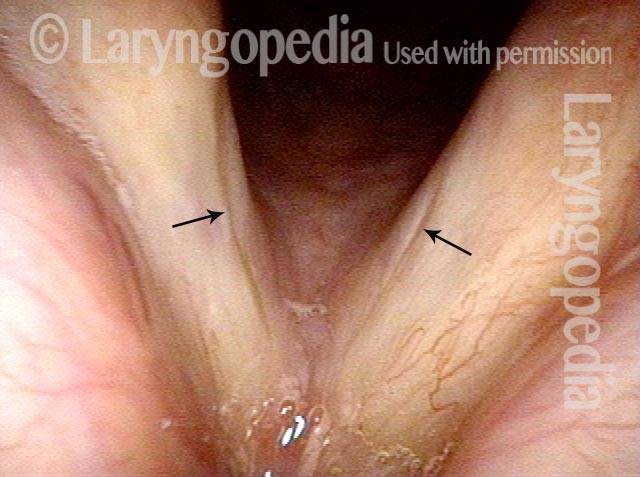
Cords do not close (3 of 4)

Vocal cords only come in near contact (4 of 4)

Example 5
Oval gap during prephonatory instant (1 of 4)

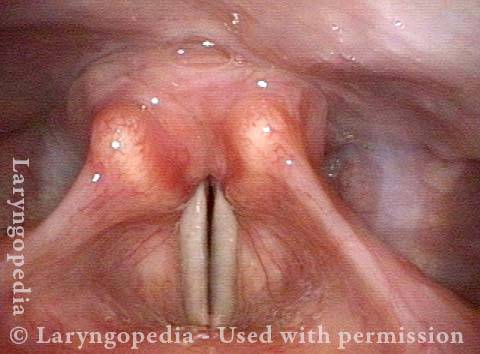
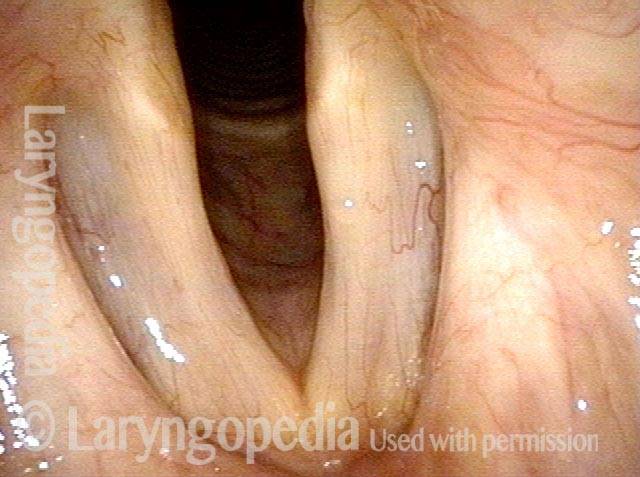
Vocal cord bowing (2 of 4)

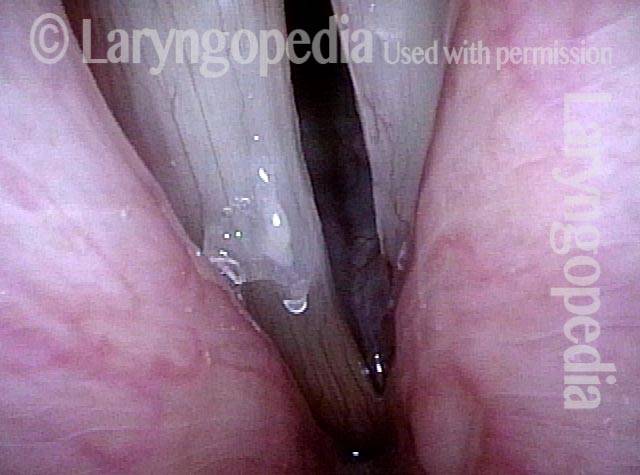
Anterior flaccidity (3 of 4)

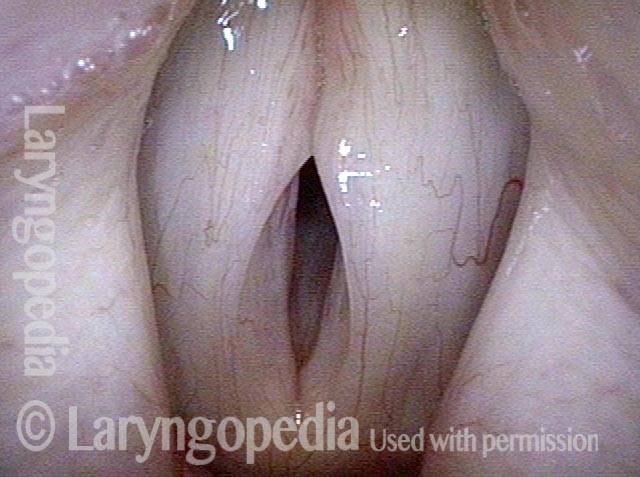
Vocal cord bowing (4 of 4)

Example 6
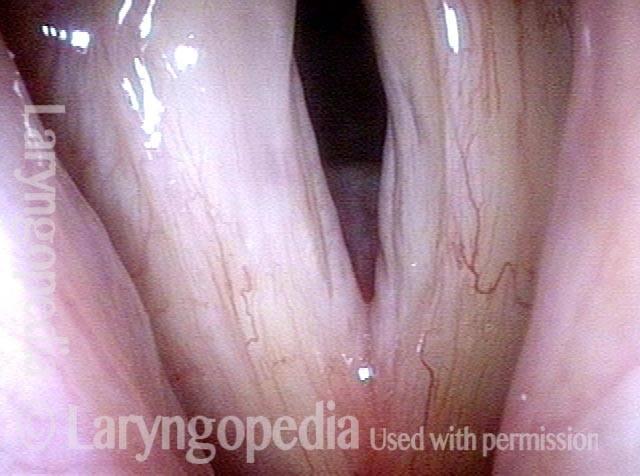
Vocal cord bowing (1 of 5)
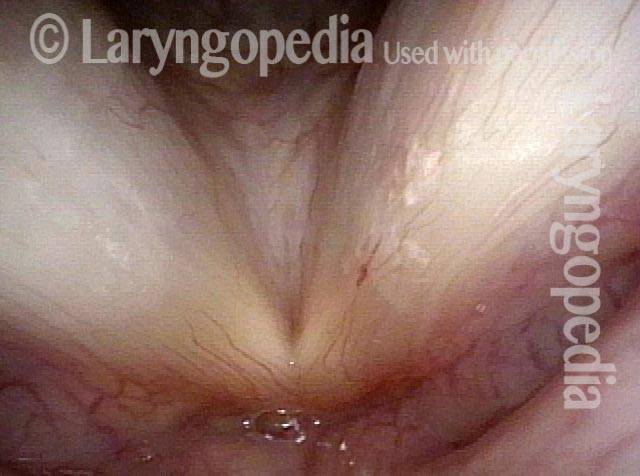
Musculomembranous are bowing (2 of 5)
Elliptical gap (3 of 5)

Vocal cord bowing (4 of 5)

Vocal cord bowing (5 of 5)
A key visual finding of vocal cord flaccidity
This seventy-something woman has noted a weak voice for at least a decade. She came for evaluation due to what seemed like further reduction of strength following a bout of laryngitis.
At her evaluation, her faintly fuzzy speaking voice can “pass for normal for age” but when asked to project, her voice manifests a lack of edge and power. At low pitch there is one moment of “luffing.” From her history and vocal phenomenology, vocal cord bowing is suspected.
Vocal cords (1 of 4)
Vocal cords phonating (2 of 4)
Large amplitude of vibration (3 of 4)
Vocal cord flaccidity (4 of 4)
Bowing of vocal cords and effect of pitch
Weak voice (1 of 8)

Phonatory view (2 of 8)

“Closed” phase (4 of 8)
B3, open phase (5 of 8)
D3, open phase (3 of 8)
B3, closed phase (6 of 8)
Bb4, open phase (7 of 8)

Bb4, closed phase (8 of 8)

Four views of vocal cord bowing in the same person
Bowed vocal cords (1 of 8)
Prephonatory view (2 of 8)

Open phase (3 of 8)

Gravel voice (4 of 8)

Reduced flaccidity (5 of 8)
Closed phase (6 of 8)

Falsetto, open phase (7 of 8)

Falsetto, closed phase (8 of 8)

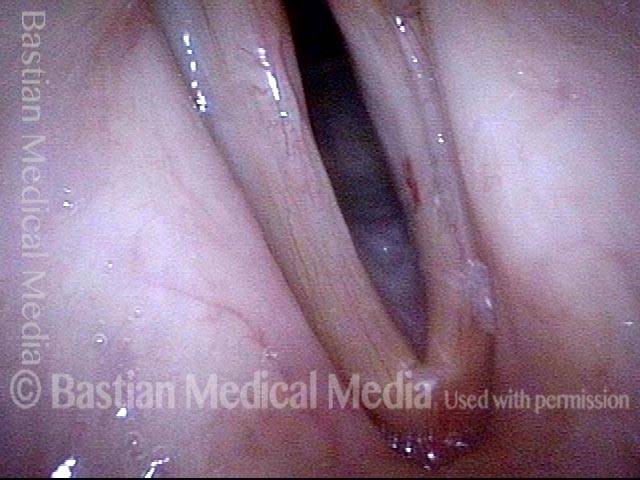
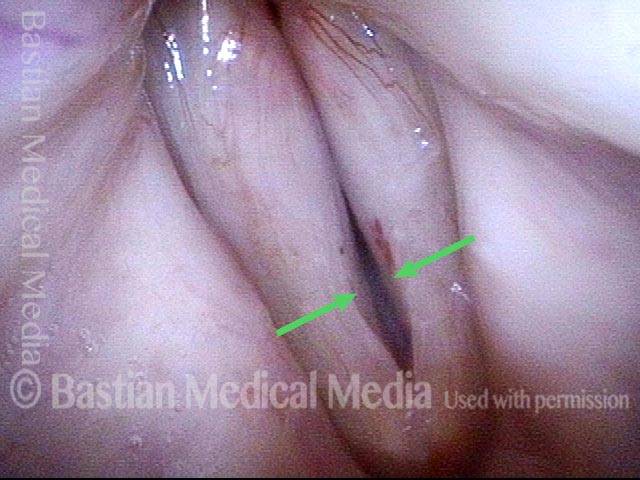
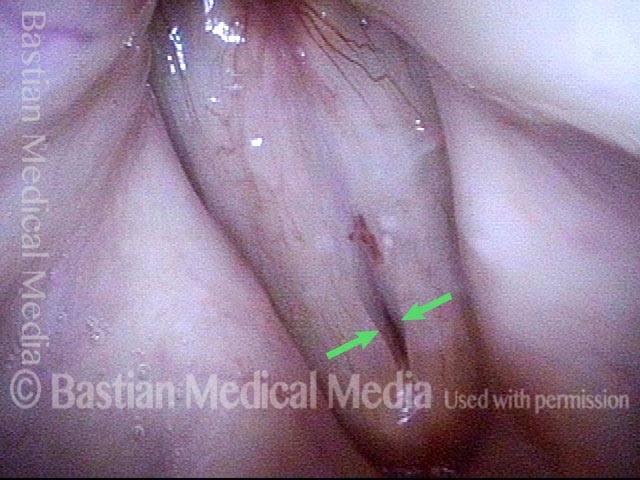
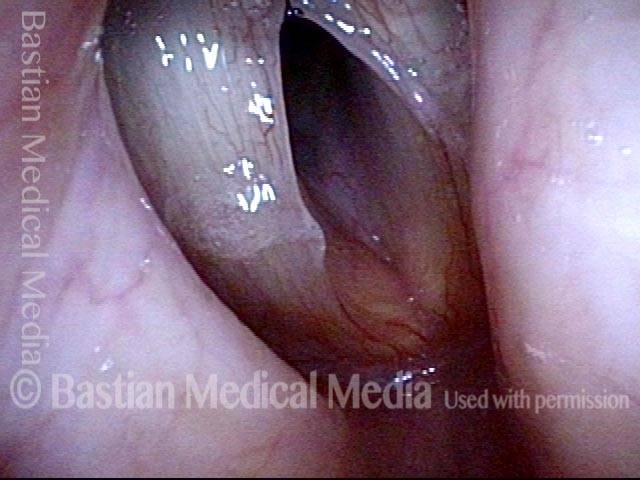
Red herring capillary ectasia and mucosal injuries
Ectatic capillary (1 of 4)
Ectatic capillary, narrow band light (2 of 4)

Margin swelling (3 of 4)
Bowing, atrophy, and flaccidity (4 of 4)
Glottic furrow—not just bowing and not glottic sulcus
Bowing vocal cords with furrows (1 of 4)
Closed phase (2 of 4)

Open phase (3 of 4)
Lower pitch reveals furrow (4 of 4)
