Cricopharyngeus Spasm and What to Do About It
Tell me more about the cricopharyngeus muscle. Where is it, and what is it for?
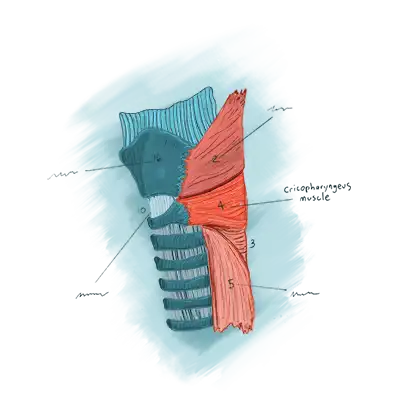
It is a sphincter, which is a circular muscle that makes a ring around the uppermost part of the esophagus to serve as a “valve” or “gateway” between the throat and esophagus. In the gastrointestinal tract, there is a series of additional sphincters: between lower esophagus and stomach; at the outlet of stomach into small intestine, and so forth down to the anus. Each of these sphincter muscles “at rest” is in a contracted state. When “in use,” each sphincter is momentarily relaxed.
When we swallow, the cricopharyngeus muscle sphincter must relax for a brief moment to let food or liquid out of the throat, through the sphincter, and into the upper esophagus. (It also relaxes momentarily, by the way, to release air from below upwards when we belch.) Normally we are unaware of this sphincter muscle because it functions outside of our consciousness.
You’ve used the word “spasm” as the cause of the sensation, but can you clarify what you mean?
By use of the word spasm, we don’t mean a cramp or a charley horse. It is instead sustained hypertonicity of the upper esophageal sphincter, or cricopharyngeus muscle. It is over-contracted. That’s why we become aware of it when this overcontraction gives rise to a feeling of pressure, choking, etc. defined as cricopharyngeus spasm.
By analogy, we are normally unaware of neck muscles that we use to hold up our heads. Yet, we have all had the experience of tight posterior neck muscles that we find to be bothersome and to intrude sufficiently into quality of life that we might ask a friend “Can you rub my neck?” In similar fashion, cricopharyngeus spasm often intrudes into a person’s mental space, and becomes oppressive, but there seems to be no way to relieve the sensation. Not only that, but the sensation causes us to worry, partly because many people with this problem search in vain to find someone to explain this to them, and they are therefore unable to put aside their worry about the sensation.
{kind=link}
{kind=link}
What is the list of features or symptoms that constitute the syndrome of cricopharyngeus spasm?
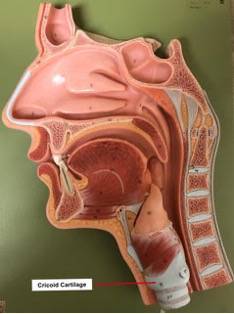
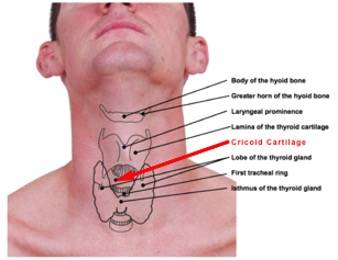
- Location of the sensation is at the level of the cricoid cartilage in the mid-to low neck.
- The nature of sensation is often described with words like choking, pressure, constriction, swelling…. Or, “It feels like a wad of phlegm.” One other particularly common description is “It feels like there is something stuck in my throat that I can’t swallow and can’t spit out.” Many say that this sensation is oppressive and preoccupying.
- The magnitude of the sensation tends to vary. Most often, it tends to become worse as the day progresses. A person might also notice that symptoms increase when they are stressed or fatigued, whatever the time of day.
- Active eating provides transient relief of the sensation. While the discomfort seems to originate in the swallowing passage, there is no interference with actual travel of food or drink.That is, the person’s ability to swallow food and liquids is fine. And in fact, during active eating,such as at lunch or dinner, the sensation subsides or even goes away completely, only to begin to return soon after finishing that meal.
Why does eating reduce the symptoms?
A person can’t rub the tight muscle directly, but each time a swallow happens, the sphincter muscle must let go momentarily, as already mentioned. This is then a kind of therapy to the over-contracted, hypertonic muscle. Swallowing saliva doesn’t help, because the volume we swallow is small, and the swallows are widely spaced in time. Active eating of a sandwich or plate of food during a mealtime, by contrast, relaxes the sphincter fully every 10 to 20 seconds across a span of 15 minutes or more. To repeat, this serves as a kind of unplanned “therapy” of the muscle and the symptoms subside for a time.
Is Cricopharyngeal Spasm Dangerous?
The problem is that the cricopharyngeus muscle is overly contracted when in its state of habitual contraction. This hyper-contraction or hyper-tonic state may be felt by the person. However, the muscle will still relax properly during swallowing, and thus does not impede swallowing.
What can be done?
There is an old saying by Alexander Pope: “To know ourselves diseased is half our cure.” This seems to apply here as many patients say that simply coming to understand the disorder, as described above, is a major step towards relief. One woman said: “When I understood what was wrong, and that I didn’t have to worry about cancer, the problem started to gradually go away across the next several weeks.”
For this to happen, however, the patient must accept and really believe in their diagnosis. Doctors can help them feel secure by making the diagnosis partially through what we call a “mind reading” exercise. It works like this: Right after the person says “Doctor, there is a lump…..”, we gently stop him or her, and ask if we can try to “read their mind.” The idea is that at the end of the “mind reading”, the patient is invited to say, “That’s it exactly!” Or, “That is mostly it but you said _________ and I would say __________.” Or, the patient might say “That isn’t at all what I am experiencing” and in this third case, attention is turned to a different diagnosis. If the physician does successfully “read the patient’s mind,” describing patient symptoms exactly, the patient finds it easier to accept and believe in the diagnosis because of the “mind-reading” involved.
Keep in mind that there really isn’t an examination finding, blood test, or X-ray to make the diagnosis for cricopharyngeus spasm. It is based in the precise 4-part syndrome described above.
Many such patients report that they can now “throw the sensation over their shoulders.” In other words, if particularly symptomatic, they can more easily say to themselves: “That crazy muscle….” It is a little like ignoring the sensation of new glasses, or contact lenses. And as mentioned, many say that knowing and trusting the diagnosis all by itself is the beginning of slow, steady, reduction and eventual disappearance of the symptoms across a few weeks’ time.
What if I want to do more than just “know myself diseased”? Isn’t there anything medical the doctor can do?
The occasional patient asks this and our list of further options includes:
- Work with a physical therapist or speech pathologist. The focus of that work is anterior neck relaxation, possibly by use of surface biofeedback electrodes, yawning maneuvers or very gentlestrap muscle massage (carefully avoiding going anywhere near the vascular compartments of theneck/ carotid arteries!!)
- A confirmatory “diagnostic” test in the form of a muscle relaxant, such as valium. That medication, called a benzodiazepine, has a tranquilizer effect, but we actually wish we could take it out of the medication. For our purposes, it is only the muscle relaxant property that we want. But they of course come together…. So here is how to do the diagnostic trial:
- We provide a prescription for four tablets of 5 mg each. These four tablets each represent a “diagnostic test.”
- Get into your pajamas about 2 hours before your normal bedtime on an evening when you are not planning to go out, and when you are also more than averagely symptomatic. Now take a moment to “commune” with your CPS sensation. “Measure” it on a 10-point scale, for example. (Suppose you choose “6.”) Notify family that you are about to do your first diagnostic test of CPS. You can also set a loud timer for 90 minutes.
- Now, take Valium tablet #1.
- 90 minutes later, commune with/measure for a second time the level of the sensation. It is usually not gone altogether, but noticeably diminished. 25% to 75% reduction would be what people commonly report. So on this particular evening, you might notice that “6” has become “2” or “3.” Again, this is the result of the direct muscle relaxant properties of Valium.
- If you fall asleep on the couch and waken in the middle of the night, you have three more opportunities to do the diagnostic test in coming days or weeks.
- Rarely, a person can have the muscle injected with botulinum toxin. This is in the extreme casewhere the person isn’t worried about the diagnosis, but is simply plagued by the sensation itself. Of hundreds of persons we have diagnosed with this disorder, we have done this in a single patient, who achieved great benefit for the duration of botulinum toxin effect, approximately 4 months.
Conclusion
In summary, cricopharyngeus spasm occurs when hypertonicity in a circular, “valve” muscle mid- to low neck causes the sensation of a lump or choking, etc. It is a benign condition but especially while it remains undiagnosed, it can cause great distress and worry.