What is the list of features or symptoms that constitute the syndrome of cricopharyngeus spasm?
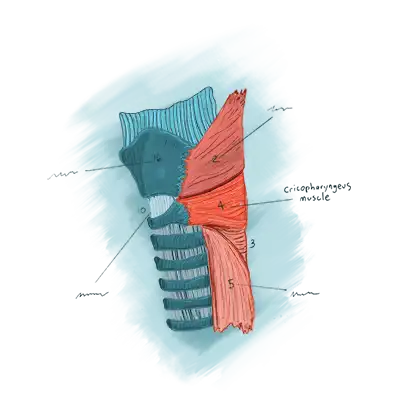
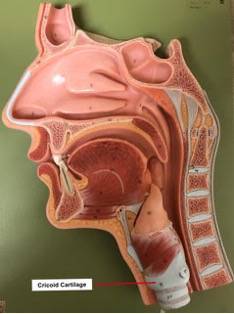
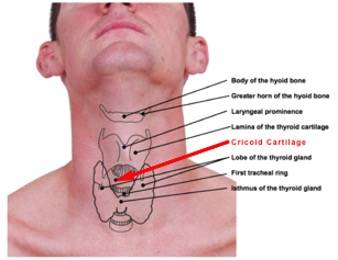
- Location of the sensation is at the level of the cricoid cartilage in the mid-to low neck.
- The nature of sensation is often described with words like choking, pressure, constriction, swelling…. Or, “It feels like a wad of phlegm.” One other particularly common description is “It feels like there is something stuck in my throat that I can’t swallow and can’t spit out.” Many say that this sensation is oppressive and preoccupying.
 The magnitude of the sensation tends to vary. Most often, it tends to become worse as the day progresses. A person might also notice that symptoms increase when they are stressed or fatigued, whatever the time of day.
The magnitude of the sensation tends to vary. Most often, it tends to become worse as the day progresses. A person might also notice that symptoms increase when they are stressed or fatigued, whatever the time of day.- Active eating provides transient relief of the sensation. While the discomfort seems to originate in the swallowing passage, there is no interference with actual travel of food or drink.That is, the person’s ability to swallow food and liquids is fine. And in fact, during active eating,such as at lunch or dinner, the sensation subsides or even goes away completely, only to begin to return soon after finishing that meal.
Why does eating reduce the symptoms?
A person can’t rub the tight muscle directly, but each time a swallow happens, the sphincter muscle must let go momentarily, as already mentioned. This is then a kind of therapy to the over-contracted, hypertonic muscle. Swallowing saliva doesn’t help, because the volume we swallow is small, and the swallows are widely spaced in time. Active eating of a sandwich or plate of food during a mealtime, by contrast, relaxes the sphincter fully every 10 to 20 seconds across a span of 15 minutes or more. To repeat, this serves as a kind of unplanned “therapy” of the muscle and the symptoms subside for a time.