Síntomas y riesgos de la papilomatosis respiratoria recurrente
La RRP puede poner en peligro la vida de los niños pequeños, si no se sigue y trata cuidadosamente, ya que las vías respiratorias de un niño son relativamente estrechas y pueden obstruirse completamente por los crecimientos proliferativos de la enfermedad; además, la PRR en niños tiende a crecer y reaparecer de forma más agresiva. En los adultos, la RRP generalmente solo afectará la función de la voz (cuando los crecimientos ocurren en las cuerdas vocales), aunque también puede afectar la respiración en casos graves. Ocasionalmente, la RRP también puede progresar a cáncer y, por lo tanto, los pacientes que se encuentran en alto riesgo de padecer esto (ver a continuación) deben ser monitoreados cuidadosamente.Características de los crecimientos.
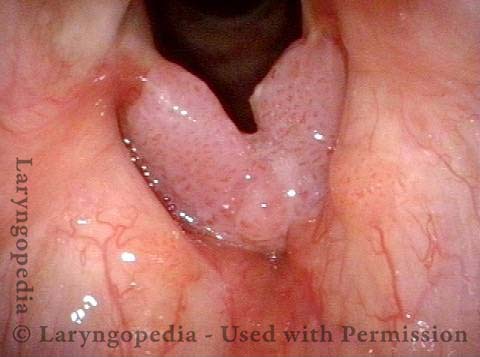
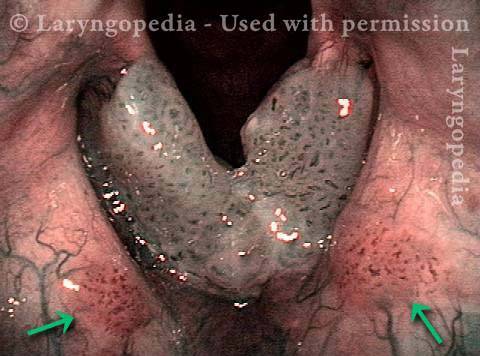
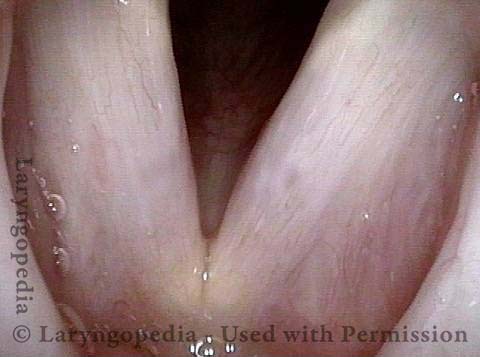
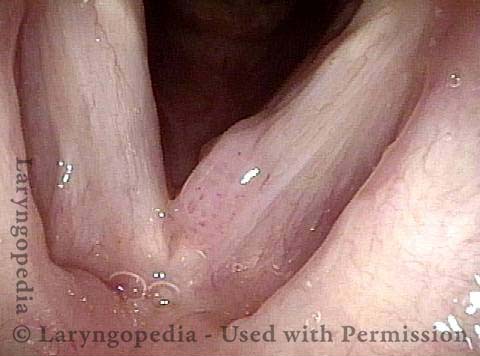
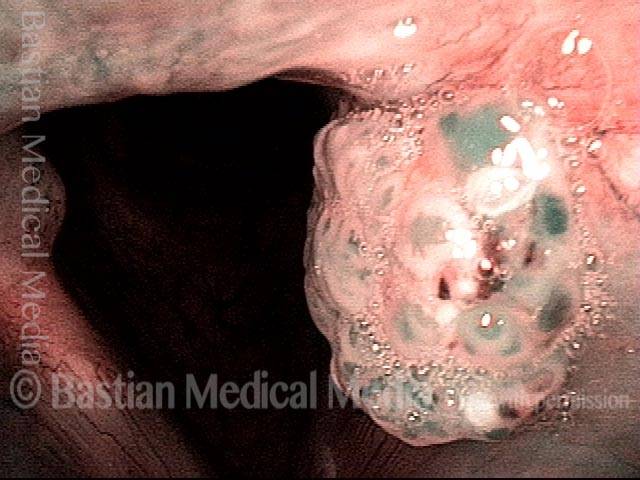
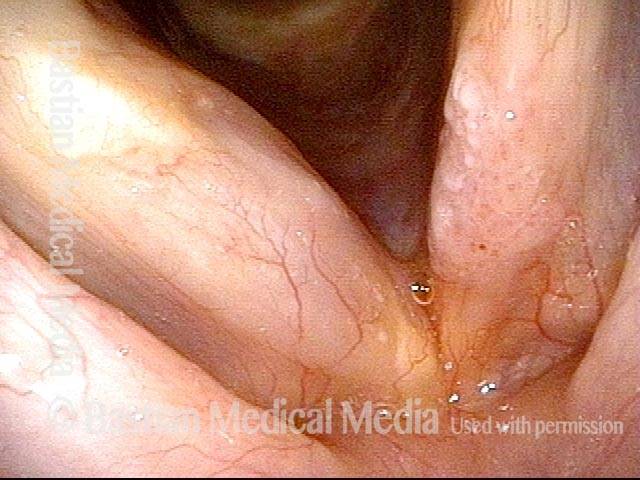
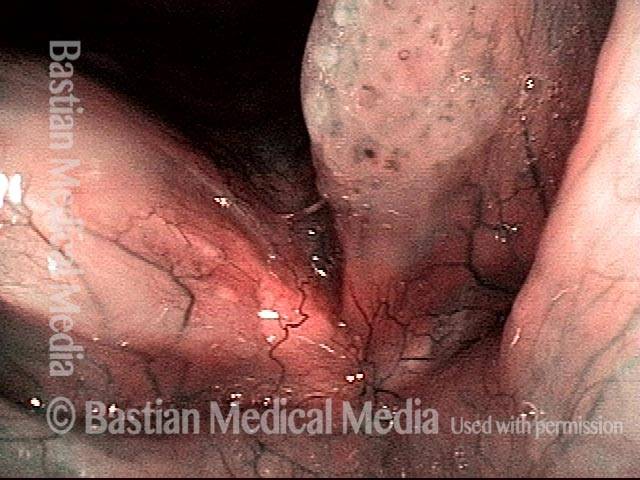
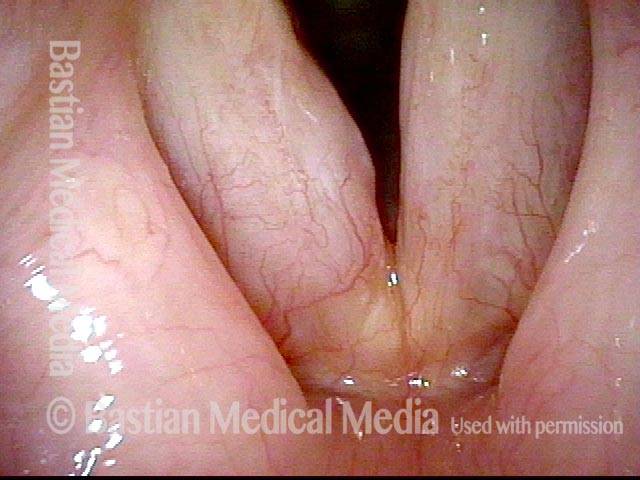
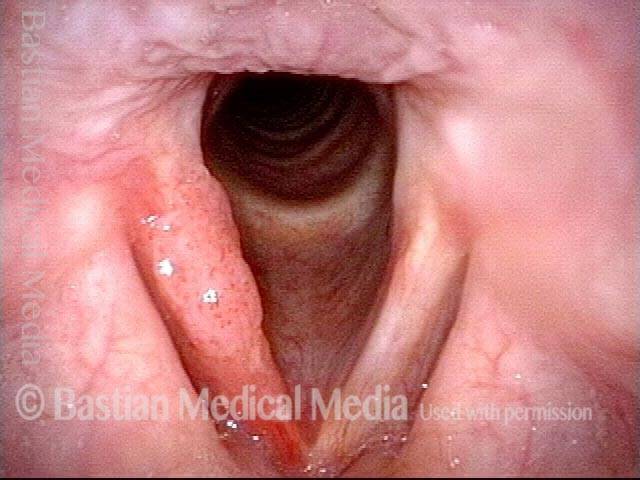
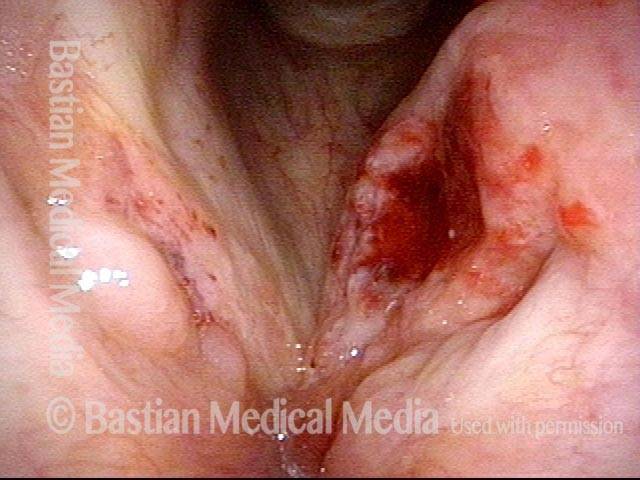
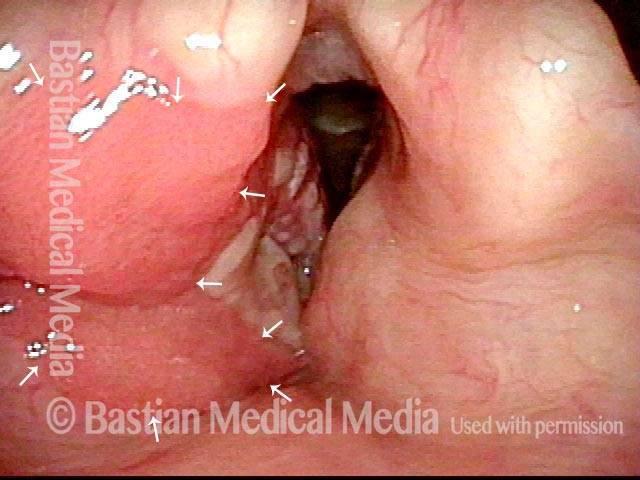
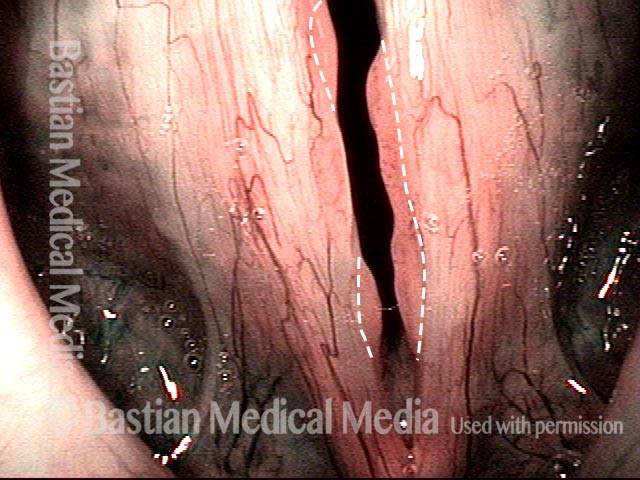
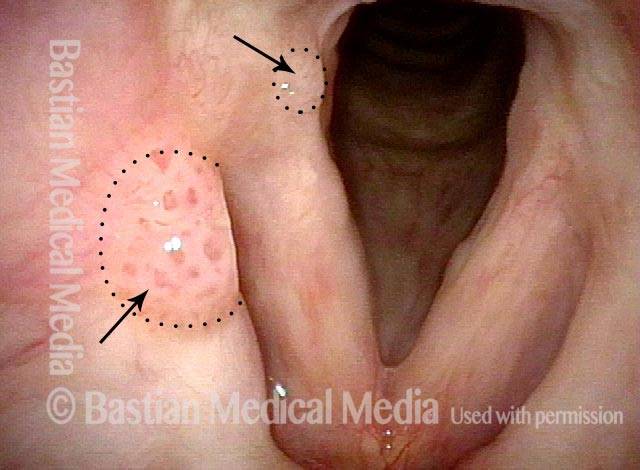
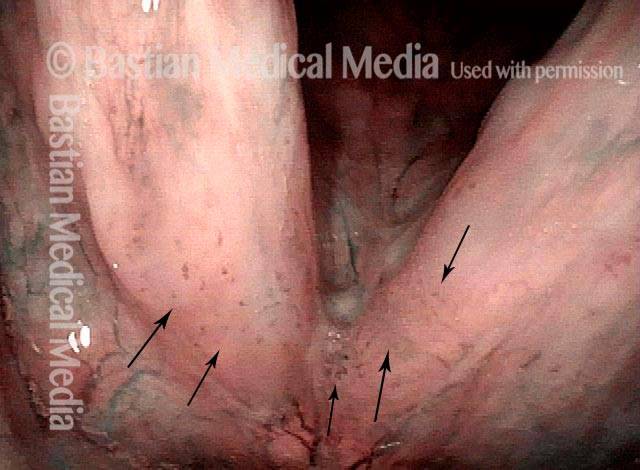
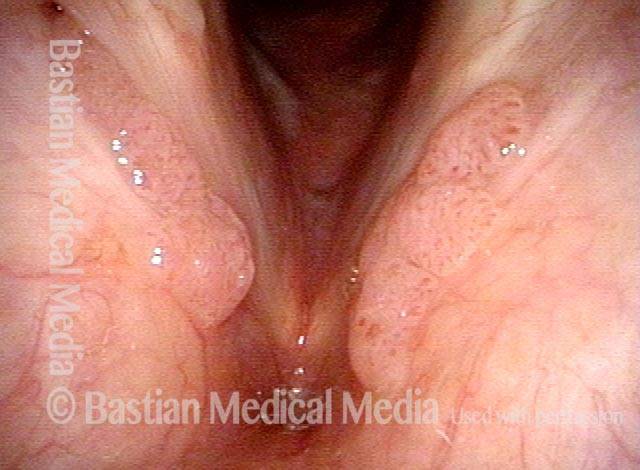
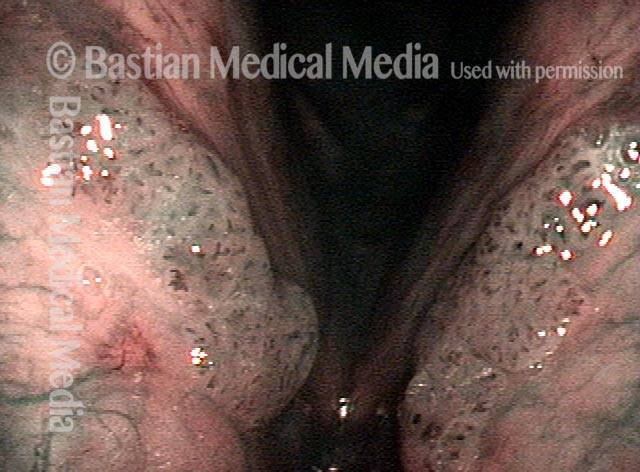
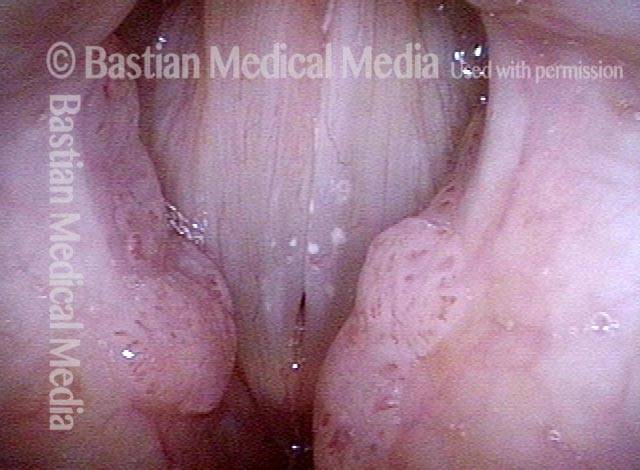
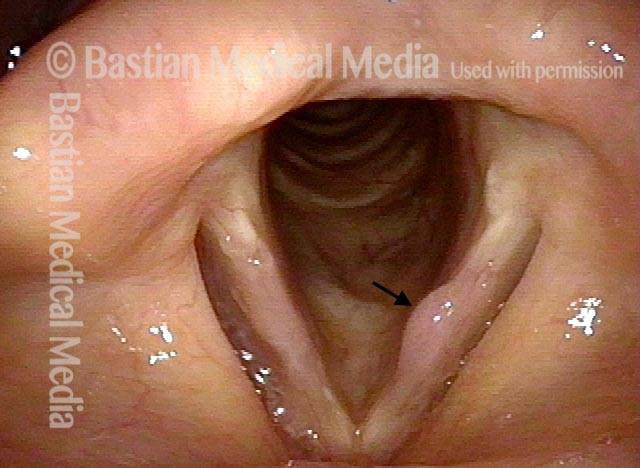
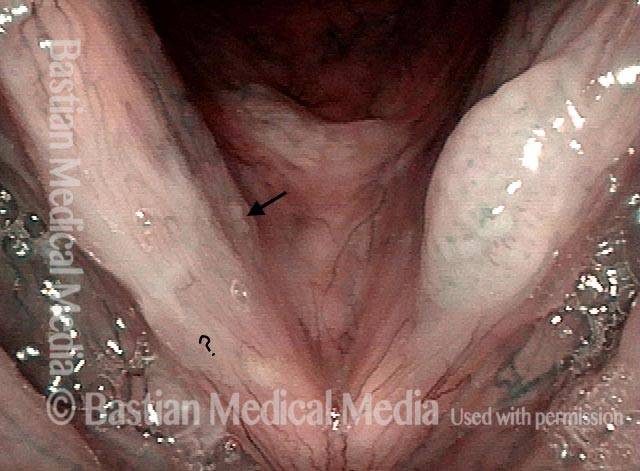
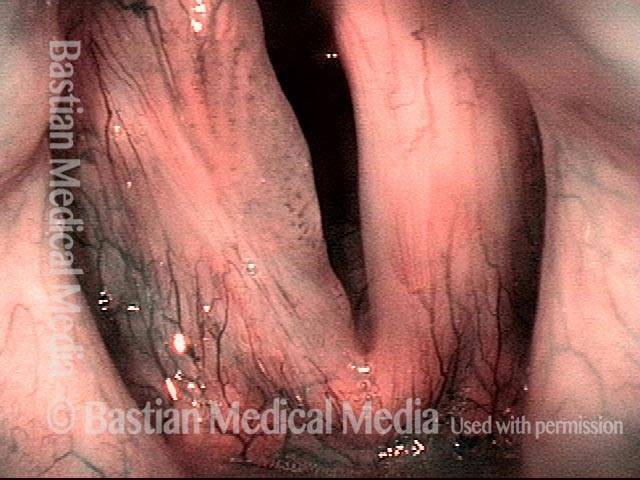
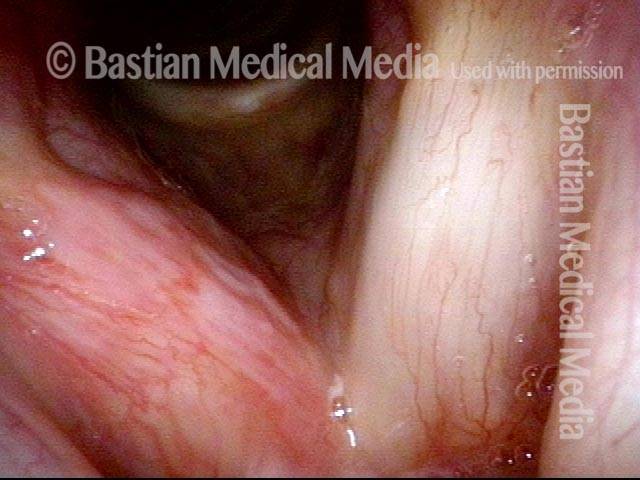
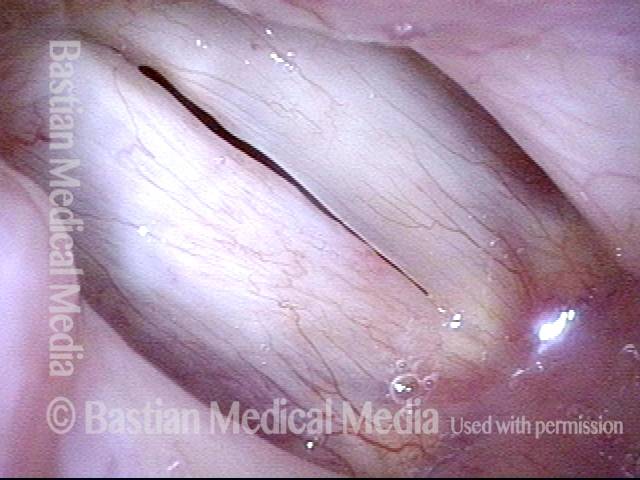
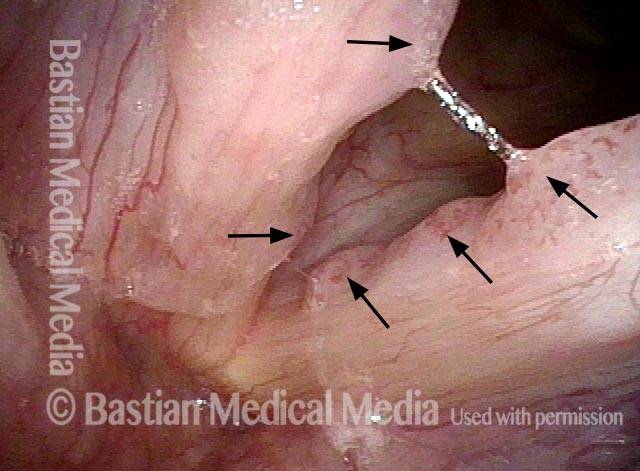
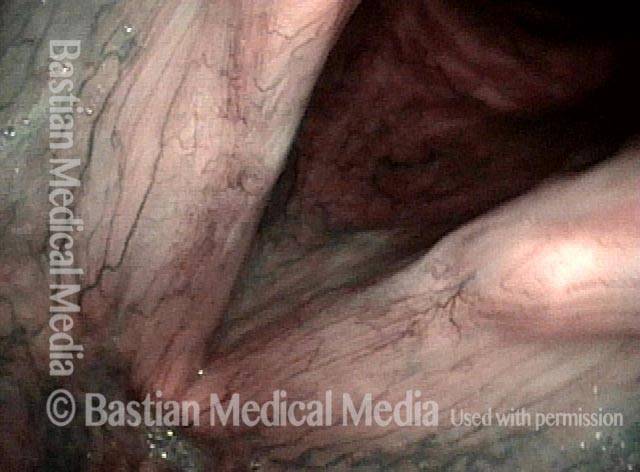
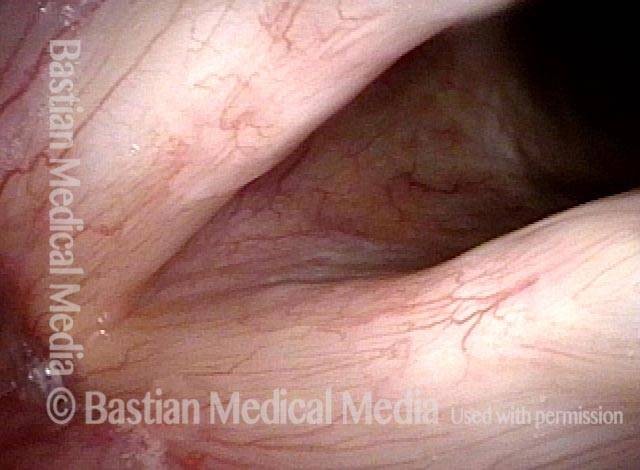
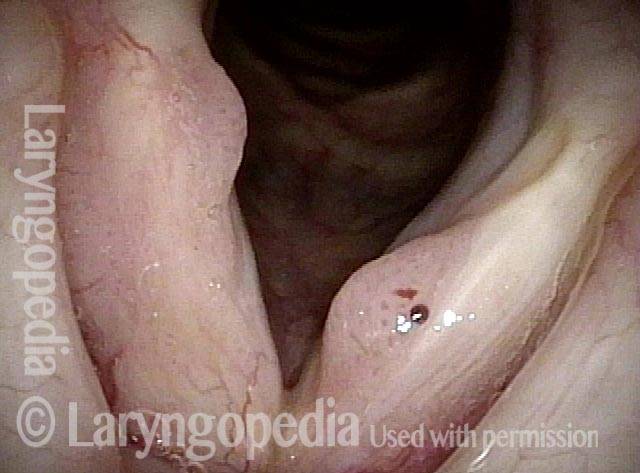
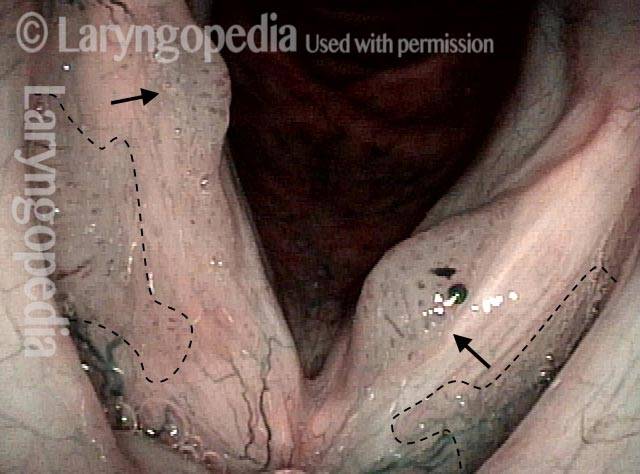
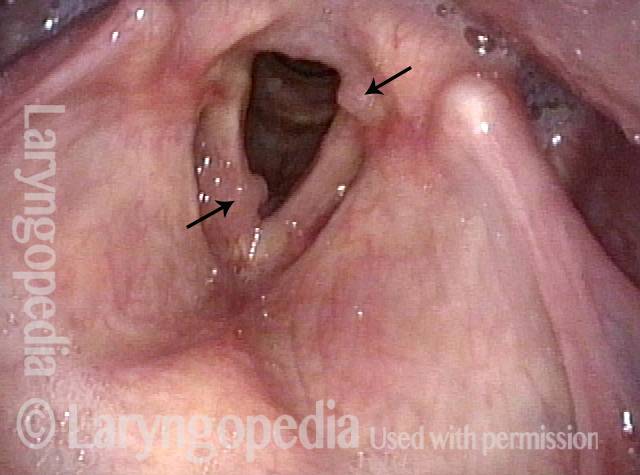
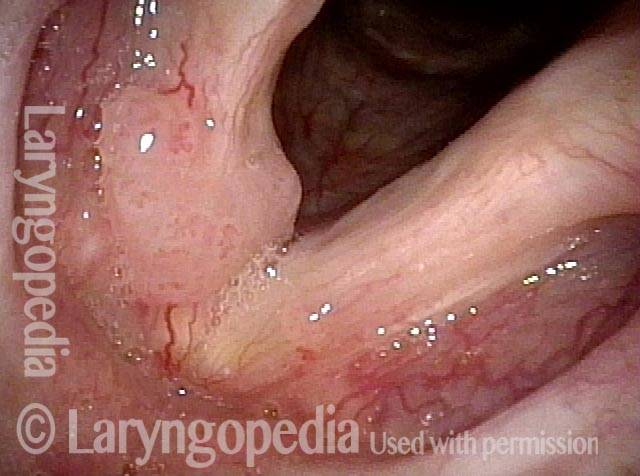
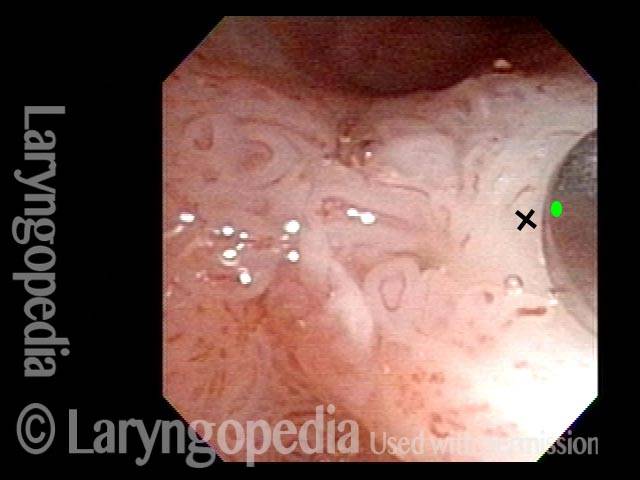
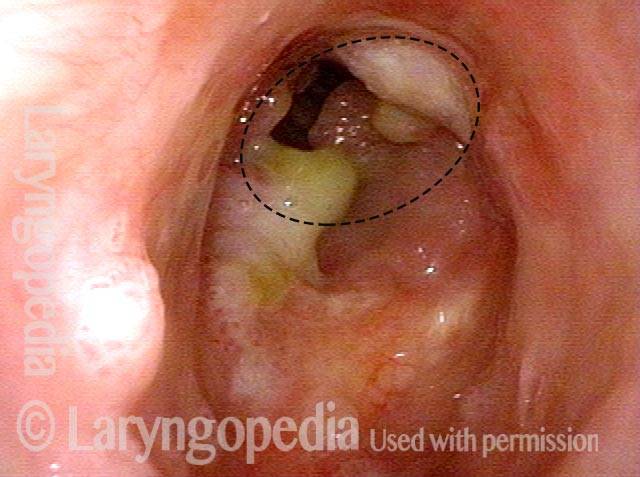
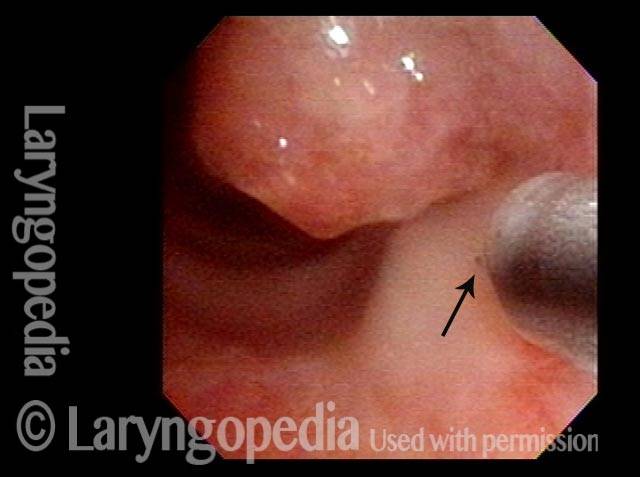
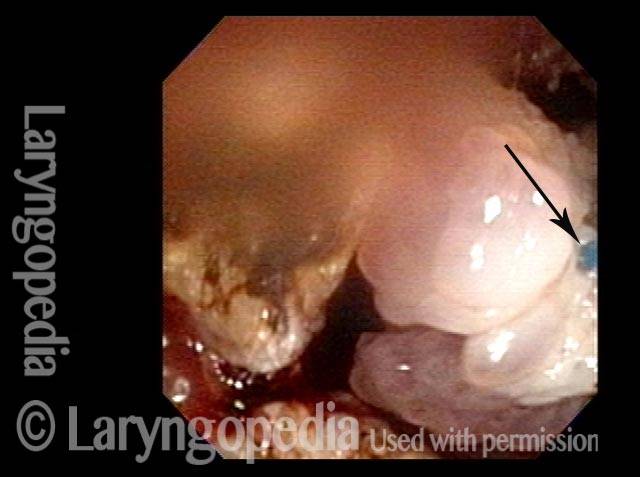
Los crecimientos generalmente asociados con RRP son tumores similares a verrugas, o papilomas, que sobresalen de manera notoria de la superficie en la que crecen, a menudo en racimos similares a uvas. Estos tipos de papilomas generalmente se observan en pacientes que tienen los subtipos de VPH 6 u 11, que son subtipos de menor riesgo de desarrollar cáncer. Hay algunos pacientes con VPH, sin embargo, que manifiestan su infección por VPH con crecimientos más sutiles y aterciopelados dentro de las vías respiratorias, crecimientos de «variante de alfombra», por así decirlo. Aunque estos crecimientos de «variante de alfombra» no tienen la apariencia de verruga de los papilomas típicamente asociados con RRP, existen al menos algunos puntos clave de similitud:- Tanto la “variante de alfombra” como los crecimientos similares a verrugas son lesiones que a veces aparecen, ya sea de forma independiente o conjunta, en pacientes que tienen VPH;
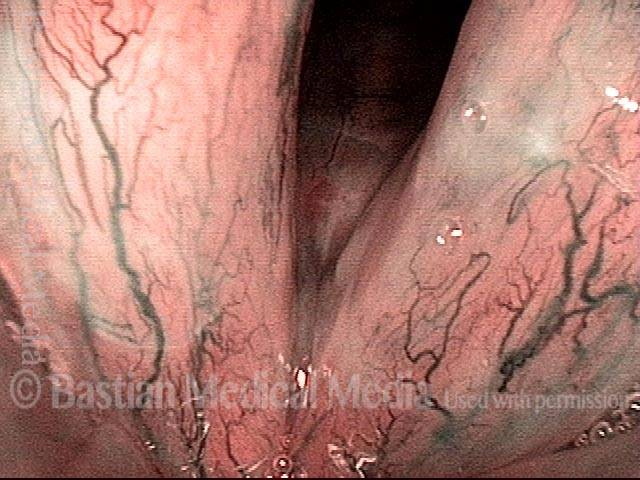
- Tanto la «variante de la alfombra» como los crecimientos similares a verrugas están punteados con marcas vasculares de lunares, porque cada «bucle» en la «alfombra» o cada «uva» en el grupo similar a una verruga tiene su propio núcleo fibrovascular, visto como un punto rojo;
- Tanto la «variante de alfombra» como los crecimientos similares a verrugas pueden alterar la función de la voz;
- Tanto la «variante de alfombra» como los crecimientos similares a verrugas suelen reaparecer si se eliminan.
Tratamiento de la papilomatosis respiratoria recurrente
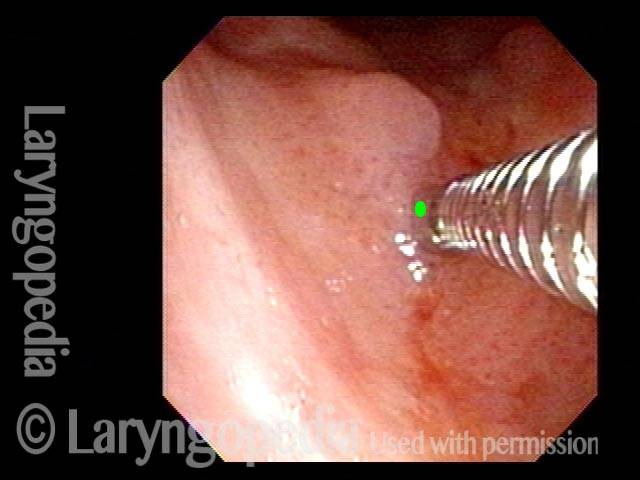
El tratamiento principal para la RRP y otras lesiones inducidas por el VPH es la extirpación quirúrgica cuidadosa y conservadora de los crecimientos. Debido a que estos crecimientos casi siempre recurren, la cirugía generalmente debe realizarse repetidamente, con una frecuencia de varias semanas en los niños, pero en promedio con mucha menos frecuencia en los adultos. Un intervalo común entre cirugías para pacientes adultos es entre cada seis meses y cada dos años, dependiendo de qué tan rápido recurra la PRR u otra lesión relacionada con el VPH y vuelva a afectar la función de la voz del paciente. También hay algunos tratamientos médicos que se han utilizado además de la cirugía, incluidos, entre otros, interferón, indol-3-carbinol, paperas intralesionales o vacuna MMR (sarampión-paperas-rubéola), cidofovir y bevacizumab.Humildad ante el virus VPH: una recurrencia de los papilomas a los diez años
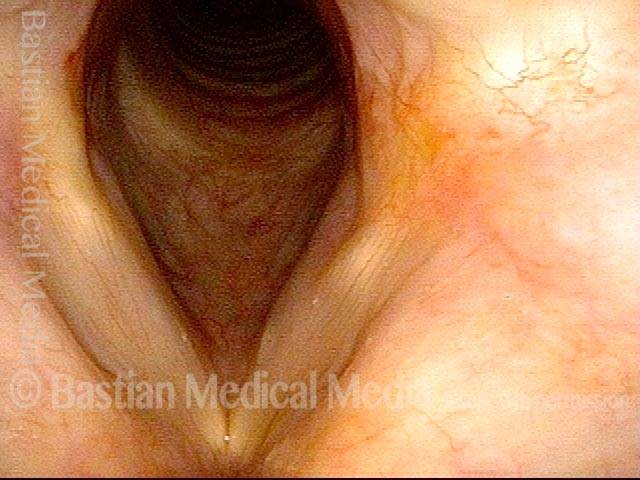
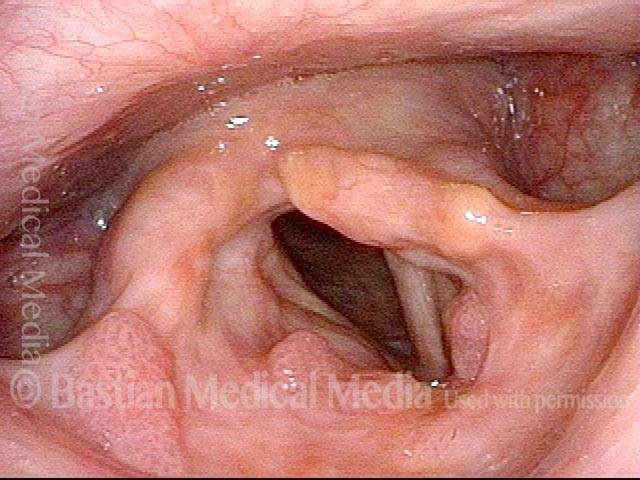
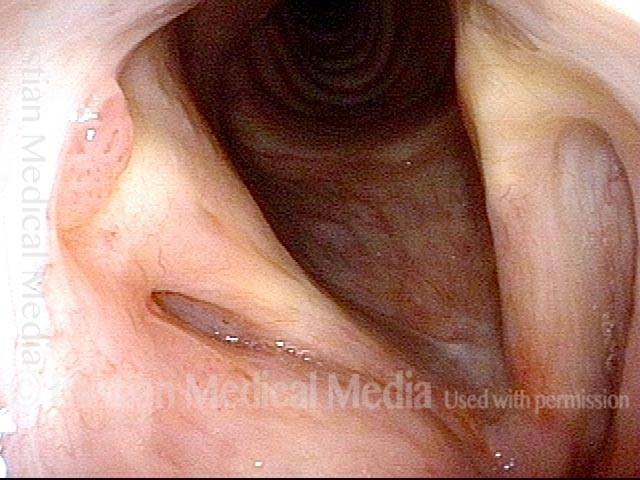
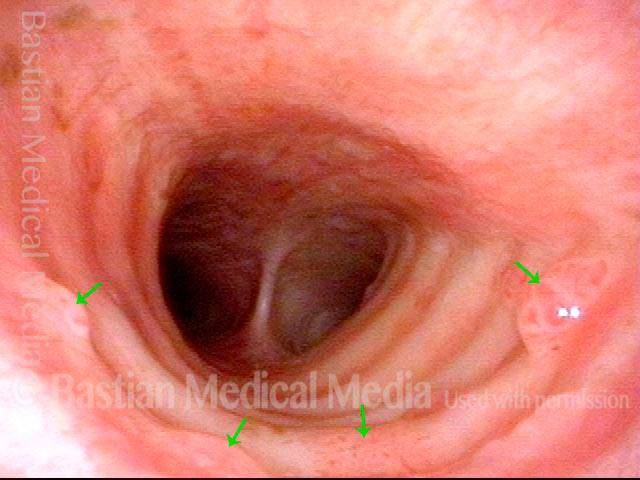
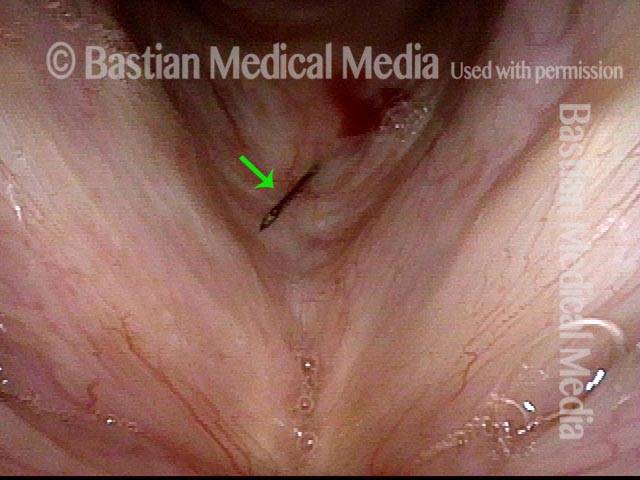
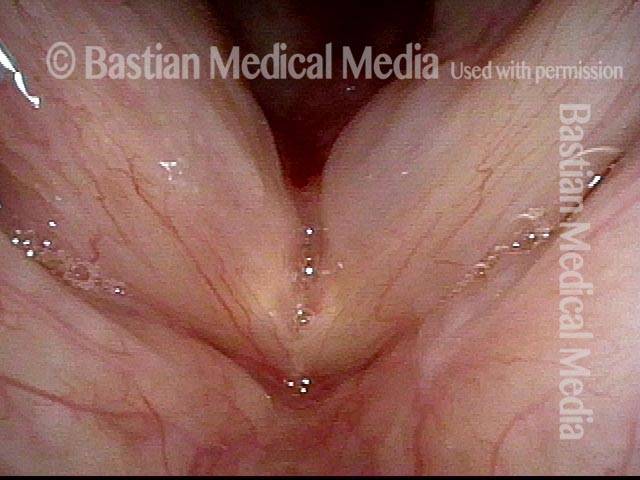
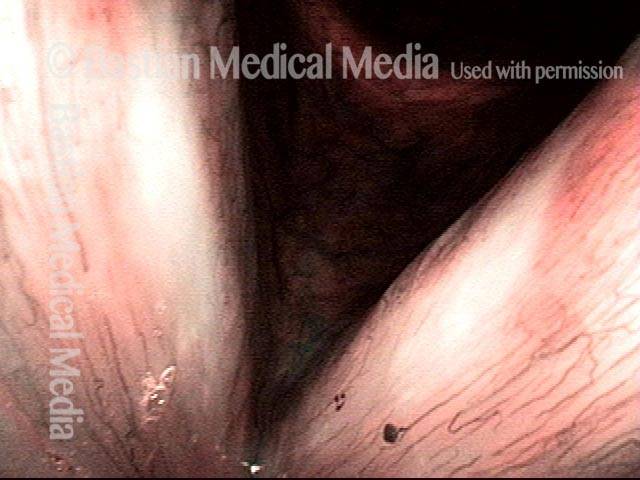
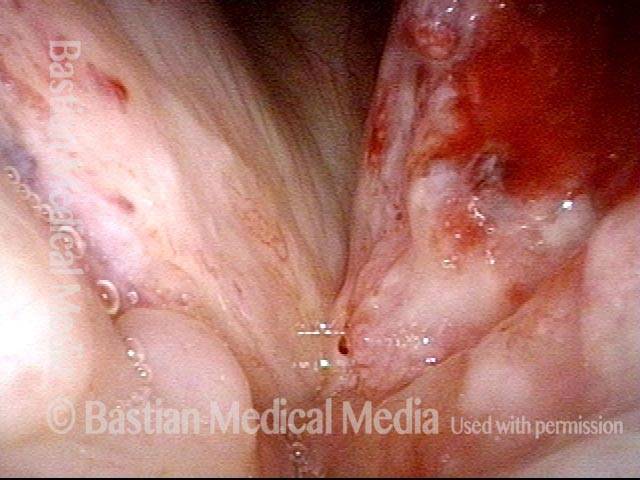
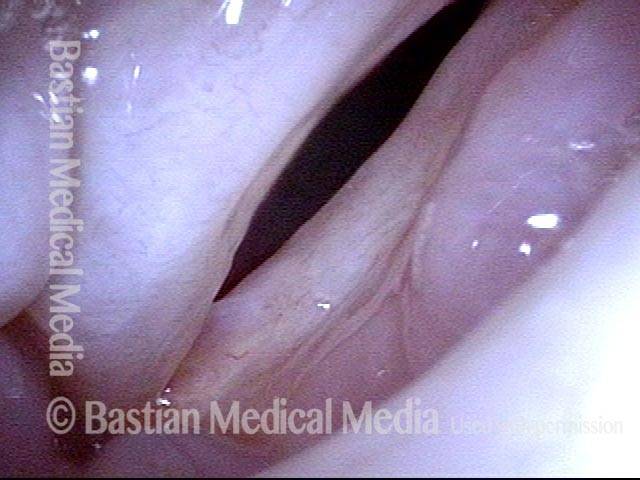
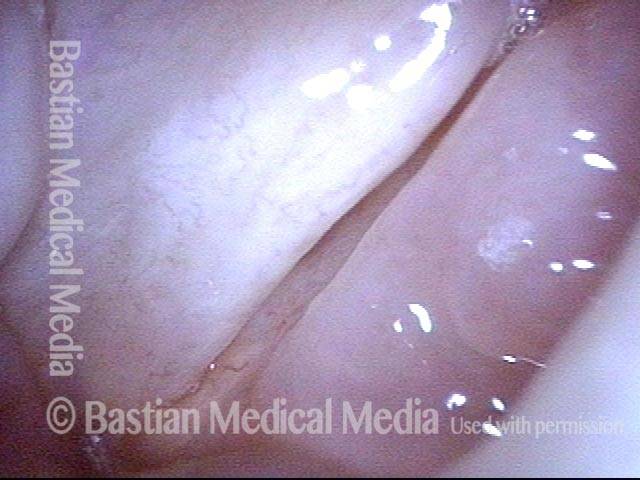
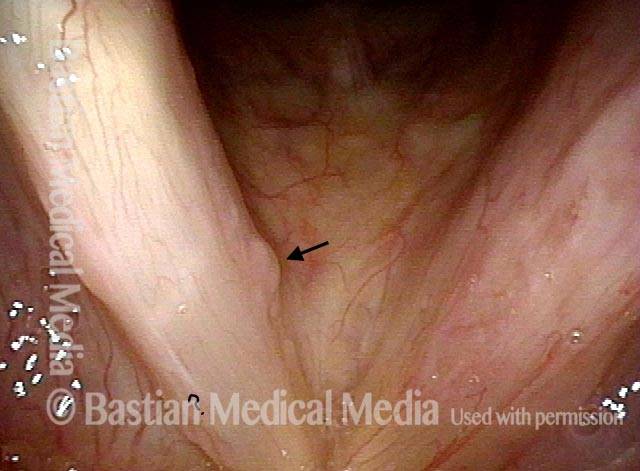
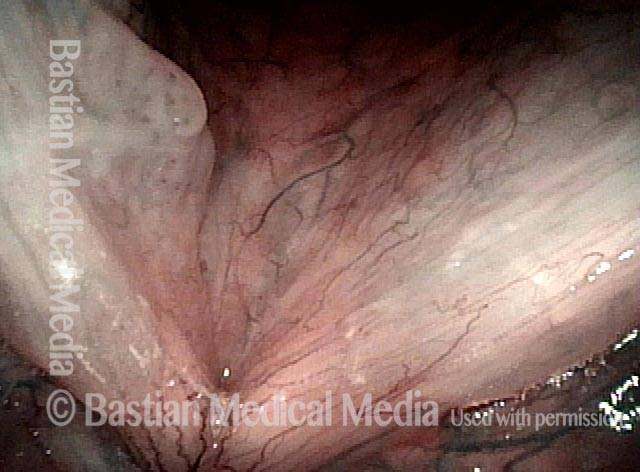
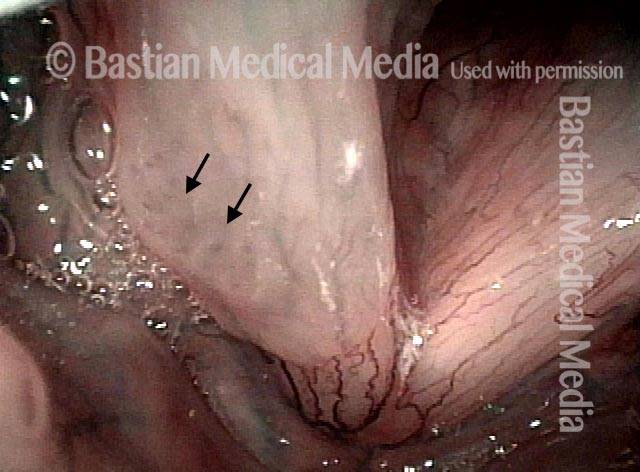
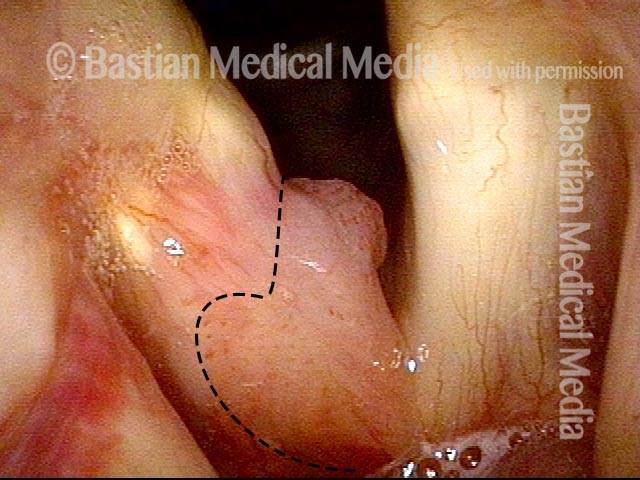
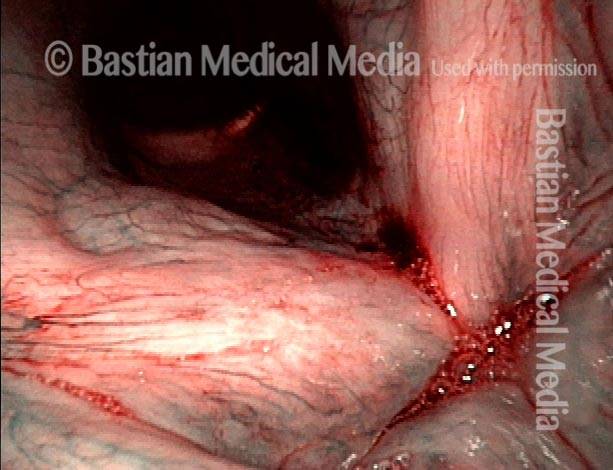
La infección por VPH se considera crónica y provoca el crecimiento recurrente de papilomas en la laringe. Aún así, a veces vemos lo que parecen ser curas, o al menos remisiones a largo plazo. Ese parece ser el caso aquí. Después de un intervalo de 8 años de voz perfecta, el paciente tuvo un aumento repentino de la ronquera que se produjo en las pocas semanas anteriores al último examen a continuación. Esta es una ilustración de por qué a menudo le decimos a un paciente que parece estar curado: “Puede que estés curado, pero generalmente decimos “remisión a largo plazo”. El escenario de este paciente no es raro. ¿Su remisión a largo plazo de 8 años se debió a una cirugía meticulosa? ¿cidofovir? ¿Su respuesta inmunológica? Es imposible decir si fue uno o todos estos factores.
Stippled Vascularity (1 of 8)
HPV infection (2 of 8)
Stippled vascularity (3 of 8)

HPV vascular effect (4 of 8)

16 months later (5 of 8)
Is it long-term remission? (6 of 8)

Recurrent Papilloma (7 of 8)
Stippled vascularity (8 of 8)

Papillomas, HPV Subtype 11, before and After Removal
Papillomas: HPV Subtype 11 (1 of 4)

Papillomas: HPV Subtype 11 (2 of 4)
Papillomas, removed: HPV Subtype 11 (3 of 4)
Papillomas, removed: HPV Subtype 11 (4 of 4)

Papillomas, HPV Subtype 6, Before and after Removal
Papillomas: HPV Subtype 6 (1 of 4)

Papillomas: HPV Subtype 6 (2 of 4)

Papillomas, removed: HPV Subtype 6 (3 of 4)

Papillomas, removed: HPV Subtype 6 (4 of 4)
Papillomas, HPV Subtype 11
Papillomas: HPV Subtype 11 (1 of 3)
Papillomas: HPV Subtype 11 (2 of 3)
Papillomas: HPV Subtype 11 (3 of 3)

Example 2
Papillomas: HPV Subtype 11 (1 of 2)

Papillomas: HPV Subtype 11 (2 of 2)
HPV Lesions
Lesions of HPV Subtype? (1 of 2)

Lesions of HPV Subtype? (2 of 2)

Lesions and Papillomas of HPV, Before and After Removal and Adjuvant Injection
Lesions and papillomas of HPV subtype? (1 of 8)

Subtle lesion (2 of 8)
Open phase (3 of 8)
1 week after removal (4 of 8)

1 week after removal (5 of 8)
Injecting adjuvant (6 of 8)
After injecting adjuvant (7 of 8)
After final adjuvant injection (8 of 8)

Papillomas, HPV Subtype 55, Going Into Remission
Papillomas: HPV Subtype 55 (1 of 4)

Papillomas: HPV Subtype 55 (2 of 4)

Papillomas, in remission: HPV Subtype 55 (3 of 4)

Papillomas, in remission: HPV Subtype 55 (4 of 4)
Papillomas, HPV Subtype 31, Going Into Remission
Papillomas: HPV Subtype 31 (1 of 4)
Papillomas: HPV Subtype 31 (2 of 4)
Papillomas, in remission: HPV Subtype 31 (3 of 4)
Papillomas, in remission: HPV Subtype 31 (4 of 4)

Papillomas, HPV
Papillomas: HPV Subtype? (1 of 2)

Papillomas: HPV Subtype (2 of 2)

Pushing Past Red Herrings to Find the Real Issue
Obvious lesion not important (1 of 3)

Granuloma (2 of 3)

Carpet-varient papilloma (3 of 3)

Papillomas, HPV Subtype 18 or 45
Papillomas: HPV Subtype 18 or 45 (1 of 2)
Papillomas: HPV Subtype 18 or 45 (2 of 2)

Lesions of HPV Subtype 16
Lesions of HPV Subtype 16 (1 of 3)

Lesions of HPV Subtype 16 (2 of 3)

Lesions of HPV Subtype 16 (3 of 3)

Cancer, HPV Subtype 16, Before and After Radiation
Cancer: HPV Subtype 16 (1 of 5)
Cancer: HPV Subtype 16 (2 of 5)
Cancer: HPV Subtype 16, after radiation therapy (3 of 5)

Cancer: HPV Subtype 16, after radiation therapy (4 of 5)
Cancer: HPV Subtype 16, after radiation therapy (5 of 5)
Papillomas, HPV Subtype 45
Papillomas: HPV Subtype 45 (1 of 2)
Papillomas: HPV Subtype 45 (2 of 2)

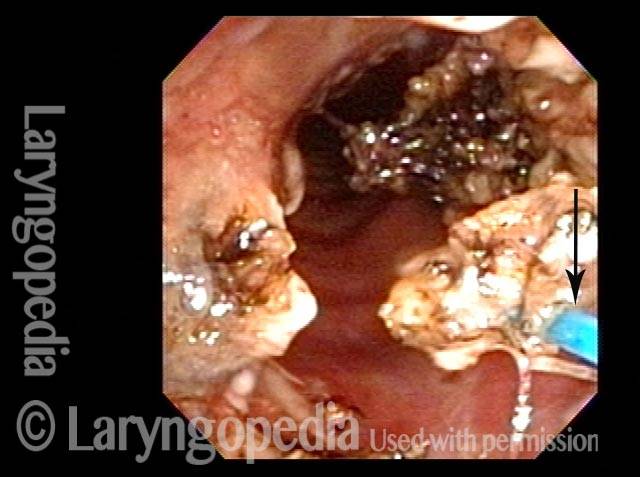
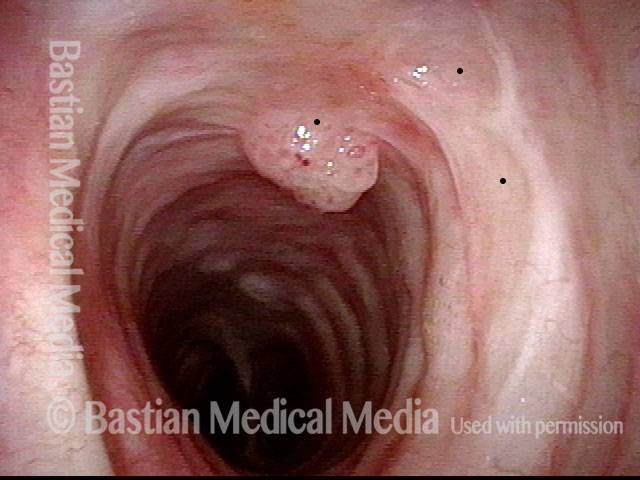
Mid-Tracheal Papilloma, Treated By Thulium Laser
Mid-tracheal papilloma, being treated by thulium laser (1 of 5)
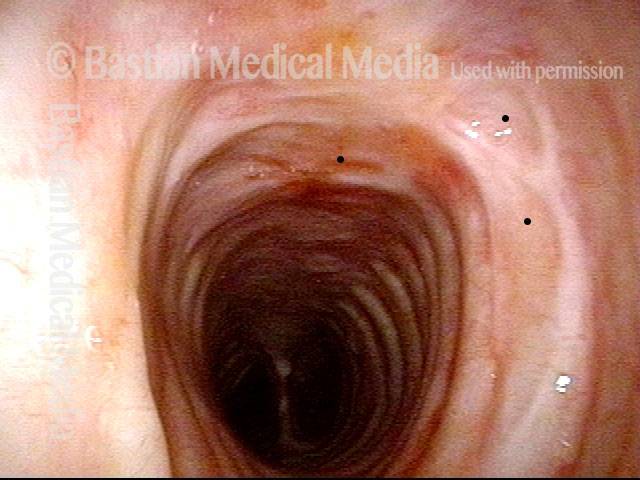
Months after treatment: no papilloma (5 of 5)
Mid-tracheal papilloma, being treated by thulium laser (2 of 5)
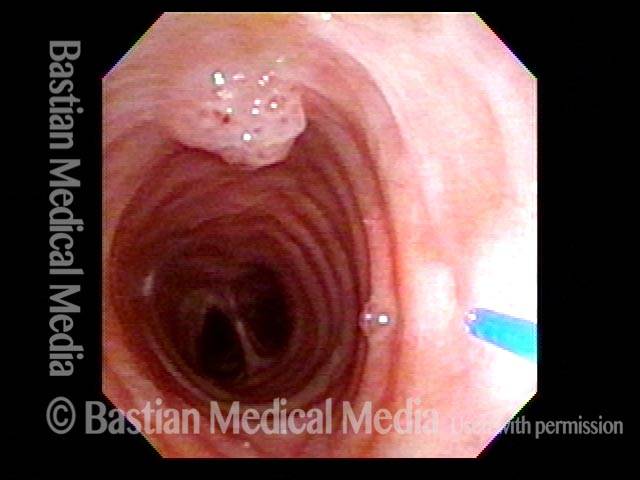
Mid-tracheal papilloma, being treated by thulium laser (3 of 5)

Mid-tracheal papilloma, being treated by thulium laser (4 of 5)

Subtle Papillomas, HPV Subtype 6
Subtle papillomas, HPV subtype 6 (1 of 3)
Subtle papillomas, HPV subtype 6 (2 of 3)

Subtle papillomas, HPV subtype 6 (3 of 3)
HPV Vascular Effect
Two papillomas (1 of 3)
Stippled vascularity (2 of 3)

HPV vascular effect (3 of 3)
Laryngeal Papillomas Rarely Can be Found by … Accident
Papilloma finding (1 of 4)
Narrow band light (2 of 4)
Closed phase (3 of 4)
Open phase (4 of 4)

Winning Papilloma Battles, but not Winning the War….Yet
Left vocal cord lesion (1 of 8)
Narrow band light (2 of 8)
One week after removal (3 of 8)
2 months after removal (4 of 8)
7 months after removal (5 of 8)
Papilloma and mucus (6 of 8)
Stippled vascularity (7 of 8)
HPV disease (8 of 8)
What «Cured» this Case of RRP? Surgery? Cidofovir? The Patient’s Immune System? All Three?
Papilloma (1 of 8)
Stippling (2 of 8)

One week after surgical removal (3 of 8)

Cidofovir injection (4 of 8)
Six months after surgical removal (5 of 8)
One week after second removal (6 of 8)
4 months later, healed (7 of 8)

3 years later, no sign of papilloma (8 of 8)
RRP Cure? Or Just Long Term Remission?
Chronic hoarseness (1 of 4)
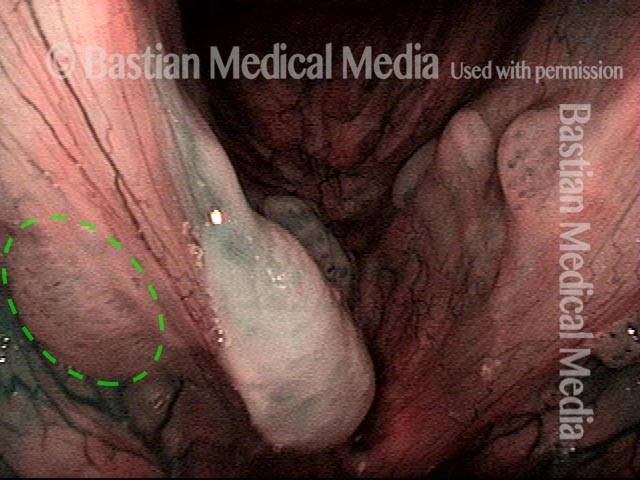
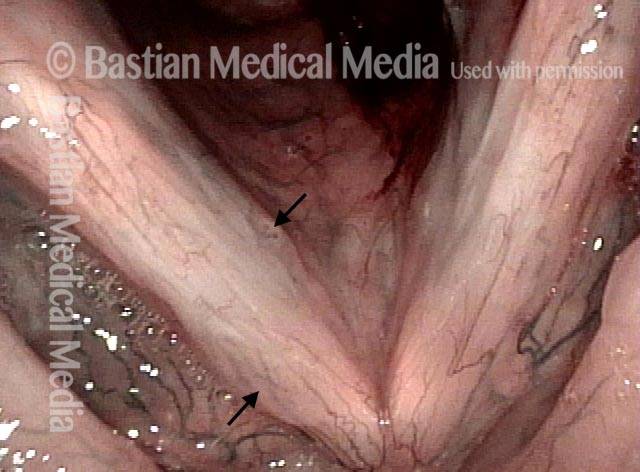
4 months later (2 of 4)
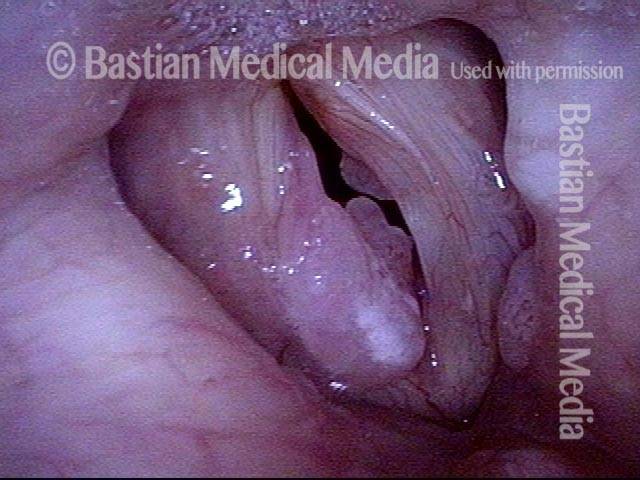
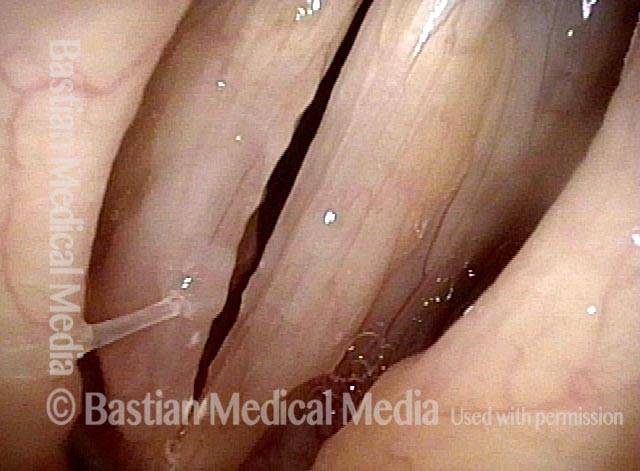
8 months from start of treatment (3 of 4)
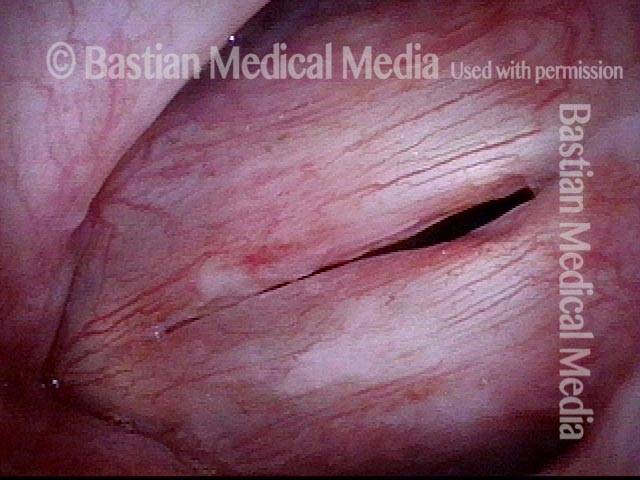
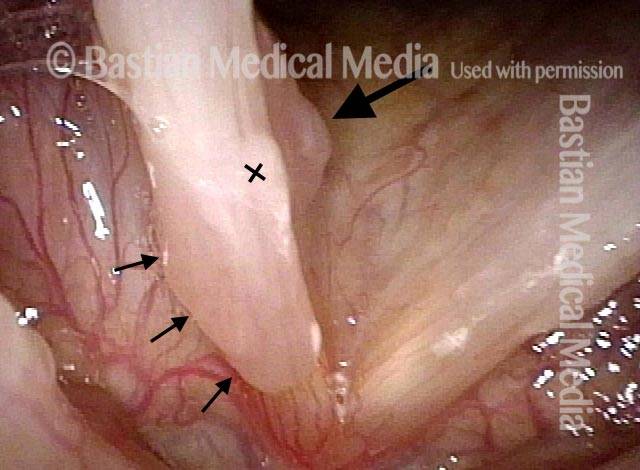
Narrow band lighting (4 of 4)

Polyps Need A Close Look: Here’s One Reason Why
«Polyps» diagnosis (1 of 4)

Papillomas (2 of 4)
Vascular stippling (3 of 4)
Prephonatory instant (4 of 4)

Long-term Remission or even «cure» of RRP/Laryngeal Papilloma
Chronic hoarseness (1 of 6)
Narrow band light (2 of 6)

Higher magnification (3 of 6)
Higher magnification, narrow band lighting (4 of 6)

Post-operation (5 of 6)

Post-operation, narrow band lighting (6 of 6)

Injected Local Anesthetic Causes Blanching
Infiltrating anesthetic (1 of 3)

Blanching (2 of 3)
Subglottis being injected (3 of 3)
Local Rather than Topical Anesthesia can Permit Fairly Major Tracheal Surgery
Obstructive papillomas (1 of 4)
Local injections (2 of 4)
Removal of papilloma (3 of 4)
Improved breathing with papilloma removal (4 of 4)