An incomplete or frustrated form (forme fruste) of Granulomatosis with Polyangiitis (GPA, Wegener’s Granulomatosis) which we believe to be the cause behind some cases of inflammatory subglottic or tracheal stenosis.
Forme Fruste GPA vs. GPA
Unlike full-fledged GPA, this forme fruste variant may or may not necessarily involve the sinus and nasal cavities, and in the author’s caseload of about 60 patients, it has not ever progressed to involve the lungs and kidneys.
Treatment Methods
Such patients can go for years with only the need for intermittent dilation of the subglottic or tracheal narrowing. This disorder may be the same as what some call “idiopathic subglottic stenosis,” for which some have recommended cricotracheal resection and reanastomosis as treatment.
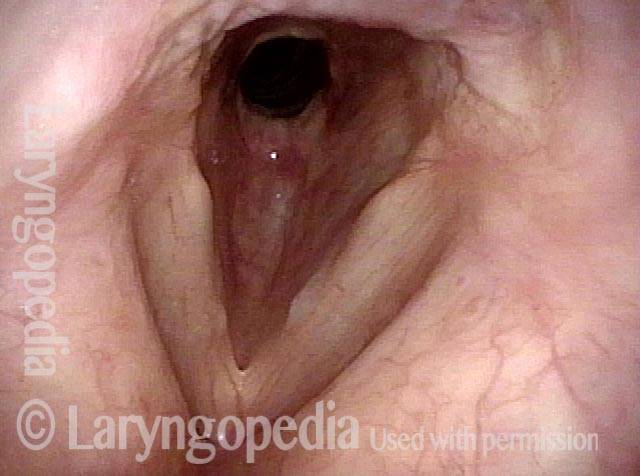
Subglottic / Tracheal Stenosis
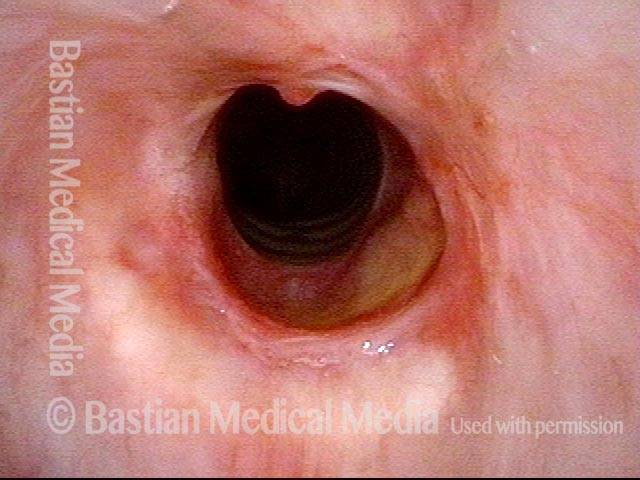
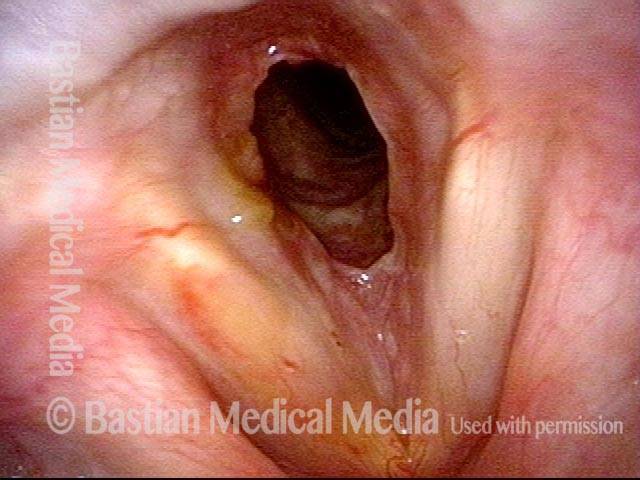
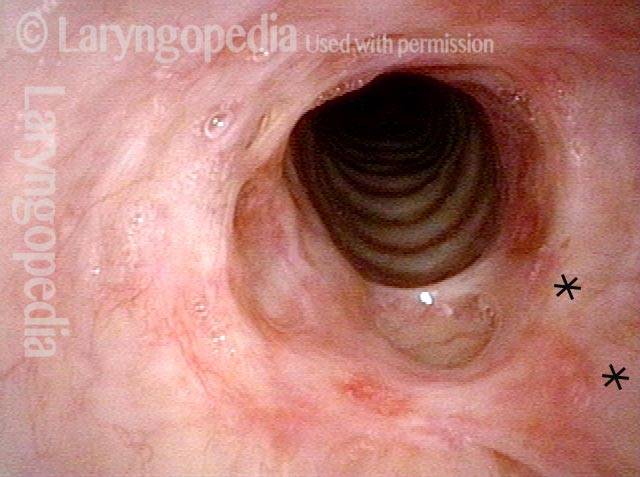
Wegener’s granulomatosis (1 of 4)
Inflammatory subglottic/tracheal stenosis, thought to be the result of an incomplete expression of Wegener’s granulomatosis (no history of trauma).
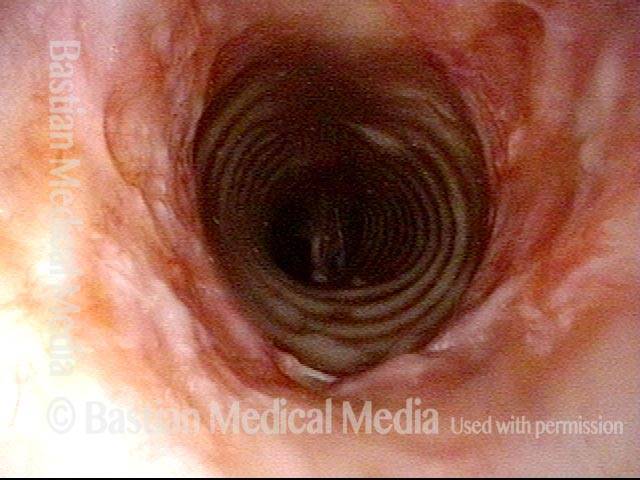
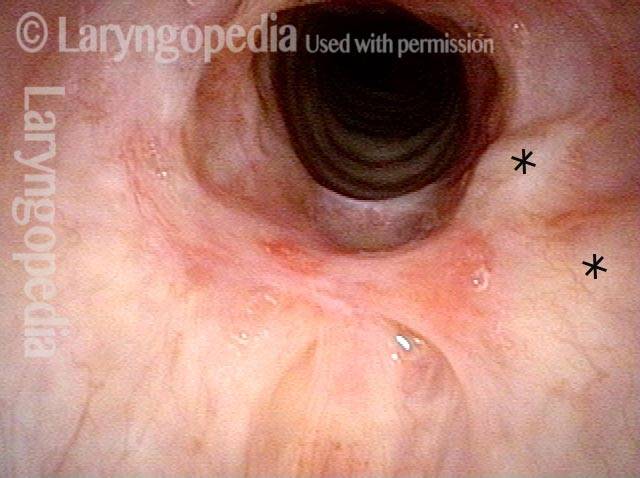
Subglottic / Tracheal stenosis (2 of 4)
Close view, from vocal cord level.

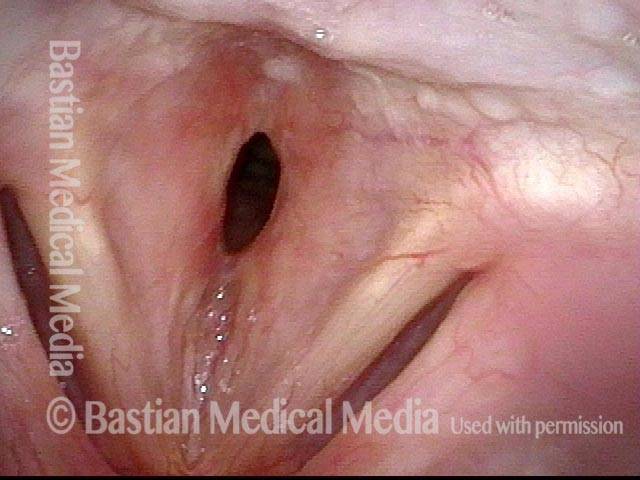
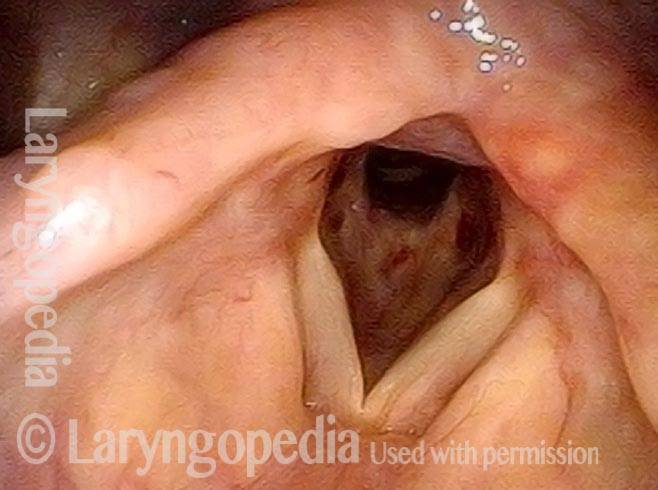
Subglottic / Tracheal stenosis (3 of 4)
Close view, from just above vocal cords.

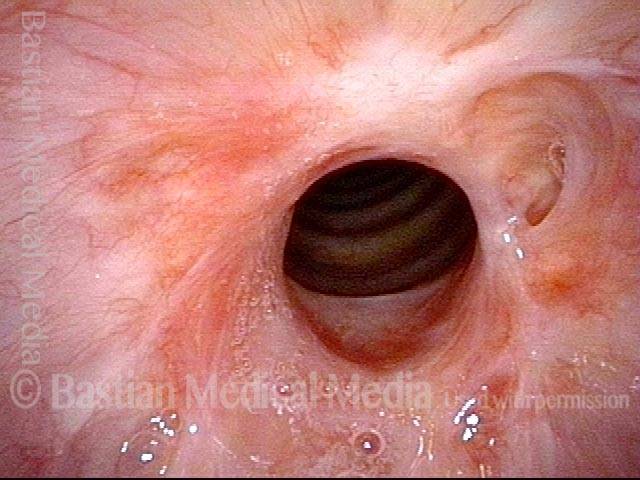
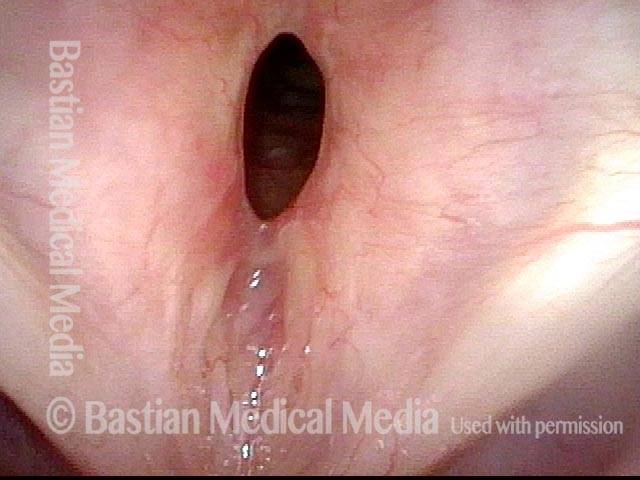
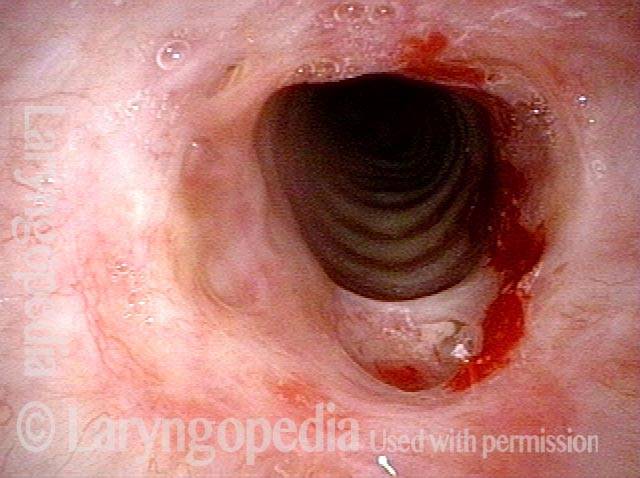
Inflammed Stenosis (4 of 4)
Close view, showing the inflammatory nature of the stenosis.

Tracheal Stenosis, Due to Forme Fruste Wegener’s Granulomatosis
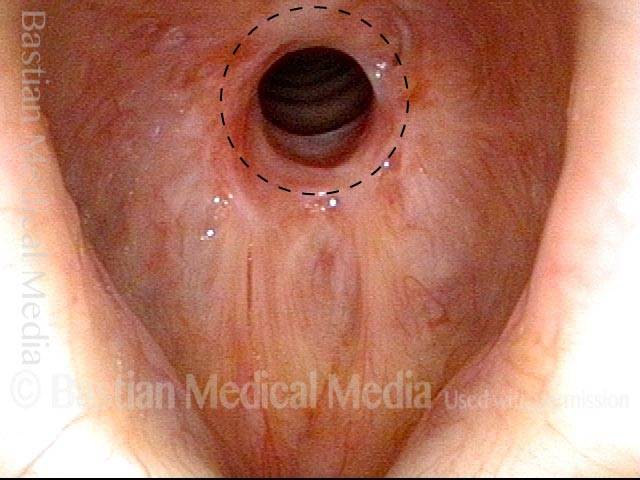
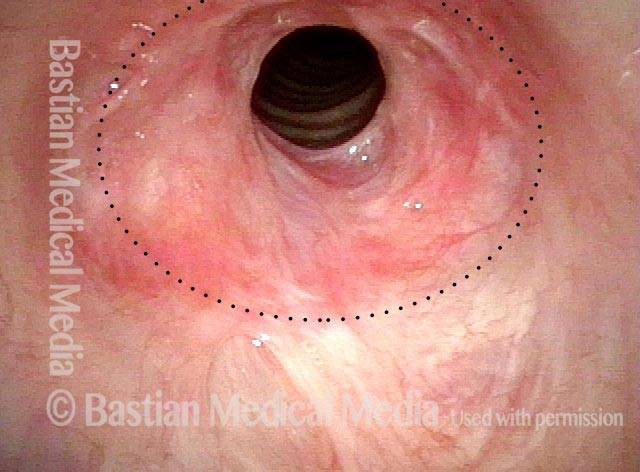
Tracheal stenosis (1 of 3)
View from level of vocal cords shows residual lumen of airway at only ~35% of normal. The dotted circle shows how big the lumen should be.
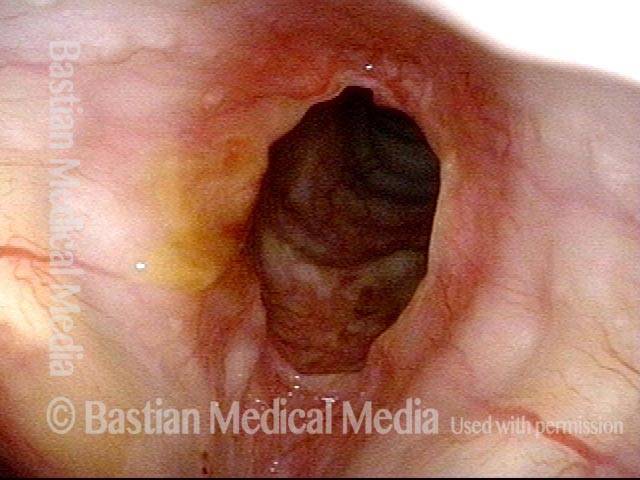
Tracheal stenosis (2 of 3)
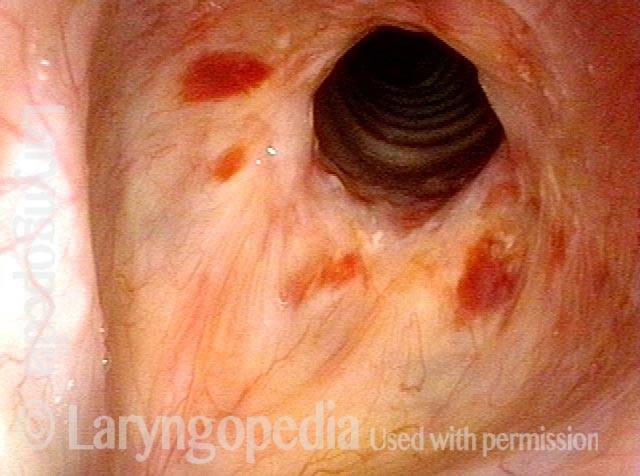
Closer view shows the characteristic appearance of mucosa and the inflammatory nature of the stenosis (pinkness).
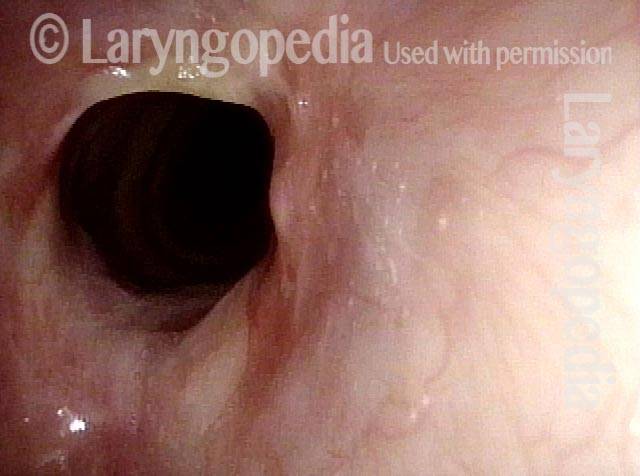
Just below the tracheal stenosis (3 of 3)
After just passing through the stenotic area, distal trachea is normal in caliber and color.

Subglottic Stenosis, Before and After Dilation
Subglottic stenosis, before dilation (1 of 2)
This individual has undergone at least a dozen prior dilations, each of which provides dramatic relief from noisy breathing and exercise intolerance. Here the patient is halfway to needing re-dilation, due to the typical inflammatory stenosis that is seen. Compare with photo 2.
Subglottic stenosis, after dilation (2 of 2)
One week after one of this patient’s dilations (with Kenalog injection and topical Mitomycin C), showing a dramatic widening of her airway; compare with photo 1. After a number of years, inflammatory lesions such as this sometimes “burn out,” and the interval between dilations increases.
Example 2
Subglottic stenosis (1 of 5)
Middle-aged woman with unexplained shortness of breath and noisy breathing, due to this idiopathic inflammatory and very high subglottic stenosis. The patient initially declined dilation due to her anxiety. She also had granularity of the nasal septum and a positive ANCA profile for Wegener’s granulomatosis.

Subglottic stenosis, worsened (2 of 5)
Five months later, the symptoms became intolerable, and the stenosis was noted to be slightly narrower and with a greater posterior component. The patient agreed to dilation.
Subglottic stenosis, worsened (3 of 5)
Same exam as photo 2; this close-up view shows more clearly the inflammatory nature of this stenosis.
Subglottic stenosis, after dilation (4 of 5)
Five days after outpatient dilation, triamcinolone injection, and topical mitomycin C application. The patient’s symptoms have vanished, the harsh inspiratory noise is no longer heard, and the size of the airway, though still not normal, is more than doubled. Compare with photo 2 of this series.
Subglottic stenosis, after dilation (5 of 5)
Same exam as photo 4, close-up view. Intensification of the inflammatory changes of this stenosis are expected so early after dilation. Compare size of the stenosis with photo 3 of this series.
A Soft Finding to Support a Diagnosis of Forme Fruste Wegener’s Granulomatosis
Inflammatory subglottic stenosis ( 1 of 4)
Middle-aged woman with chronic difficulty breathing for about two years. Initially treated unsuccessfully for asthma, and recently found to have this clearly inflammatory subglottic stenosis. No prior history of trauma or endotracheal intubation. Workup for Wegener’s granulomatosis was technically negative, and biopsy showed the usual “acute and chronic inflammation.”

Closer view indicates a forme fruste of Wegener’s granulomatosis (2 of 4)
Closer view, showing the clearly demarcated (dotted line) area of inflammation and narrowing. Normal tracheal rings are seen in the shadow, below the stenosis. Negative ANCA notwithstanding, we believe this is a forme fruste of Wegener’s granulomatosis.
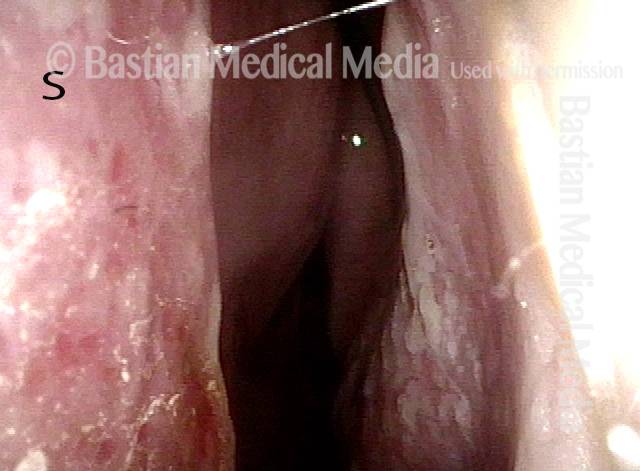
Inflammation on septum (3 of 4)
As is often the case in persons with inflammatory subglottic stenosis of unknown cause, there are some signs of inflammation in the nose, too, usually on the septum, denoted here with “S. ” Right side of the septum is subtly abnormal.
Closer view of septum (4 of 4)
Here, under narrow-band (blue) light, the mottled, inflammatory appearance of the right side of the septum (S) is more clearly seen.
Stenosis Before and After Dilation for Forme Fruste Wegener’s
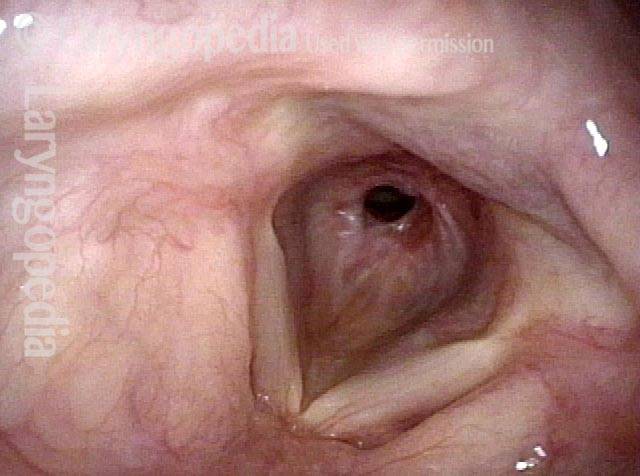
Subglottic stenosis (1 of 5)
High-grade subglottic stenosis in a woman diagnosed syndromically with forme fruste Wegener’s granulomatosis-related subglottic stenosis. With a narrowing less than 50%, she is very symptomatic. Her breathing is noisy, and her forced inspiration time is about 3 seconds. Compare with photo 4.
Inflammation (2 of 5)
Closer visualization reveals the inflammatory nature of the stenosis.

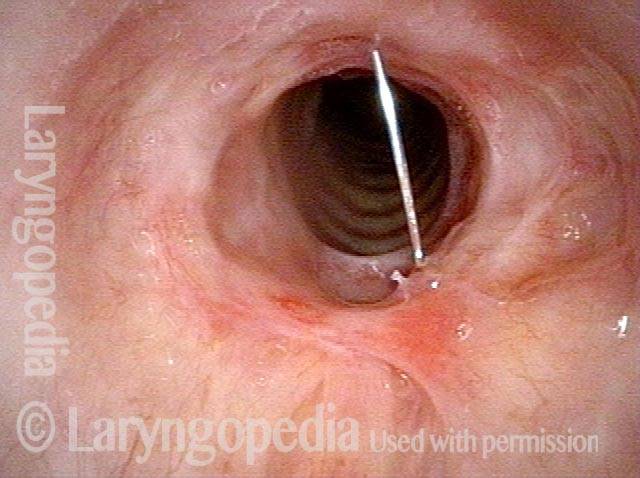
Flexible scope (3 of 5)
Here the distal chip flexible scope has passed through the narrowing not only to see into distal trachea, but also as a breathing test. The patient becomes very aware of reduced space and this indicates a marginal airway.

Post-dilation (4 of 5)
A week after dilation, triamcinolone injection and mitomycin C application, the patient says breathing is now normal, and forced inspiration time is only a second in duration–normal. Compare with photo 1.
Post-operative bruising (5 of 5)
Closer visualization with early postoperative bruising. The trachea is now easily visible through the larger opening. Compare with photo 2.
A Different Approach to Inflammatory Tracheal Stenosis
Planning on periodical injections (1 of 4)
Three months after successful dilation, the patient says breathing is still normal. We are planning an injection of triamcinolone every 3 or 4 months, attempting to lengthen the interval between dilation procedures. Please note that the *s (right of photo) are for comparison with photo 2.
Long-acting steroid (2 of 4)
A needle has been passed into the anterior neck to place submucosal long-acting steroid. Note the bulging and blanching at the *s and compare with photo 1.
Needle going into the posterior of stenosis (3 of 4)
Here the needle has been passed translumenally and into the posterior portion of the stenosis.
Posterior tracheal wall (4 of 4)
The posterior tracheal wall has flattened as compared with photo 3, due to the infiltrated medication.
Vascular Manifestations of Wegener’s-related Septum Changes, and Subglottic Stenosis Indistinguishable from Forme Fruste Wegener’s
View inside left nostril (1 of 4)
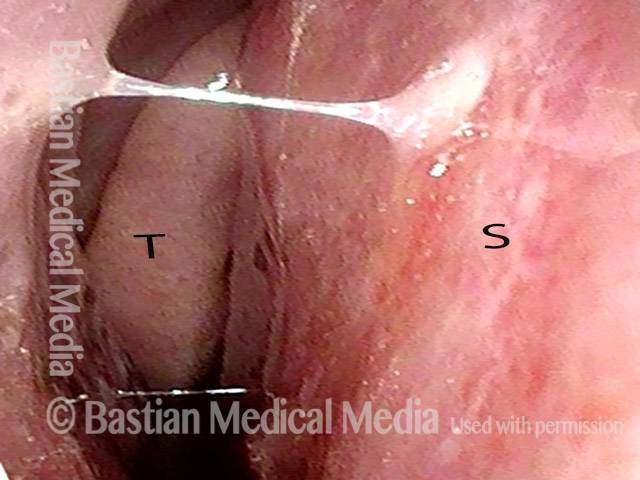
This man has Wegener’s Granulomatosis, with sino-nasal, subglottic, and pulmonary effects, and is on immunosuppressive therapy with very good clinical results. This view is just inside his left nostril and our focus – seen better in the next photo – is the stippled vascular pattern sometimes seen in auto-immune disorders. (S = septum, and T = inferior turnbinate.)
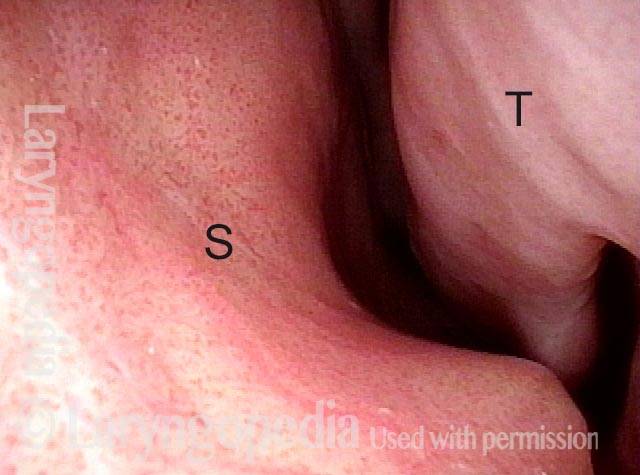
Narrow band light (2 of 4)
Under narrow band light, the unusual vascular pattern of both septum and turbinate becomes much more obvious.

Distant view (3 of 4)
In this distant view, his subglottic stenosis looks just like the many other examples in Laryngopedia of forme fruste Wegnener’s. The stenosis seen with both entities are visually indistinguishable.
Closer view (4 of 4)
A closer view of the stenosis reveals more clearly the adherent mucus that is so difficult for such patients to cough out due to the “speed bump” interruption of the mucociliary blanket at the stenosis.
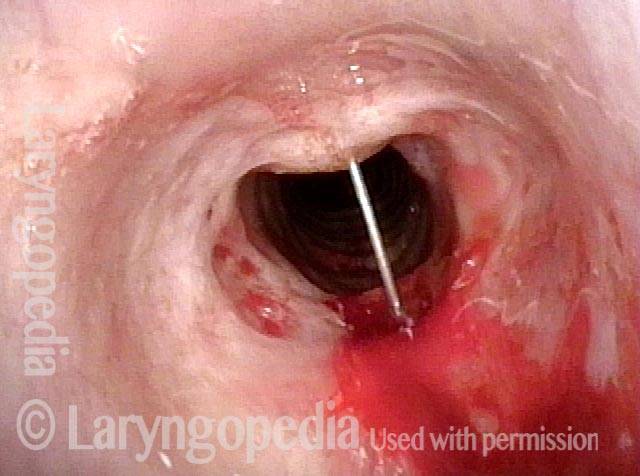
One Way to Deliver Topical Anesthesia Despite A Powerful Gag Reflex…
Powerful gag reflex (1 of 4)
The usual method of dripping topical anesthesia into larynx, subglottis, and trachea from above through an Abraham cannula is difficult due to a powerful gag reflex. Here, the tip of a short 25 gauge needle has entered through the cricothyroid membrane, just below the anterior commissure.

Patient inhaling (2 of 4)
2% lidocaine has just begun to squirt through the needle with the patient inhaling.
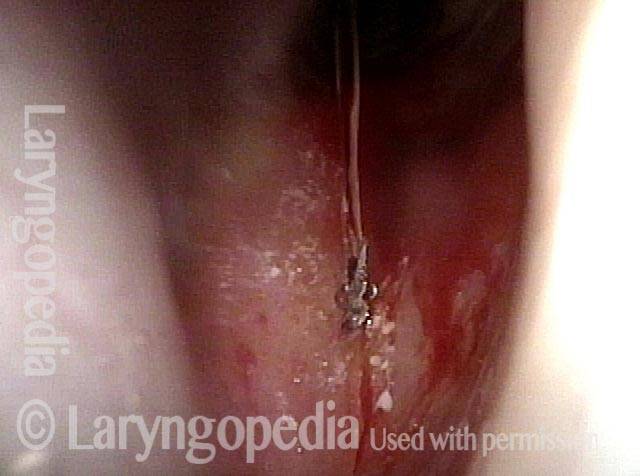
Patient coughs (3 of 4)
Half a second later, the topical anesthetic is splattering (see streaks) and as the patient coughs. This will fully anesthetize the area topically.

Topical anesthesia applied (4 of 4)
The topical anesthesia established by this method now allows injection of kenalog (see white submucosal bulge) into the posterior tracheal wall as a means of managing this patient’s subglottic stenosis likely due to forme fruste Wegener’s granulomatosis.