Thyroid Cartilage Fracture and Dislocation of the Right Cricothyroid Joint
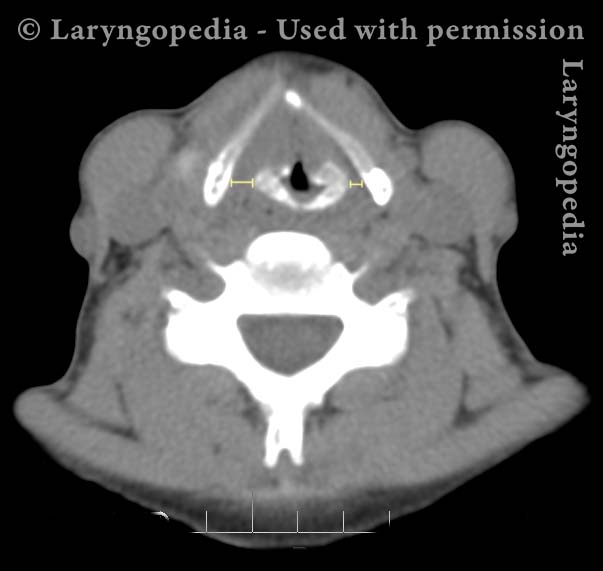
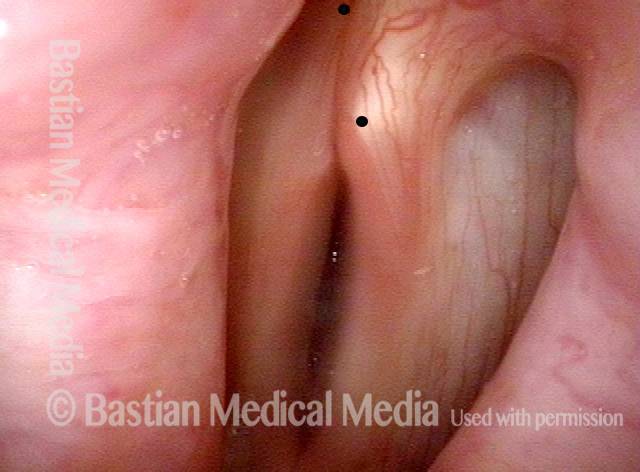
This middle-aged woman fell and hit the front of her neck on a large bottle she was carrying. Voice was altered immediately, though not completely gone. There was no significant hemoptysis but it did hurt to swallow. She also developed subcutaneous air in her neck. The CT scan showed a nondisplaced thyroid cartilage fracture anteriorly. But the previously-overlooked injury was disruption of the right cricothyroid joint. The right thyroid ala was positioned farther posteriorly on the cricoid cartilage, foreshortening the right vocal cord.
Following our rule of thumb that the repaired larynx must be better than the injured larynx, and that the surgical repair trauma could not be worse than the injury trauma, it was decided to leave this problem unrepaired. That’s because the recurrent nerve on the right side would be put at great risk by trying to reattach the cricothyroid joint, which would become ankylotic anyway.
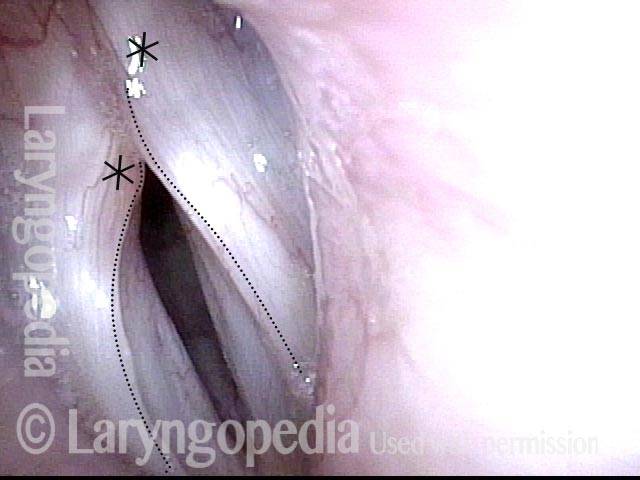
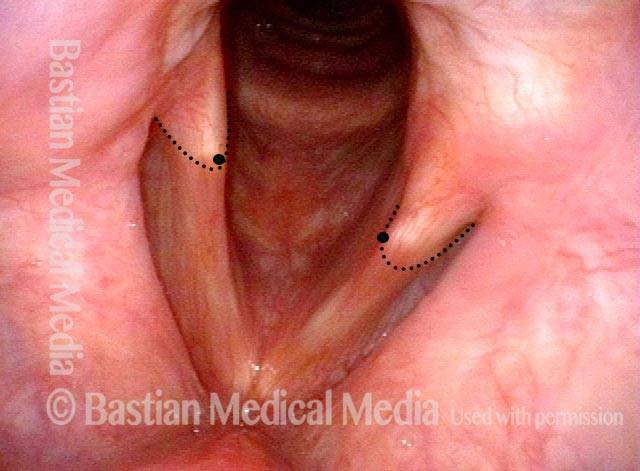
At original examination, bruising, swelling of the right cord is seen, but fairly good mobility of that cord for phonation and breathing. Part of the reason for the convexity is not only swelling but also foreshortening of the right cord as compared with the left.
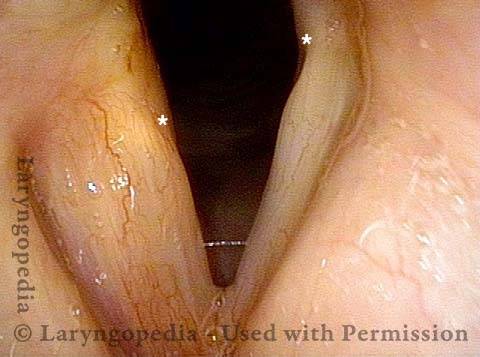
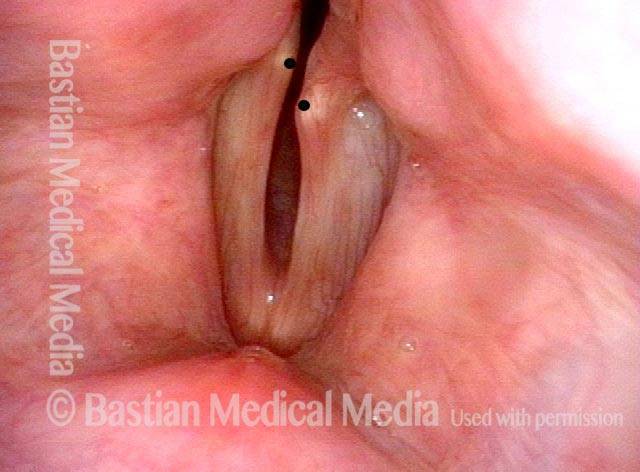
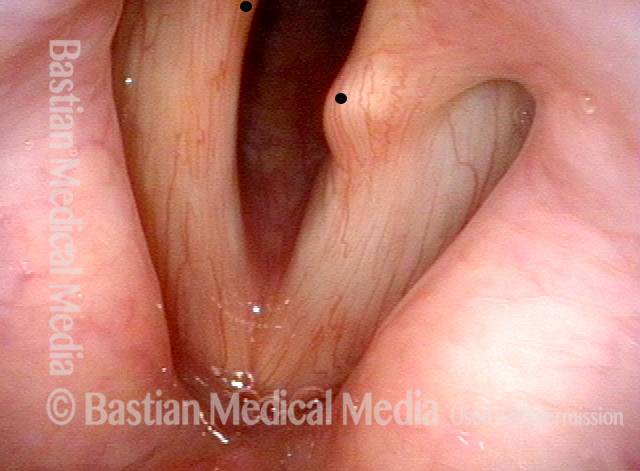
At a follow up examination several weeks later, speaking voice was extremely functional though lacking in expected upper range due to loss of mobility at the cricothyroid joint. The patient found this result acceptable compared with proceeding to repair with such uncertain results.
Larynx fracture (1 of 10)

Larynx fracture (2 of 10)

Larynx fracture (3 of 10)

Larynx fracture (4 of 10)
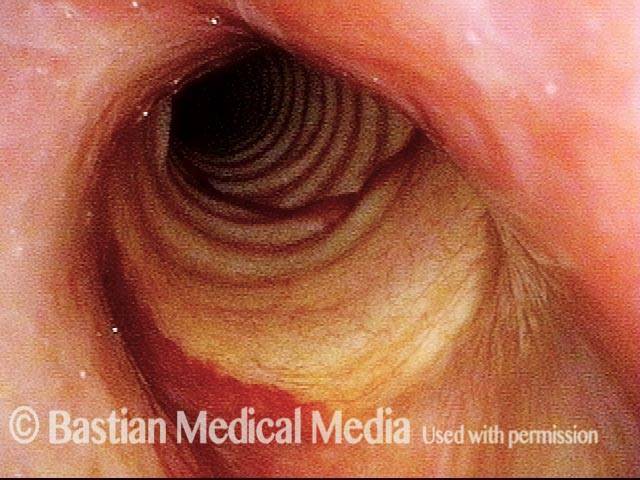
X-ray of Fracture (5 of 10)

Bruising largely resolved (6 of 10)

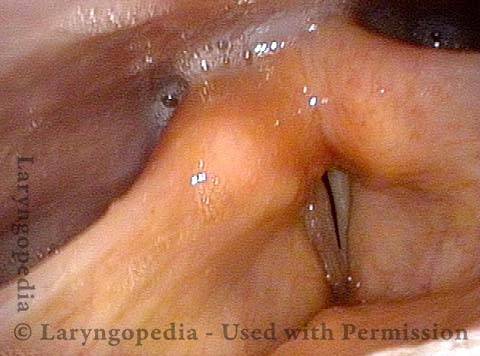
Anterior subluxation (7 of 10)
Good approximation (8 of 10)
Resolved cricoid bruising (9 of 10)

Resolved Bruising (10 of 10)
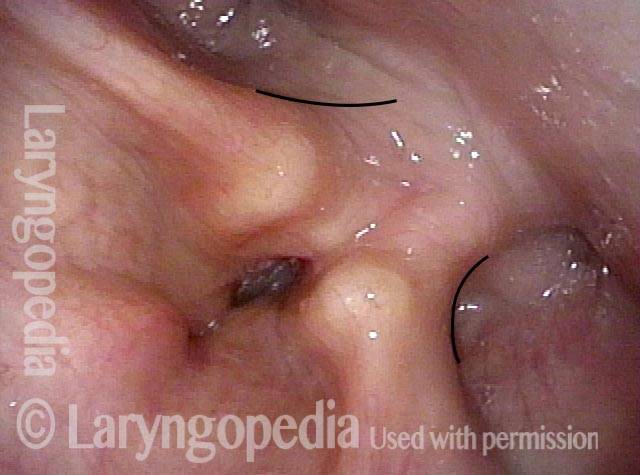
Antero-Superior Fracture of Cricoid Cartilage Containing the Cricoarytenoid Joint
Breathing position (1 of 4)
Mis-match (2 of 4)
Prephonatory view (3 of 4)
Phonation (4 of 4)
Probable Larynx Fracture Seen Via Endoscopic Cues
This man sustained a sports injury a few months earlier including a blow to the anterior neck. Voice was instantly drastically altered. A fracture is suspected via endoscopic “cues.”
Fracture suspected (1 of 5)

Phonation (2 of 5)
Convex margin (3 of 5)

Closed phase (4 of 5)

Open phase (5 of 5)

Larynx Fracture—Endoscopic Nuances Are Fascinating!
Twenty years earlier, during a hockey game, this man’s anterior neck was hit by a puck. His voice has never been the same, and he was told there was a “voicebox injury.”
Hockey injury (1 of 4)

Phonation (2 of 4)

Phonation under strobe light (3 of 4)

Foreshortening of soft tissue (4 of 4)