 IA-only paresis refers to weakness or paralysis of the larynx’s interarytenoid (IA) muscle, an unpaired muscle spanning between the bodies of both arytenoid cartilages but with normal function of the other muscles in the larynx. The IA muscle helps to bring the posterior commissure together for voice production and, more specifically, to bring the bodies or “heels” of the arytenoid cartilages on each side simultaneously to the midline. The following are indicators of IA-only paresis:
IA-only paresis refers to weakness or paralysis of the larynx’s interarytenoid (IA) muscle, an unpaired muscle spanning between the bodies of both arytenoid cartilages but with normal function of the other muscles in the larynx. The IA muscle helps to bring the posterior commissure together for voice production and, more specifically, to bring the bodies or “heels” of the arytenoid cartilages on each side simultaneously to the midline. The following are indicators of IA-only paresis:
- Movement: The vocal cord opens normally for breathing. From a distance, it can appear to close normally for voicing, but more intense and up-close inspection shows a persistent posterior commissure opening not only for voicing but also at the moment of cough and Valsalva maneuver. Without confirming that the heels of the arytenoids cannot come together regardless of task, the possibility of a functional posturing abnormality (such as seen for nonorganic voice disorders) cannot be ruled out. If voice change has occurred abruptly, and the above criteria pertain, IA-only paralysis can be considered; if of very gradual onset, the clinician will first want to rule out a deformity of the cricoarytenoid joints, such as can be seen with cricoid chondrosarcoma.
- Position and appearance: Position is normal during breathing, but the posterior commissure cannot be brought to full closure whether during voicing, cough, or Valsalva maneuver.
- Appearance during voicing (under strobe lighting): Vibration of the vocal cords can be normal, though, again, the persistent posterior commissure gap will be seen. The tone and bulk of the vocal cords themselves are normal.
- Voice quality: Air-wasting, and with shortened phonation time, but without the luffing and diplophonia often apparent when the thyroartyenoid (TA) muscle is also paralyzed.
Other variants of vocal cord paresis include TA-only, TA + LCA, PCA-only (posterior cricoarytenoid muscle), and LCA-only (lateral cricoarytenoid muscle).
The Rarest Paresis: Interarytenoid (IA) Weakness, Manifested as Inability to Pull the “Heels” of the Arytenoid Cartilages into Contact
Large gap during phonation (1 of 7)
This elderly patient’s voice became suddenly severely weak and whispery approximately 1 week after a URI. She is also coughing frequently on liquids. During attempted phonation, the gap between the cords is enormous; both “heels” (h) and “toes” (t) of the arytenoid cartilages. There is no lateral turning of the tips of the vocal process, suggesting that LCA muscles are functioning normally. The significance of bowing is hard to evaluate (is it “baseline” or part of the paresis?).

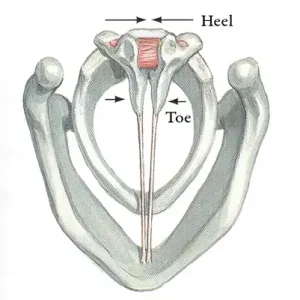
Interarytenoid muscle (2 of 7)
This drawing by Frank Netter shows the interarytenoid (IA) muscle (arrow). It pulls the bodies of the arytenoids together.

Atrophied right cord (3 of 7)
Here, while she is quietly breathing, you can see that PCA (lateralizing) muscles are unimpaired. TA muscles are again hard to evaluate fully in this position. The right cord is arguably atrophied as compared with the left (not subsequently validated).

IA muscle is not working (4 of 7)
At closer range, this vocal cord posture is the same when the patient responds entirely believably to rapid-fire and repeated requests for phonation, Valsalva, and throat clearing/coughing. A nonorganic disorder is ruled out. The only reasonable conclusion: the IA muscle is not working or it has perhaps avulsed (the latter hypothesis is disproven, below). Dysfunction of the cricoarytenoid joints on a sudden basis is arguably not a reasonable alternate explanation. Vocal processes point straight anteriorly (arrows), again suggesting that LCA muscles are intact. There is no “luffing” with her loudest (whispery) phonation, and this suggests that TA muscles are also functioning normally.
3 months later (5 of 7)
Approximately 6 weeks after the initial drastic loss of voice, the patient noted some improvement. By this visit, 3 months later, her voice seemed normal to her and the clinician. Here, we can see that both “heels” and “toes” (body of arytenoid and tips of vocal processes, respectively) fully approximate. This is a pre-phonatory instant, before the vibratory blur commences.
Recovery of (IA) muscle (6 of 7)
A closer view of the posterior commissure showing again complete closure of the posterior commissure. Compare with photo 4. The only reasonable explanation seems to be recovery of interarytenoid (IA) muscle function.
Secretional overlay on IA muscle (7 of 7)
A closer view, with unfortunately some secretional overlay, at least shows where the IA muscle would be found. Compare with photo 4.
IA-Only Paresis
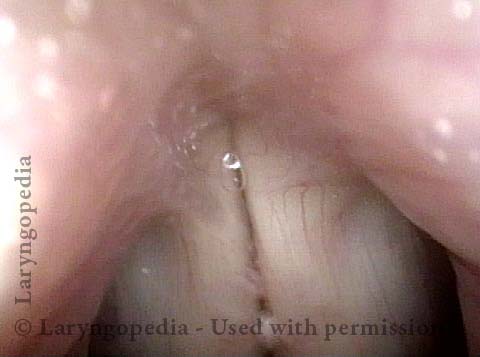
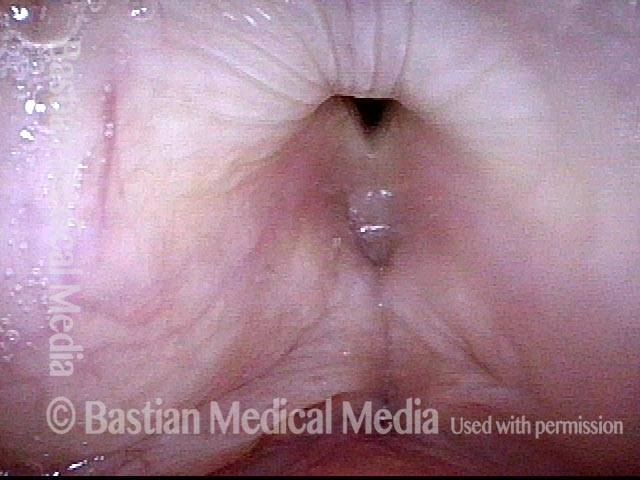
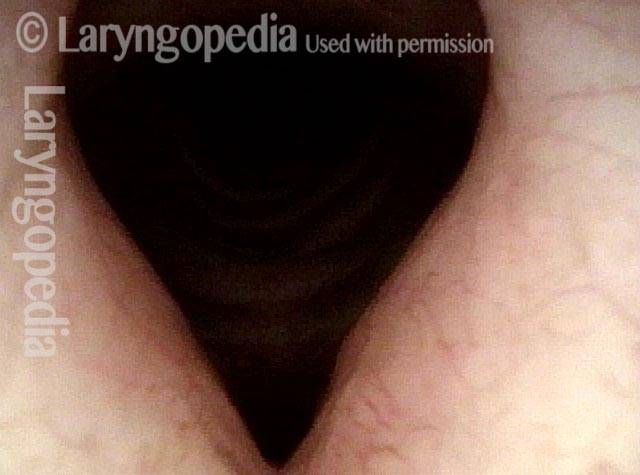
IA-only paresis (1 of 5)
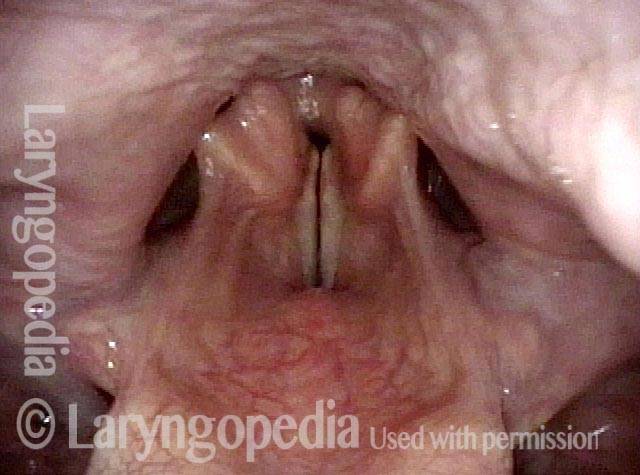
This patient describes his voice as being extremely weak with an abrupt onset that was unrelated to intubation or any other injury. The patient's voice sounds extremely breathy regardless of vocal task. The amount of bowing seen here cannot fully explain the breathy (air-wasting) dysphonia that is heard.
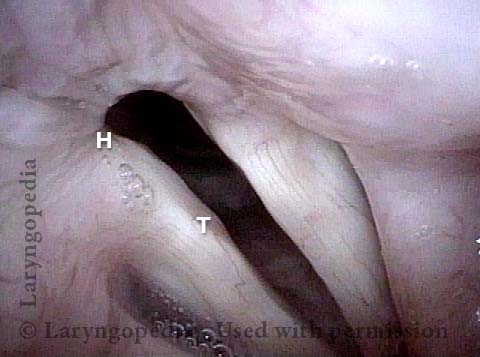
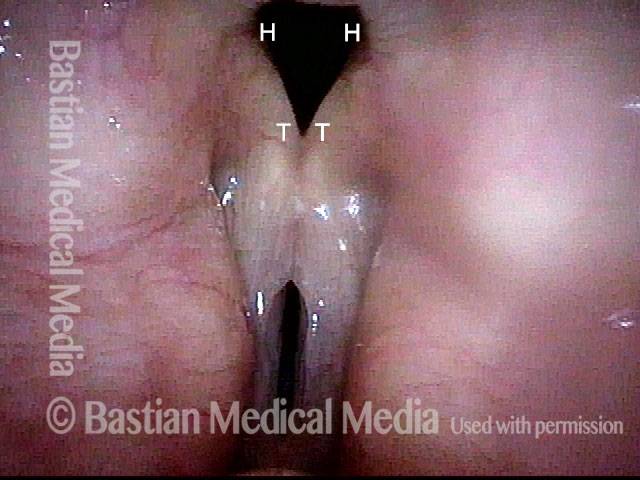
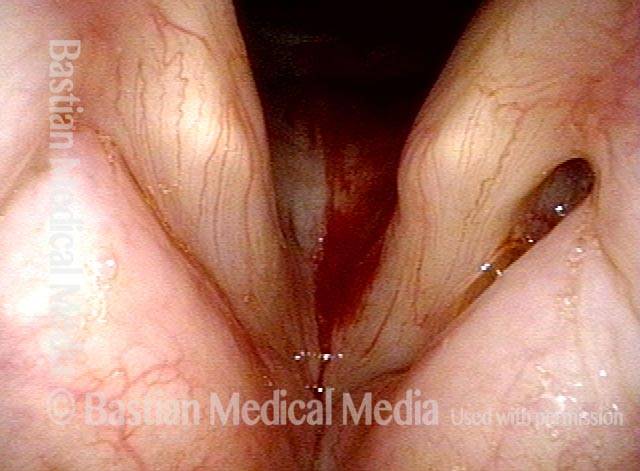
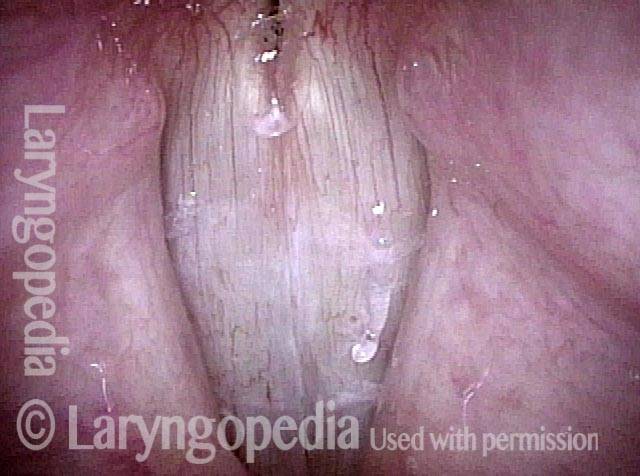
IA-only paresis (2 of 5)
An intense visualization of the posterior commissure begins to reveal the mystery. While the "toes" (indicated by each letter T), or vocal processes of the arytenoids, come into full contact, the "heels" (indicated by each letter H), or bodies of the arytenoid cartilages, do not.
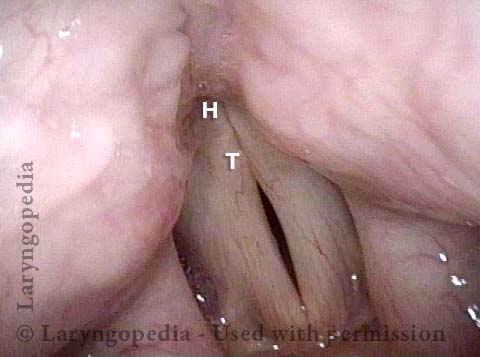
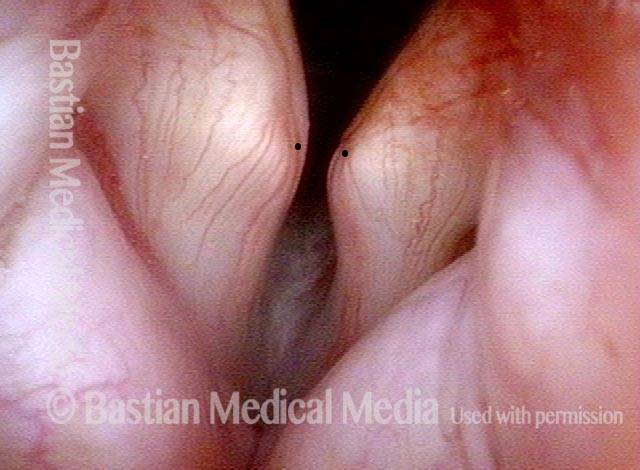
IA-only paresis (3 of 5)
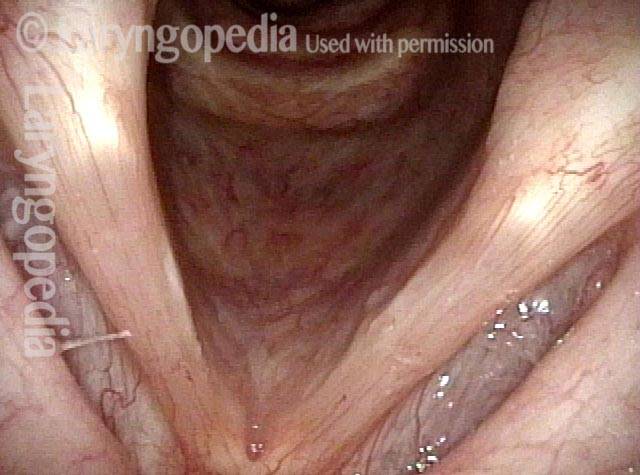
An even closer view shows the persistent posterior commissure gap.
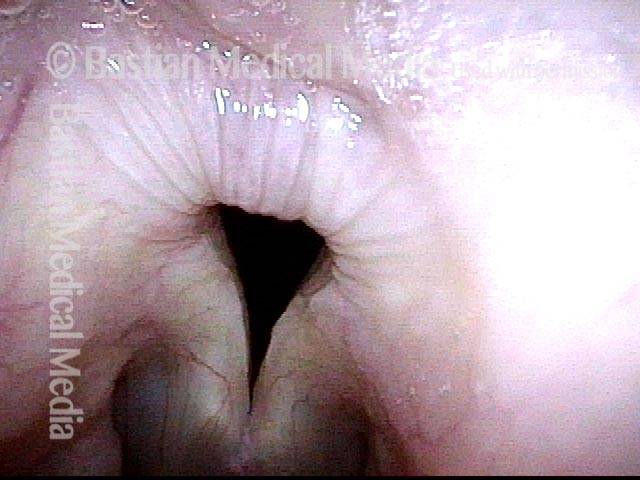
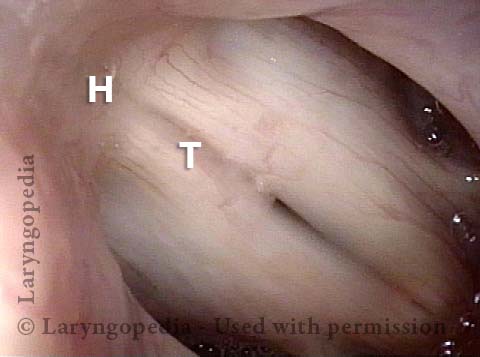
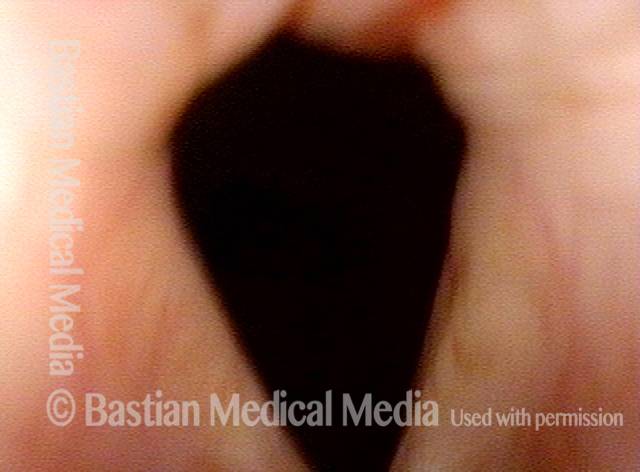
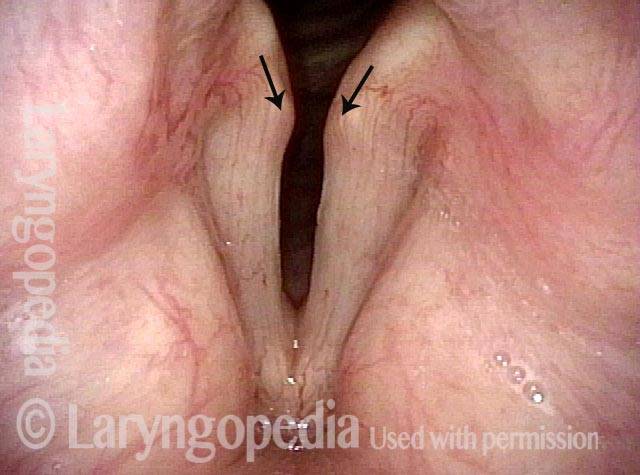
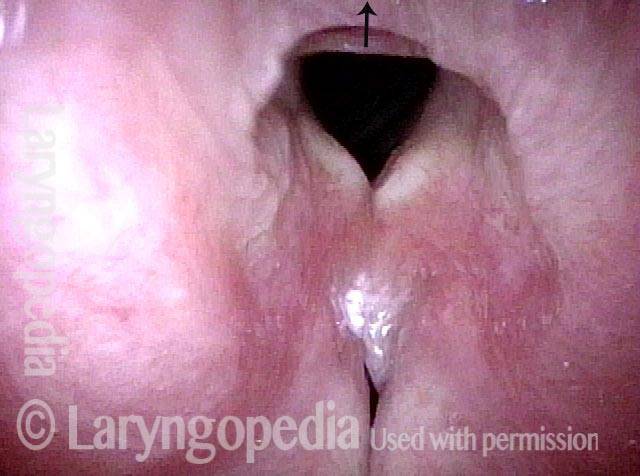
IA-only paresis, during a cough (4 of 5)
The elicited cough shown in this image proves that the patient is physically unable to close the posterior commissure.
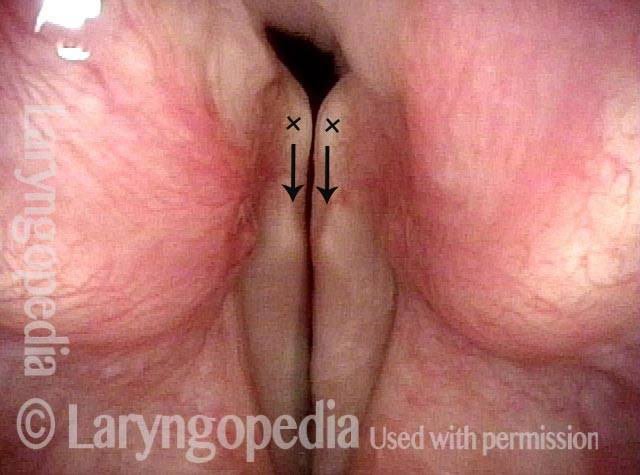
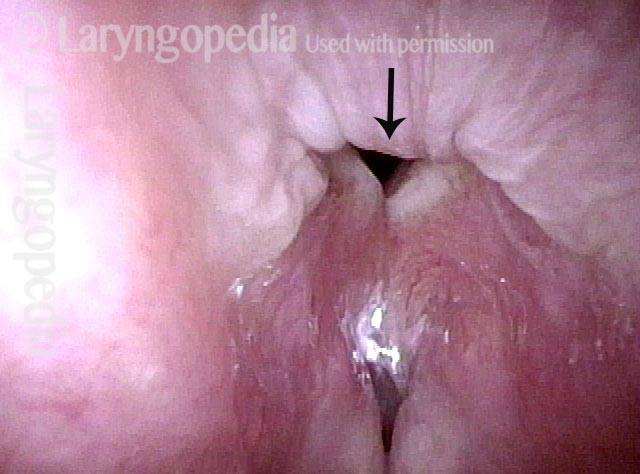
IA-only paresis, during a Valsalva maneuver (5 of 5)
An elicited Valsalva maneuver, which also fails to close the posterior commissure. High-resolution CT was performed to prove there was no abnormality of the cricoid or arytenoids which might account for this finding of apparent interarytenoid paresis or avulsion.

Interarytenoid (IA) Weakness
PCA muscles intact (1 of 4)
After SLAD-R surgery. The PCA muscles are intact, explaining normal abduction of both vocal cords for breathing.
Pre-phonatory instant (2 of 4)
At the pre-phonatory instant, one can see partial recovery of LCA muscles, explaining the ability of tips of vocal processes (at dots) to turn medially as the patient prepares to produce voice. Bowing is due to continuing TA weakness.
IA weakness (3 of 4)
The tips of the vocal processes (again at dots) are touching; the gap that remains posterior to them suggests that the interarytenoid muscle (IA) is not yet contracting sufficiently to bring the “heels” of the arytenoids together.

View of posterior commissure (4 of 4)
Very close-range view in the posterior commissure as the patient phonates, showing that the arytenoids do not come into contact. The tips of vocal processes are touching but out of view at the bottom of the photo (below the dots).
Another Interarytenoid (IA) Muscle Paresis or Is It Avulsion?
Breathy and weak voice (1 of 8)
Middle aged man with fairly abrupt weakening of voice with no explanation that occurred a year before this examination. Voice is very breathy, air-wasting, and weak. He also has a tendency to cough on liquids. Distant view at high pitch shows good vocal cord closure and symmetrical pharyngeal squeeze.
Bowing (2 of 8)
The abducted vocal cords for breathing show vocal cord bowing but otherwise nothing particularly noteworthy.
Pre-phonatory view (3 of 8)
As the vocal cords move towards each other on the way to producing voice, note the medial turning of the vocal processes (arrows), suggesting LCA muscles to be intact. The bodies of arytenoids, their “heels” as compared with the vocal process “toes” do not yet approach each other.
Phonatory view (4 of 8)
Now producing voice (see vibratory blur of the cords under this standard light) shows that vocal processes are in contact (arrows) but the ‘heels’ of the arytenoids still do not approximate. Is this nonorganic? Neurogenic? Orthopedic (cricoarytenoid joints)? Myogenic?
Posterior commissure (5 of 8)
Deep inside the posterior commissure during phonation. The large chink persists.
TA function (6 of 8)
Closed phase of vibration at B3 (247 Hz) shows good thyroarytenoid (TA) function.
IA mucosa (7 of 8)
The interarytenoid (IA) mucosa is blown away from the chink here by uncontrollable blast of air even while the patient tries to Valsalva /breath hold. Tight closure of not only true, but also false cords verifies his level of effort.
IA avulsion (8 of 8)
During same Valsalva maneuver 1/5th of a second (6 frames) later, the interarytenoid mucosa has oscillated anteriorly (arrow). Why can’t the arytenoid “heels” come together? The best thought here is interarytenoid avulsion which could have sudden onset. Denervation seems possible but less likely given presumed bilateral innervation of that muscle, and a bilaterally symmetrical joint problem of rapid onset also seems unlikely.
Watch the Progression of A Rare Laryngeal Paresis Scenario Including Interarytenoid (IA) Muscle
Full abduction (1 of 5)
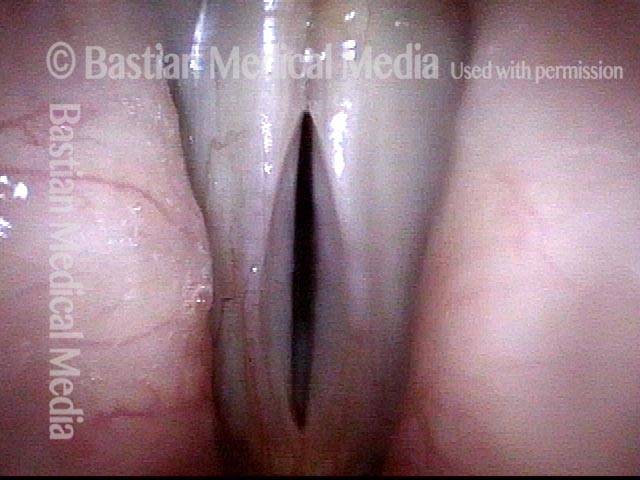
Three months ago, this otherwise healthy woman experienced an abrupt change in voice. The vocal phenomenology is that of weakness and air-wasting. Here, in full abduction, the vocal cords look slender and the whitish lesion of the right cord (left of photo) is a red herring finding. (Compare with Photo 3.)

Large gap during phonation (2 of 5)
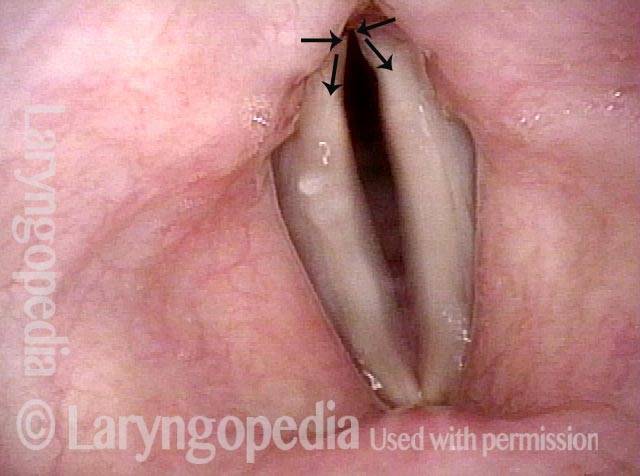
During phonation (note blurring of the vocal cord margins), there is a large gap between the cords. Interarytenoid muscle seems to be functioning, in that the “heels” of the arytenoids come into quite good contact (horizontal arrows, above). The tips of vocal processes, or “toes” of the arytenoid cartilages, point laterally, (diverging arrows, below) suggesting LCA weakness. (Compare with photo 4.)
Two months later—voice is even worse (3 of 5)
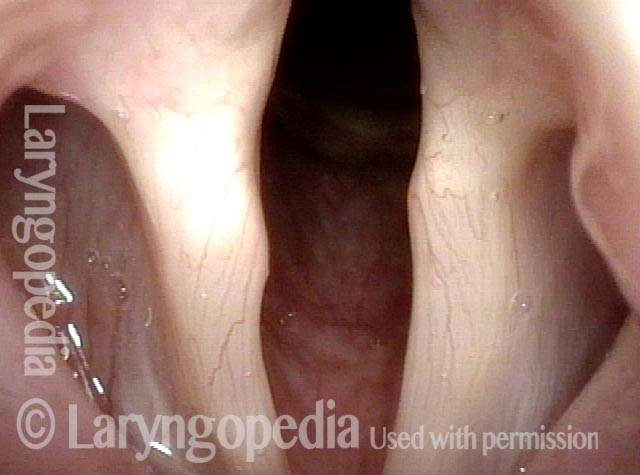
Two months later, the patient reports that her voice is even worse. Note that while breathing, the vocal cords appear to be hyper-abducted. It is as though more of the ability to adduct (come together) has been lost; put another way, that abduction is less “balanced” by any tone from adductory (voicing) muscles. (Compare with photo 1.)

Arytenoids no longer touch (4 of 5)
Here, at the prephonatory instant, just before vibratory blurring commences, notice that the heels of the arytenoids no longer touch. It is as though IA muscle is denervated. (Compare with photo 2.)
Breathy voicing (5 of 5)
Extremely breathy voicing has commenced. Note the blurring of the right cord margin (left of photo). If anything, the posterior glottis is even farther apart. Radiographic/diagnostic questions: Is there a mass lesion anywhere? No. Is the cricoid cartilage deformed? No. What is causing this? Unknown.
