LCA-only paresis refers to weakness or paralysis of the vocal cord’s lateral cricoarytenoid (LCA) muscle, but with normal function of the vocal cord’s other muscles. The LCA muscle helps to bring the vocal cord to the midline for voice production and, more specifically, to bring the “toe” of the arytenoid cartilage to the midline.
The following are indicators of LCA-only paresis:
- Movement: The vocal cord opens normally for breathing. From a distance, it can appear to close normally for voicing, but more acute and up-close inspection often shows a faint lag or reduction of crispness of approach to the midline, and inspection of the posterior commissure at close range shows that in fact it does not fully adduct.
- Position and appearance: Position is normal during breathing, but again, the vocal cord does not come fully to the midline for voicing. A tell-tale indicator of LCA-only paresis is lateral turning of the vocal process. This lateral turning is seen best in low voice, and is a little less apparent with very high voice (as illustrated by a pair of photos below).
- Appearance during voicing (under strobe lighting): Persistent slight gap between the vocal cords posteriorly, with the laterally turned vocal process, but no flaccidity of the cord with vibration. Normal tone and bulk of the vocal cord itself.
- Voice quality: Weak and air-wasting, but without the luffing and diplophonia often apparent when the thyroartyenoid (TA) muscle is also paralyzed.
LCA Weakness
Lateral cricoarytenoid (LCA) weakness is best seen during phonation. Lateral turning of the vocal process during voicing is the “key” finding, though there are others. We say the “toe” (tip of vocal process) is turned laterally. The “heel” of the arytenoid is together, signifying normal function of the interarytenoid (IA) muscle.
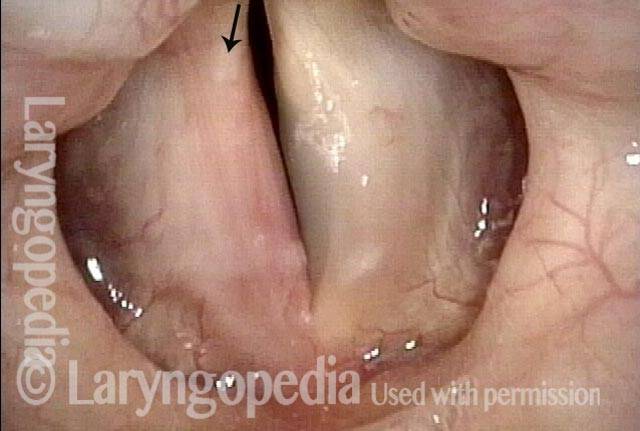
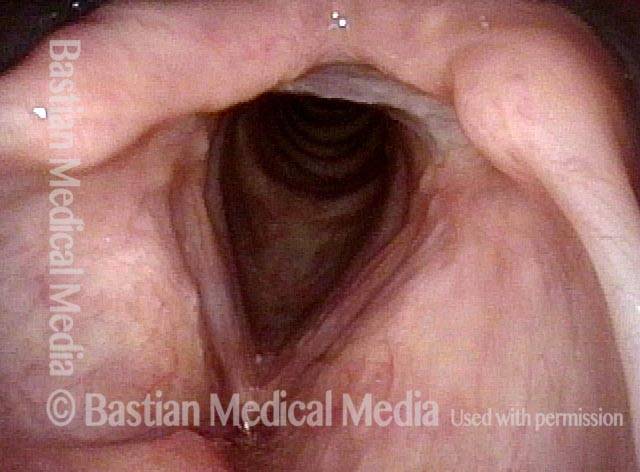
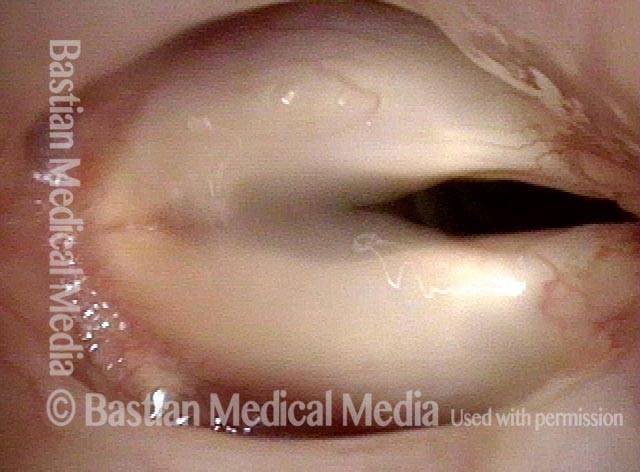
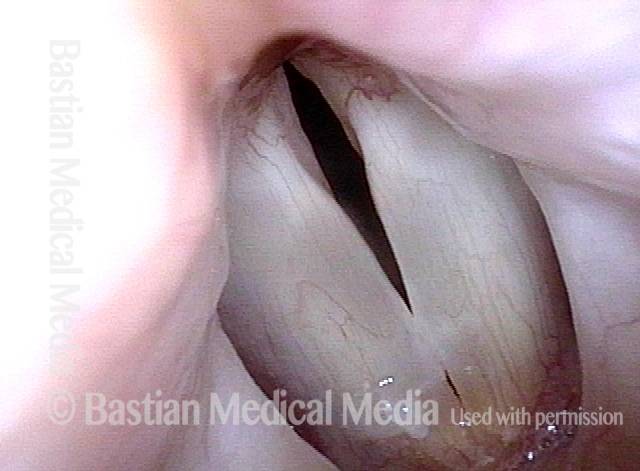
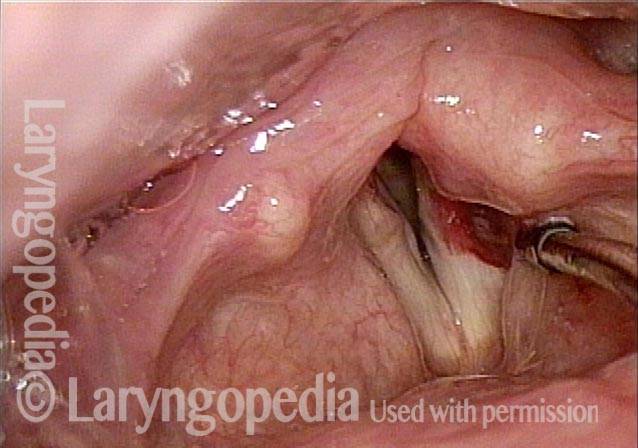
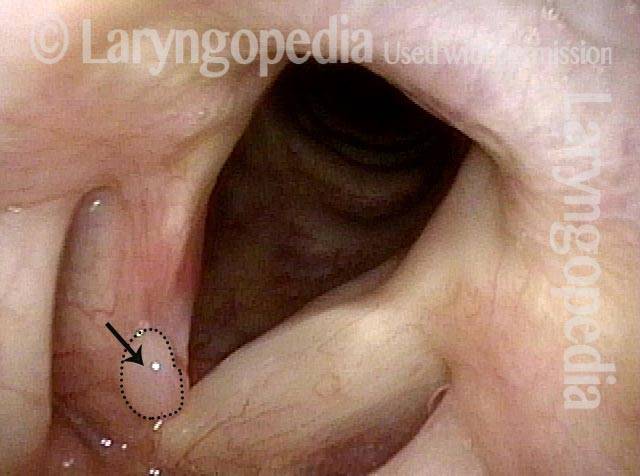
LCA weakness, in a patient with vocal cord paralysis (1 of 4)
Phonation in the low chest register (note the wide zone of vibratory blurring). Here, the vocal process is clearly seen to turn laterally (arrow), a tell- tale indicator of LCA weakness. As other views of this particular patient would indicate, she actually also has weakness of the TA and PCA muscles, not just LCA-only paresis, but this view alone would correspond to a patient who had LCA-only paresis.

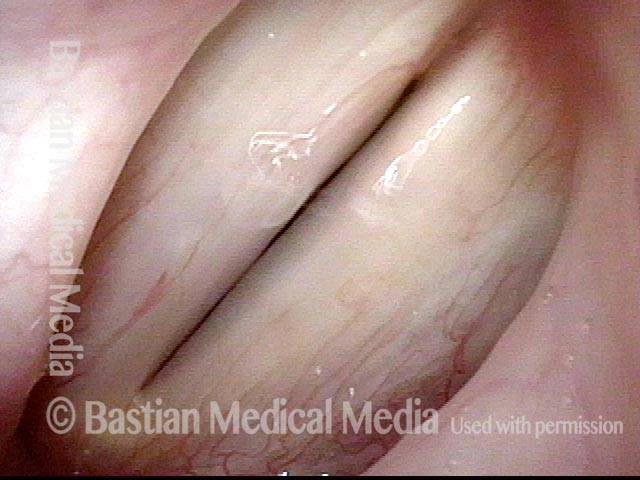
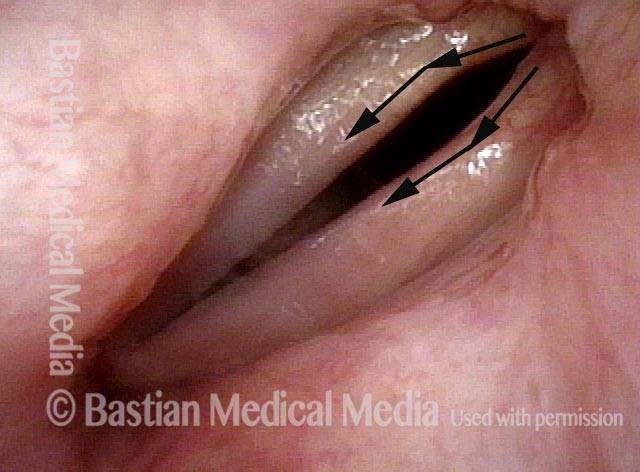
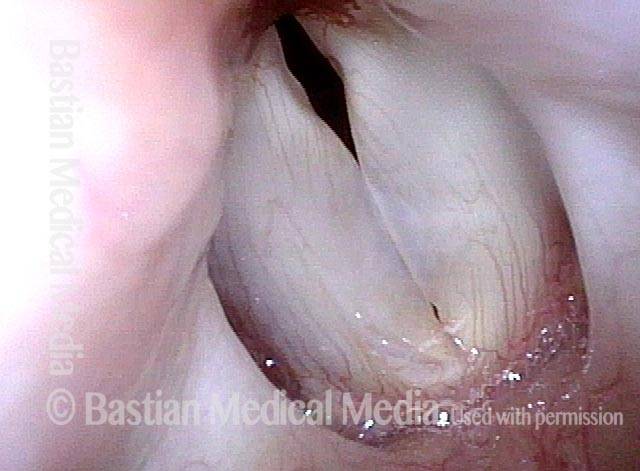
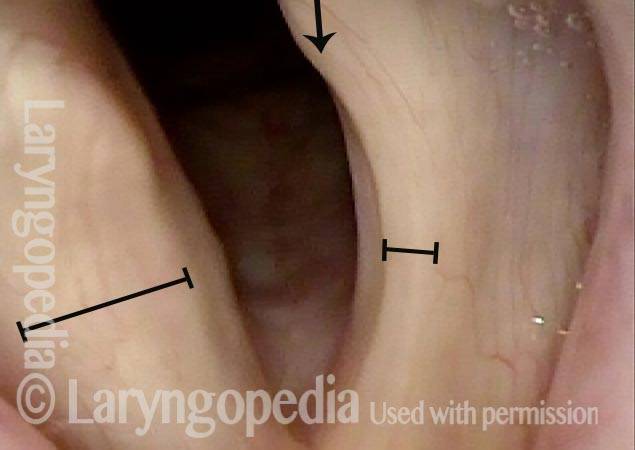
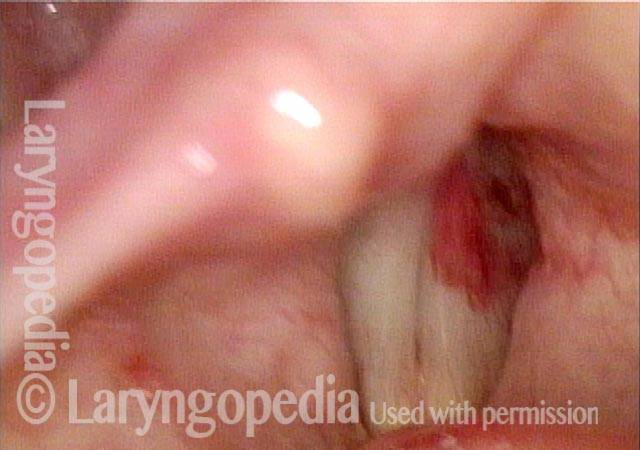
LCA weakness, masked by high pitch (2 of 4)
Phonation at very high pitch (as expected, the vibratory blur narrows). The antero-posterior lengthening of the left cord (right of image) at this high pitch turns the vocal process on that side back towards the midline (compare with photo 1), masking the LCA weakness. This low voice/high voice difference in the posterior commissure is routinely but not universally seen with LCA weakness.
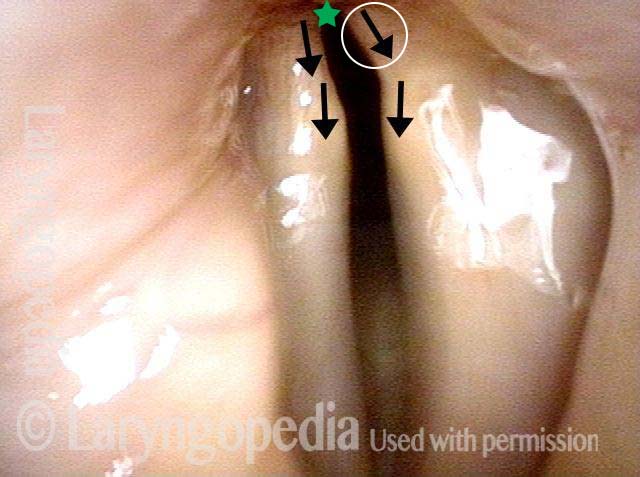
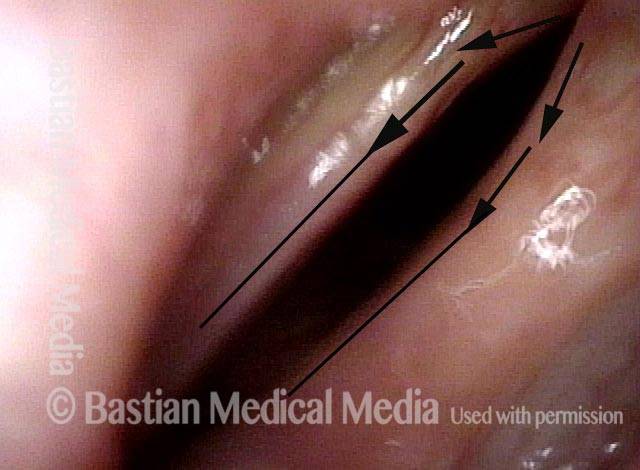
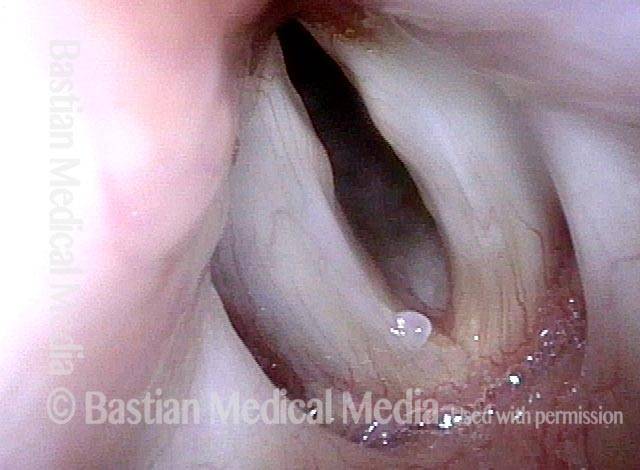
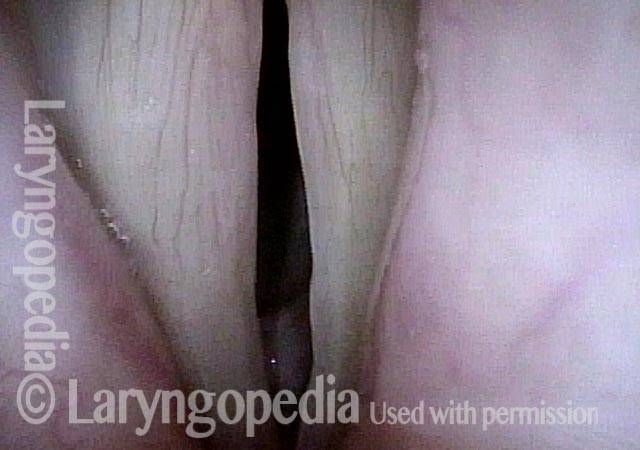
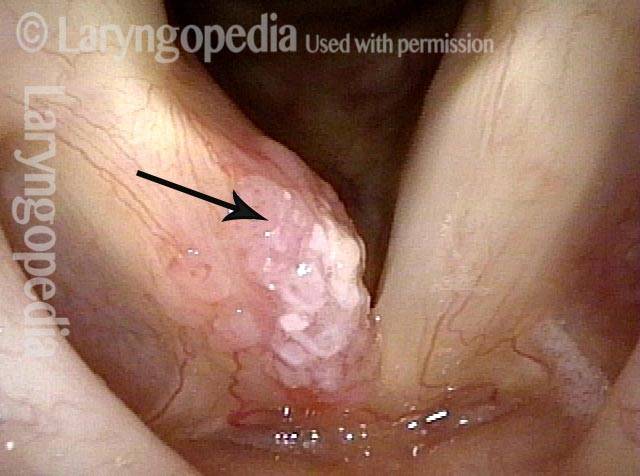
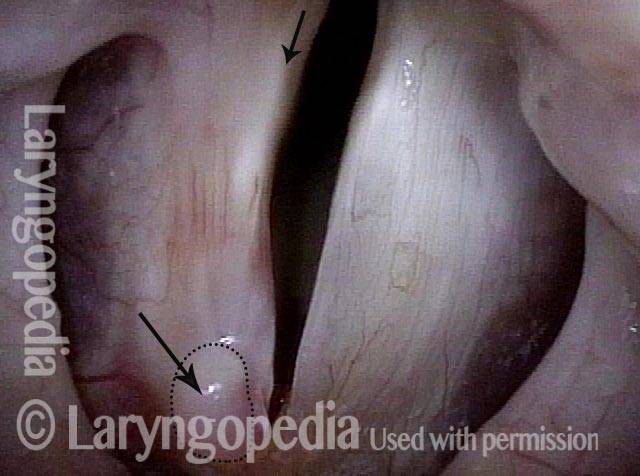
Imposed breathy voice (3 of 4)
Low pitch exaggerates the key finding of lateral turning of the vocal process (circled arrow). Notice that both cord margins are blurred and there is a large gap between the cords. The person is therefore phonating here with an “imposed” breathy voice due to lack of glottic closure caused by the lateral turning of the vocal process. Though barely inside this photo, the “heels” of the arytenoids are together, signifying normal IA function.
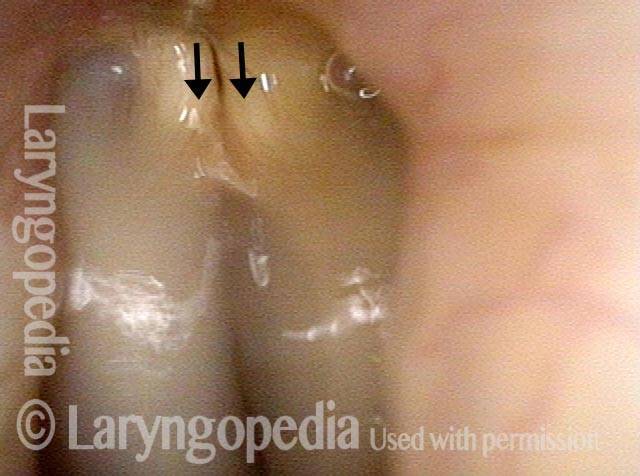
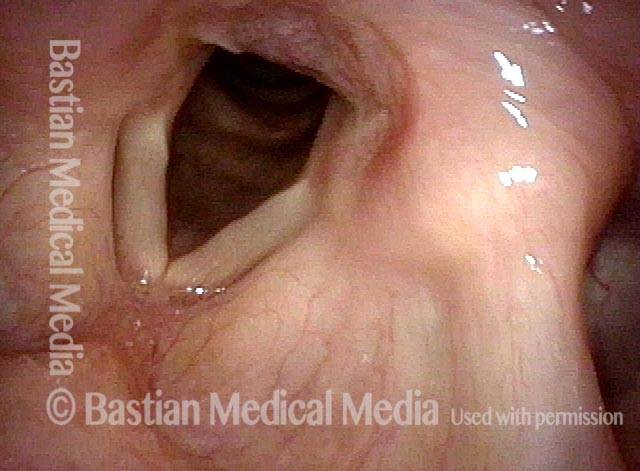
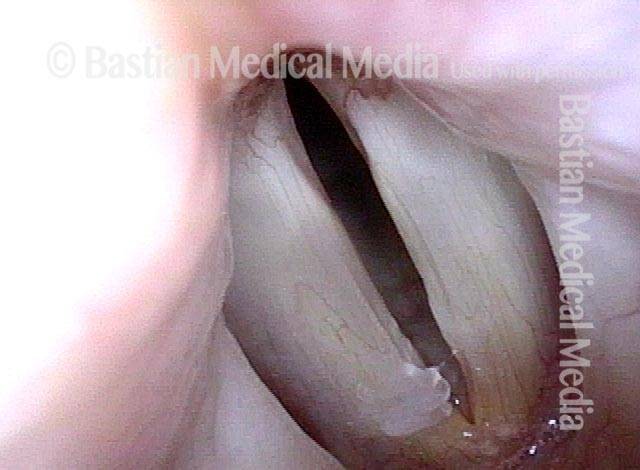
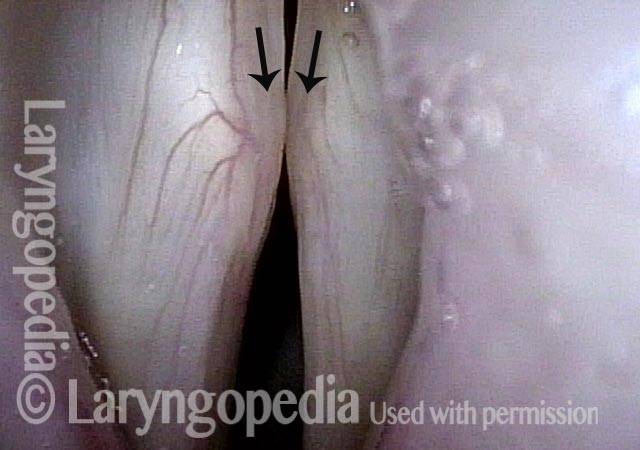
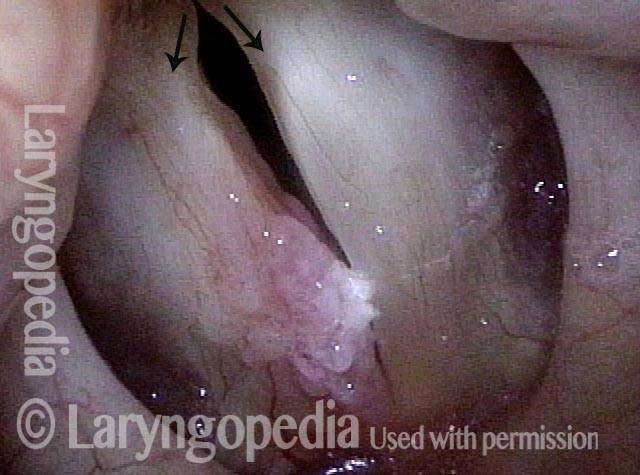
LCA paresis has recovered (4 of 4)
Several weeks later, this person’s voice recovers fully. The explanation? The LCA paresis has recovered. Note that both vocal processes align (arrows) and the “toes” of the arytenoids are together, as are the “heels.”
Bilateral LCA Weakness?
Weak, air-wasting voice (1 of 4)
Forty-something tradesman who developed weak voice abruptly after an upper respiratory infection, but that was more than a year prior to this examination. Panoramic view during breathing shows some inflammation but the voice quality is of air-wasting, not laryngitis.
Pre-phonatory instant (2 of 4)
A closer view at the pre-phonatory instant of D4 (~294 Hz). The posterior-most arytenoid surfaces are in contact, but the vocal processes turn a little bit laterally, and this seems to account for the gap between the cords. This is not typical bowing.
Phonatory blurring (3 of 4)
At G3 with phonatory blurring, the cords are shorter, but the lateral turning and posteriorly-shifted “pseudo-bowing” remains.

Bilateral LCA weakness (4 of 4)
At even lower pitch, E3 (~165 Hz), the remarkable gap is again seen to originate primarily from lateral turning of the tips of the vocal processes, suggesting bilateral LCA weakness.
Severe MTD or Bilateral LCA Weakness?
Breathiness (1 of 6)
Older middle-aged woman with a great deal of breathiness creeping into her voice, despite good training and long singing experience. Here, in breathing position, the vocal cords look fairly normal.
Phonation (2 of 6)
At closer range during phonation at G3, note that the vocal processes are both turned slightly laterally. The membranous folds are blurred due to vibration.
Closed phase (3 of 6)
As seen under strobe light during closed phase of vibration at G3 (196 Hz), the lateral turn of the vocal processes is again seen.
Open phase (4 of 6)
Open phase at the same pitch.
Large gap (5 of 6)
At the higher pitch of G4 (392 Hz), note the lengthening of the vocal cords, which often turns vocal processes a little bit more to the midline, but they remain distinctly turned laterally, explaining the large gap.
Open phase (6 of 6)
Open phase at the same pitch. This appears to be bilateral LCA weakness given relative abruptness of onset in a highly trained and experienced singer. Why this happened is unknown.
Paresis Visual Taxonomy Can Be Trusted, But Is This Taking the LCA Cue Too Far?
Post carotid endarterectomy (1 of 7)
Immediately after carotid endarterectomy a few weeks earlier this voice was drastically altered due to left vocal cord “paralysis” — actually paresis as we shall see. Note that the left cord (right of photo) is bowed and atrophied (spaghetti-linguini sign). TA muscle is definitely wasted. Curiously, the left vocal process almost appears straight or faintly medial-turning (arrow), suggesting preserved LCA action.
PCA muscle (2 of 7)
The lack of abduction of left vocal fold (right of photo) signifies the left PCA muscle isn’t working.

Maximum closure (3 of 7)
Maximum closure during strobe examination. Neither side has enough recoil to oscillate back to midline. This person is elderly.
Open phase (4 of 7)
At the same pitch but open phase of vibration. Neither side has significantly greater lateral amplitude. The LCA question (at ?) generated by photo 1 cannot yet be answered, because the expected lateral turning of the vocal process is unable to be evaluated. See the next photo.

LCA muscle (5 of 7)
With view directed to the posterior commissure, the vocal processes can be identified and left LCA does indeed appear to be working. That is, it is not turning laterally, as it would be if LCA were out. Can it be that PCA and TA are out, and LCA working? Watch for future examination photos…
Voice gel injection (6 of 7)
Voice gel injection in progress, with needle inserted into the left paraglottic space.
Phonation (7 of 7)
Producing voice after gel injection, there is no gap in the posterior commissure contrary to expectation if LCA were not functioning on the left. This might also explain why voice result after voice gel is better than expected when treating paralysis.
Evolution of the Wound After Laser Removal of a Vocal Cord Cancer: Not Pretty at First, but Voice Result Can Be Very Good
Vocal cord cancer (1 of 8)
Bulky but superficial right vocal cord cancer (arrow, left of photo).
Voice-making with tumor (2 of 8)
Voice-making position. Notice the more lateral turning of the right vocal process (left of photo) as compared with the left (right of photo). As the remaining series shows, it is impossible to know if this is compensation for the bulk of tumor, or weakness of the LCA muscle.
One week post-removal (3 of 8)
A week after definitive removal, swelling, early granulation, and a division of the wound into upper and lower “lips” that must bind together with healing.

Voice-making, post-removal (4 of 8)
Note again the lateral turning of right vocal process (arrow, left of photo).

Six weeks post-op (5 of 8)
Six weeks after surgery, the wound is “bound together,” and there is a residual granuloma on the upper surface anteriorly (arrow).
Voice-making, post-op (6 of 8)
Making voice, there is still that peculiar lateral turning of the vocal process on the right (left of photo).
Four months post-op (7 of 8)
Now a full 4 months since laser excision, the cord is fully healed though still pink as expected. The anterior upper surface is coated with mucus.

Voice-making, four months post-op (8 of 8)
Making voice, again that lateral deviation of the right vocal process (arrow, left of photo). Voice is very functional but a little weak. Vibratory blur is greater for left than right cord.