Introduction
Spasmodic dysphonia (SD) is a neurological voice condition that diminishes voice/speech intelligibility and markedly increases the effort to talk. The impact on social life and occupation can be devastating. Untreated patients may even lose their jobs.
There are two primary variants—adductory SD (~90%) and abductory SD (~10%). For the AD-variant, the voice cuts out or squeezes down to a strangled quality, so that syllables or words are lost. For the AB-variant, the voice intermittently and unpredictably drops out to a whisper, again losing syllables or words. The pattern of spasms varies greatly both between and within those affected. For this reason, individualization of treatment is paramount.
Target Muscles and Dose Varies
Due to the difference between the AD- and AB-muscle spasms, the target muscles are different for the two subtypes. There is also variation of severity, presence or absence of tremor, and sensitivity to botulinum toxin. The dose for one patient may easily be 10 times or more that used for another one.
Frequency of Injection Differs Between Patients
Also, crucially, each patient’s usual rate of “metabolism” of the botulinum toxin is specific to them. While the average duration of benefit might be 14 to 16 weeks, there are a fortunate few who can obtain very good results for 20 weeks. And there are the unfortunate few who metabolize so quickly that they are injected as often as every 8 weeks. Furthermore, patients occasionally choose a partial dose because of an upcoming event (reunion, speech, work presentation), understanding that the next injection will be needed sooner than usual.
Potential Impediment to the Freedom to Individualize
A few weeks ago, proposed changes to Medicare requires medical practitioners to enforce a minimum interval of 12 weeks between injections, drastically limiting the flexibility available to the patient in receiving quality care. Two big examples of how this would hurt patients:
- It would limit covered access for a subset of patients who are rapid metabolizers, needing injections every 8 or 10 weeks, for example.
- From time to time, a patient who needs an earlier injection than their usual 12+ weeks would be denied covered access, too.
If unable to pay out of pocket for uncovered injections (about $650 at Bastian Voice Institute and far more costly in many other clinics), as many as 10 or 20% of patients will spend part of each year untreated, and suffering.
Consider 4 Actual Patient Scenarios…
Patient Example 1
A first-grade teacher with AD-SD receives botulinum toxin injections that allow her to continue her profession. Her longstanding pattern, however, is as follows: The voice is breathy but functional for a couple of weeks; voice is very much improved for 5 weeks. And then spasms return with a vengeance, beginning just 7 weeks after the injection.
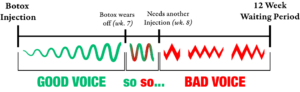
Despite taking this patient to the maximum dose she can tolerate (due to initial breathiness side effect), her spasms routinely return abruptly and nearly completely after only 8 or 9 weeks. Accordingly, for the six years since her diagnosis, she has been coming for re-treatment every 8 weeks.
If the wait between injections must be at least 12 weeks, this patient would have to pay for every other injection. Alternatively, she could go essentially untreated for a one month out of four, making teaching extremely difficult to impossible during those months, while she waits for the final four of the 12-week requirement to pass.
Patient Example 2
A young woman with SD is to be married. As the date approaches, she realizes that spasms will be noticeable for the festivities. She comes per her routine at 14 weeks, but since the wedding is only 2 weeks away, she requests a half-dose, so that she will go directly to good voice and skip the usual initial breathiness side effect.
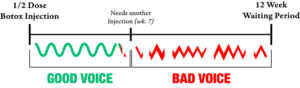 This works very well for the wedding, but just 7 weeks later she is, as expected, ready for another injection. She is forced to wait 5 weeks with a terrible voice until the 12-week requirement is met.
This works very well for the wedding, but just 7 weeks later she is, as expected, ready for another injection. She is forced to wait 5 weeks with a terrible voice until the 12-week requirement is met.
Patient Example 3
A patient has been receiving very successful injections every 16 weeks for 20 years. She has been extremely happy with the results. But after her most recent injection with her usual dose, she says she had very little breathiness and went straight to the “golden period” of voice. (Targeting is a challenge for her particular anatomy, and despite a good EMG signal, the placement must have been suboptimal. This happens every 80 injections or so, even when done by skilled and experienced physicians.)
 But now, at ten weeks, spasms are very evident, and she has an important Zoom call she must lead with international customers of her business. She is angry and frustrated that she must pay for an “early” injection, or choose to lead the crucial sales event with a strained and effortful voice.
But now, at ten weeks, spasms are very evident, and she has an important Zoom call she must lead with international customers of her business. She is angry and frustrated that she must pay for an “early” injection, or choose to lead the crucial sales event with a strained and effortful voice.
Patient Example 4
A longstanding patient, treated successfully at approximately 15 week intervals for 25 years, has moved to another state. She received an injection there just 3 weeks ago, but nothing happened. She got no benefit at all. She has returned to the area to visit her sister and requests an injection, since her spasms are in full force.
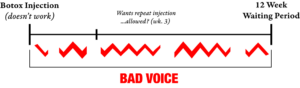
She learns that she has no coverage and must pay out of pocket for this extra injection or she must suffer vocally for another 9 weeks, waiting for the full 12-week interval to elapse, even though there was no response to the out-of-state injection.
Conclusion
Due to one-size-fits-all treatment mandates, patient and clinician freedom to meet the demands of outlier circumstances is removed. This means a reduction of the quality of care for many patients.
Imagine by analogy being told “you can’t wear your glasses for the next month,” or “Sorry, you must take your hearing aids out for the next five weeks,” or “Sorry, you can’t use your wheelchair (or cane, or insulin or blood pressure medicine) for the next few weeks.” Such a structured and rigid treatment schedule applied to a variable disorder would leave a subset of people with SD sidelined socially and vocationally purely due to refusing them medically necessary care—unless they were able to pay for this expensive treatment themselves.