La leucoplachia (leuko = bianco; plakia = placca) è una macchia bianca che si trova sulla mucosa in qualsiasi parte del corpo. Nella laringe, si osserva più spesso sulle corde vocali, sia nei fumatori di lunga data che in individui con qualche altra causa di infiammazione cronica, come (controverso) il reflusso acido.
È il termine visivamente descrittivo per quello che, alla biopsia, potrebbe rivelarsi cheratosi, carcinoma in situ o carcinoma. Sfortunatamente, la leucoplachia è un problema persistente e frustrante in laringologia, con la tendenza a ripresentarsi dopo la rimozione.
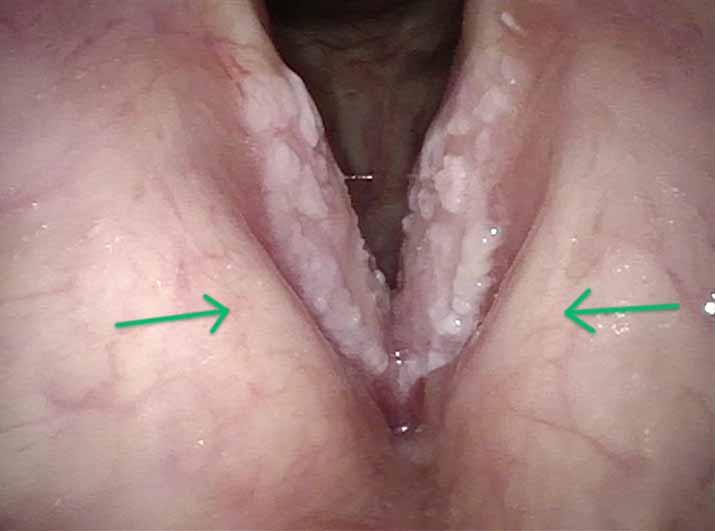
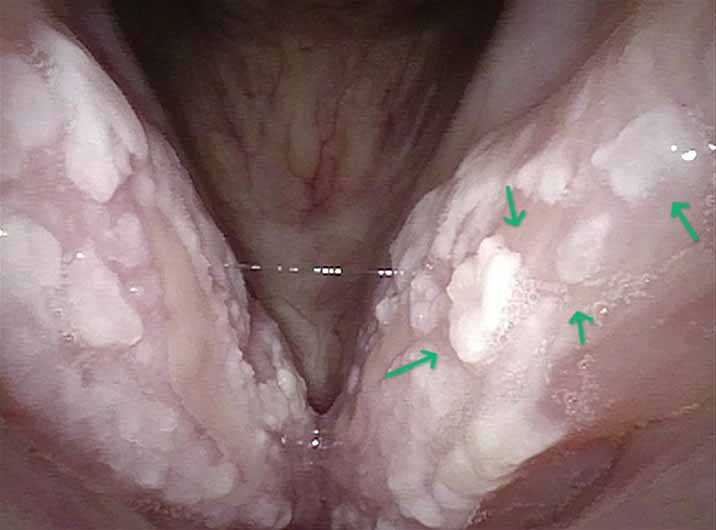
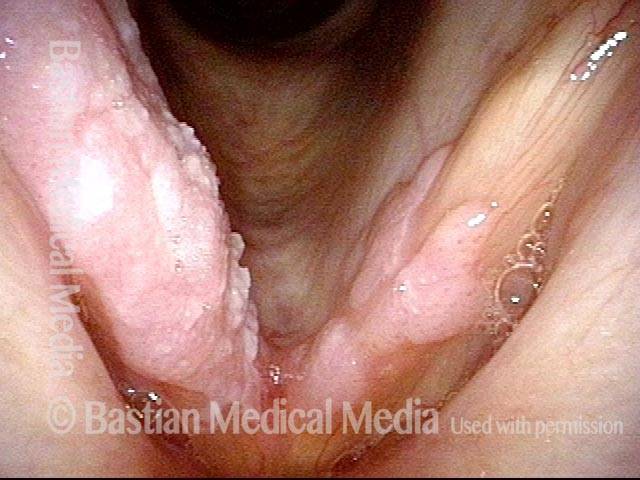
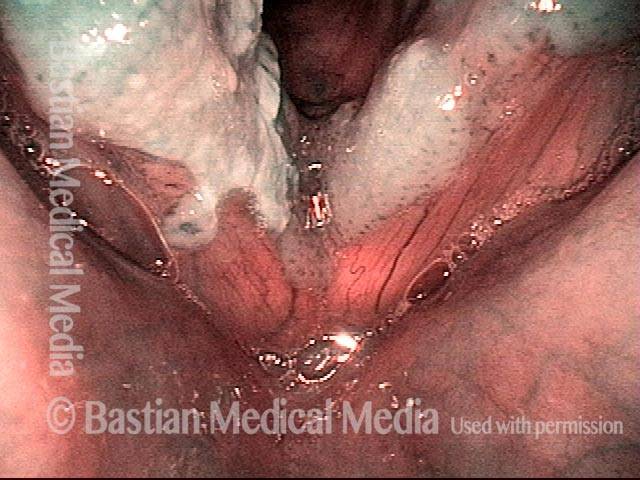
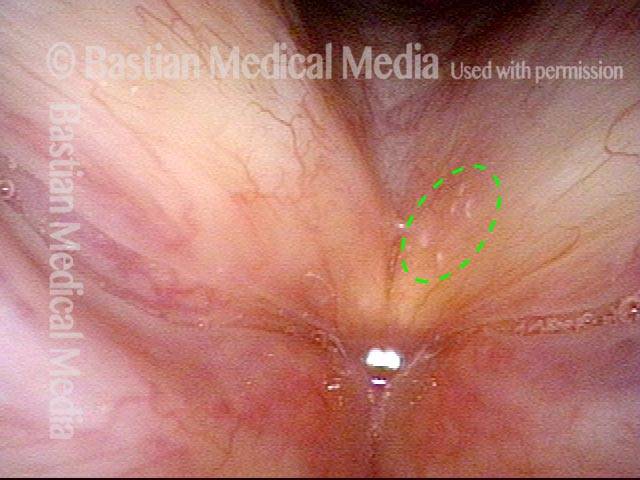
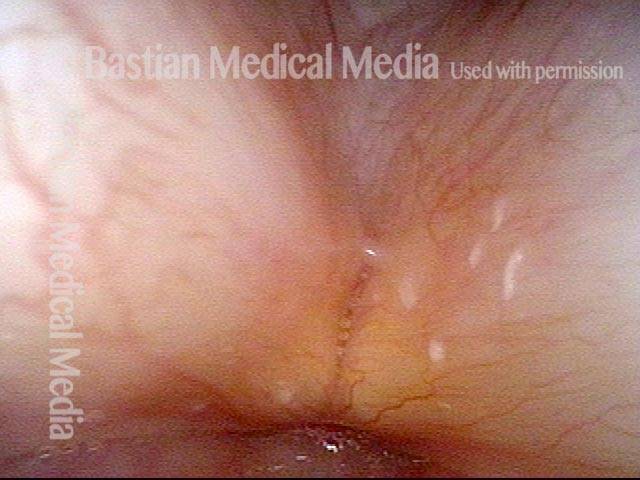
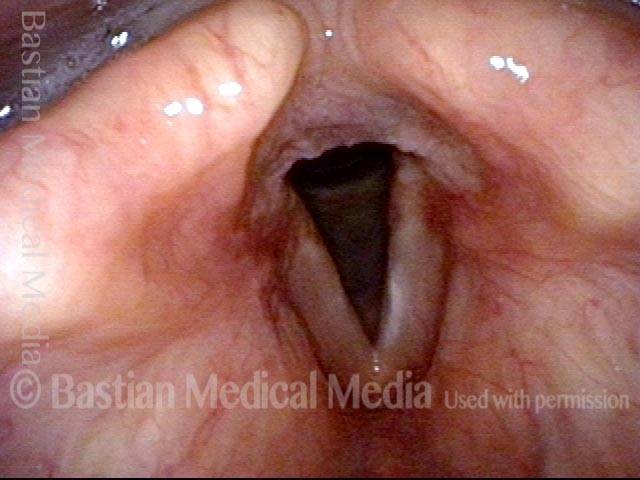
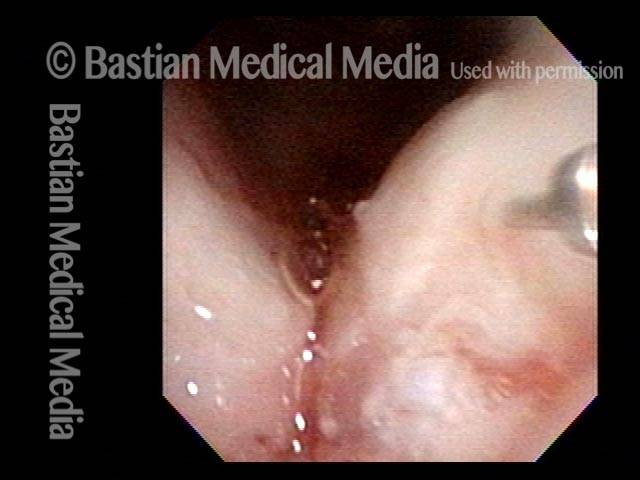
Glassa per torta e latte versato Leucoplachia post Covid in un ex fumatore
Si tratta di una persona che fumava ½ pacchetto al giorno per poco più di un decennio ma aveva smesso quasi 15 anni fa. La voce è stata sempre normale fino all’infezione da Covid-19 (nonostante la vaccinazione). Durante quella malattia si è verificata una laringite che non si è mai risolta nei sei mesi successivi al momento di questo esame. È rauco ma la voce è funzionale alla comunicazione di base.
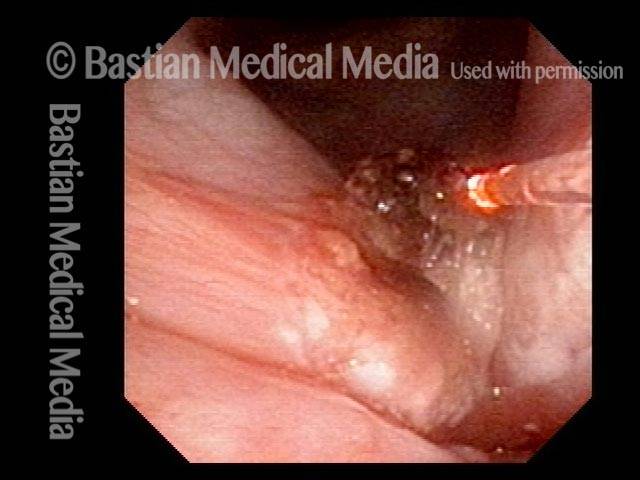
Dopo che i trattamenti di supporto (reflusso acido, ecc.) non sono riusciti a risolvere queste lesioni, seguirà la microlaringoscopia con meticoloso peeling della “membrana basale” di queste lesioni.
Leukoplakia (1 of 7)
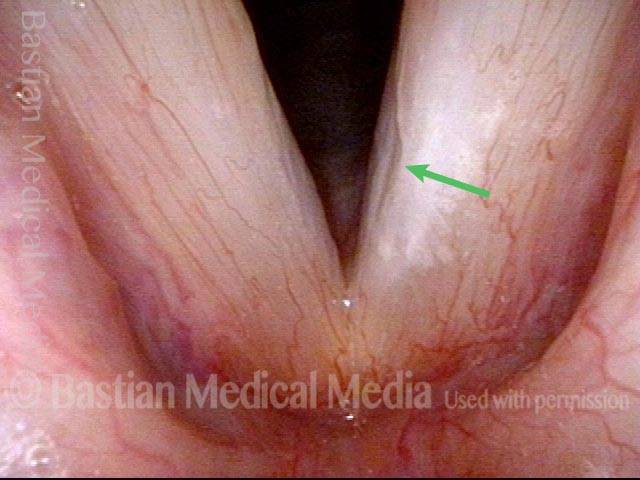
Spilled milk Leukoplakia (2 of 7)
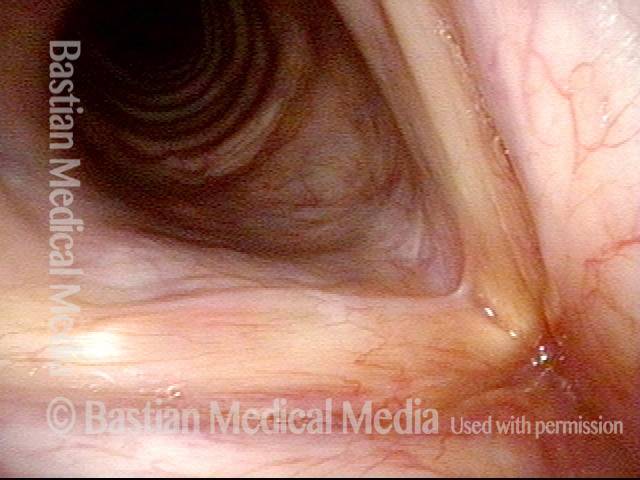
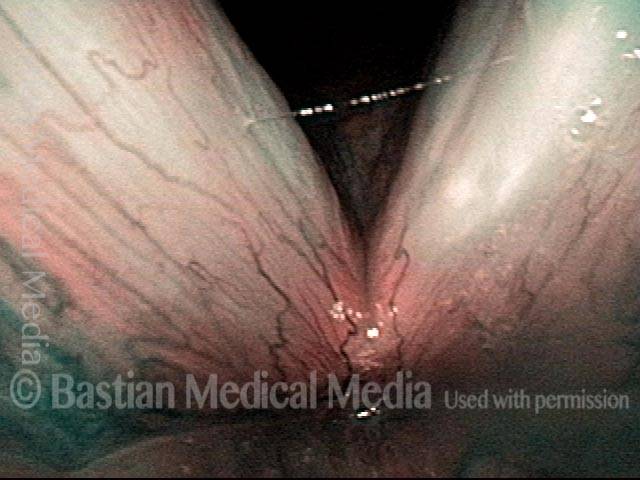
Superficial ulceration (3 of 7)

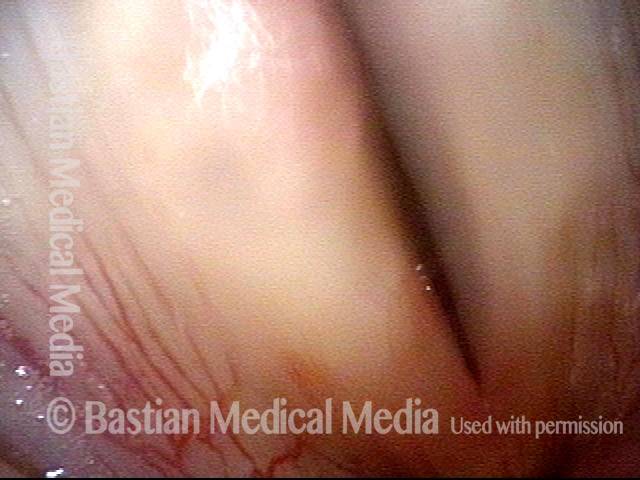
Closed phase of vibration (4 of 7)

Stiff mucosa limits vibration (5 of 7)

Leukoplakia diminishes (6 of 7)

Residual leukoplakia (7 of 7)

Altri esempi di leucoplachia
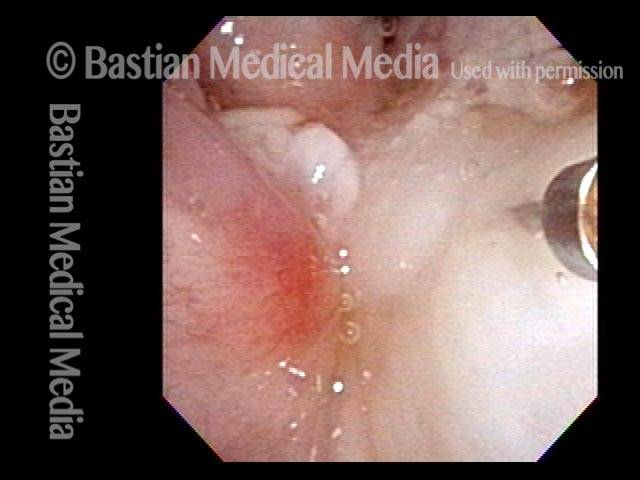
Cake-icing Leukoplakia (1 of 4)
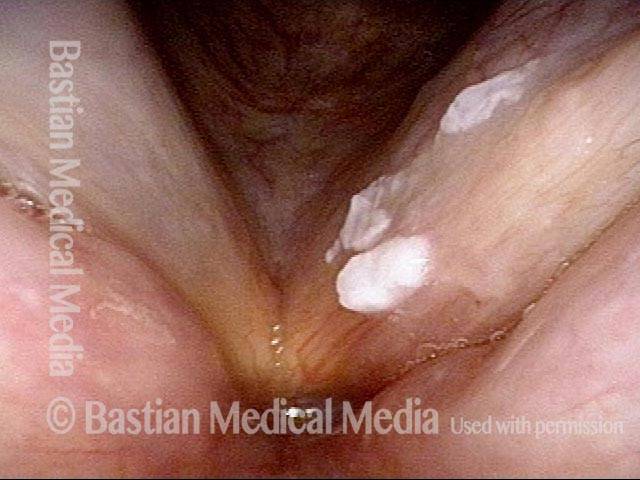
Hazy Leukoplakia (2 of 4)
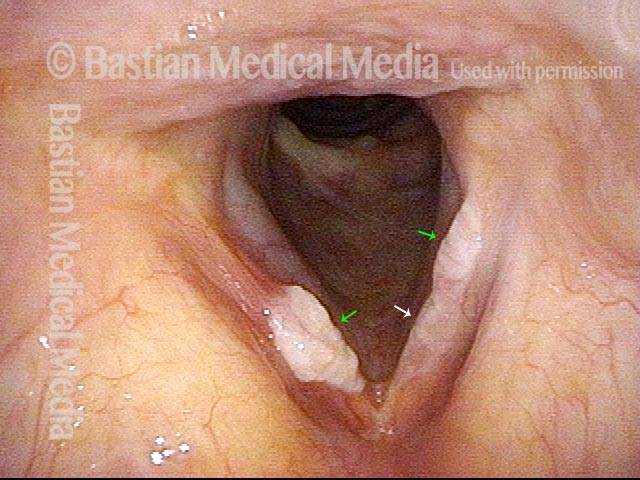
Leukoplakia (3 of 4)

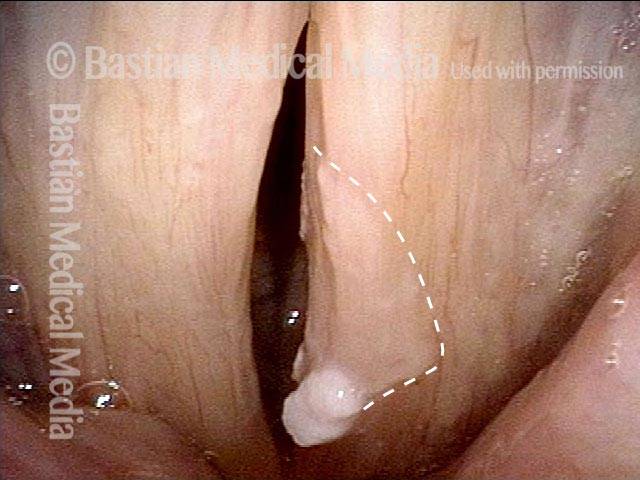
Closer look (4 of 4)

Esempio 2
Leukoplakia (1 of 2)

Leukoplakia (2 of 2)

Leucoplachia, prima e dopo la rimozione chirurgica
Diffuse Leukoplakia (1 of 4)
HPV effect (2 of 4)
Leukoplakia, after surgical removal (3 of 4)

Leukoplakia, after surgical removal (4 of 4)

La leucoplachia ha combattuto nel tempo
Leukoplakia (1 of 8)
Spilled Milk (2 of 8)

Thulium laser (3 of 8)
Coagulated tissue (4 of 8)
Leukoplakia (5 of 8)

Detachment (6 of 8)
Superficial vascular pattern (7 of 8)
Coagulated tissue (8 of 8)

Leucoplachia, prima, durante e dopo la coagulazione laser
Leukoplakia, not yet seen (1 of 6)
Leukoplakia (2 of 6)
Leukoplakia (3 of 6)
Leukoplakia, coagulated by laser (4 of 6)

Leukoplakia, 3 months after laser treatment (5 of 6)
Leukoplakia, 3 months after laser treatment (6 of 6)
Noduli vocali, leucoplachia ed ectasia capillare
Vocal nodules, leukoplakia, and capillary ectasia (1 of 4)
Vocal nodules, leukoplakia, and capillary ectasia (2 of 4)
Vocal nodules, leukoplakia, and capillary ectasia: 6 months later (3 of 4)
Vocal nodules, leukoplakia, and capillary ectasia: 6 months later (4 of 4)
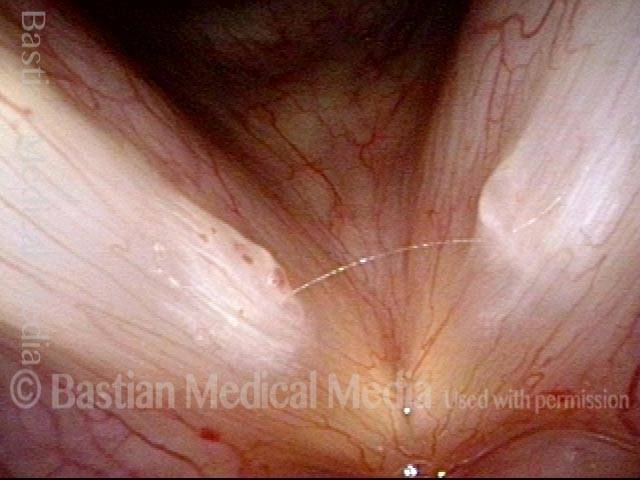
Solco glottico/leucoplachia/reflusso acido
Glottic furrow / Leukoplakia / Acid reflux (1 of 4)
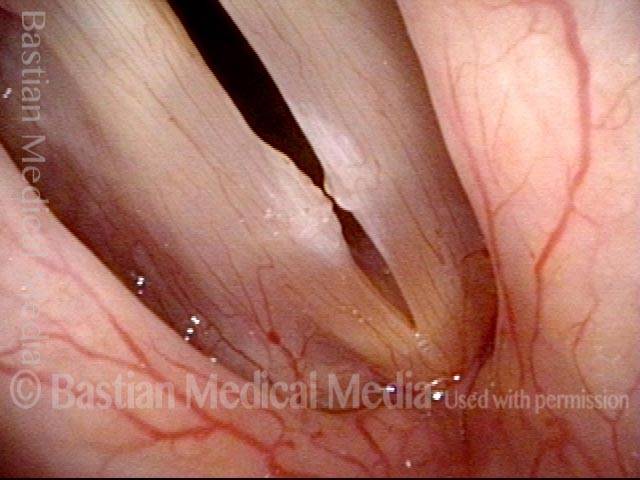
Leukoplakia (2 of 4)
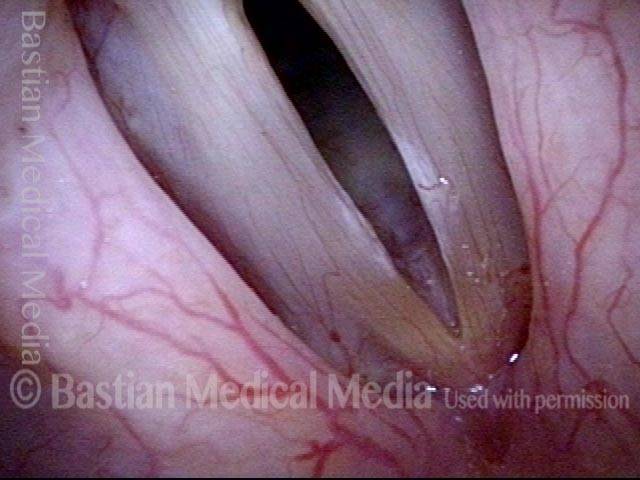
Glottic furrows (3 of 4)
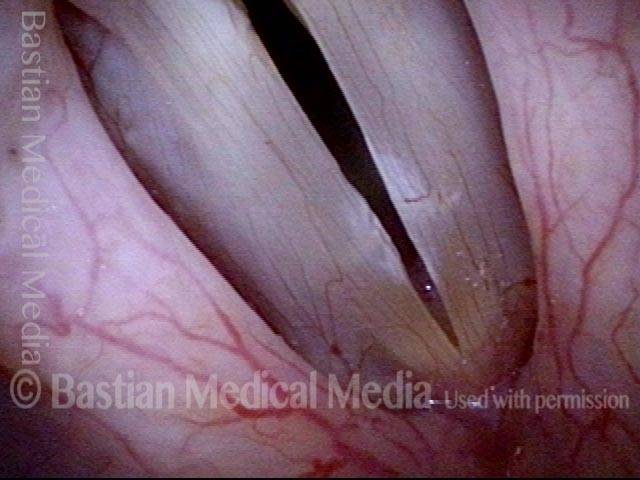
Gap during closed phase (4 of 4)

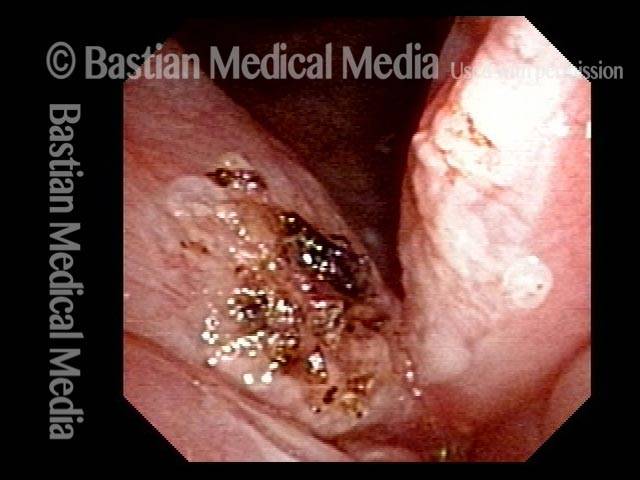
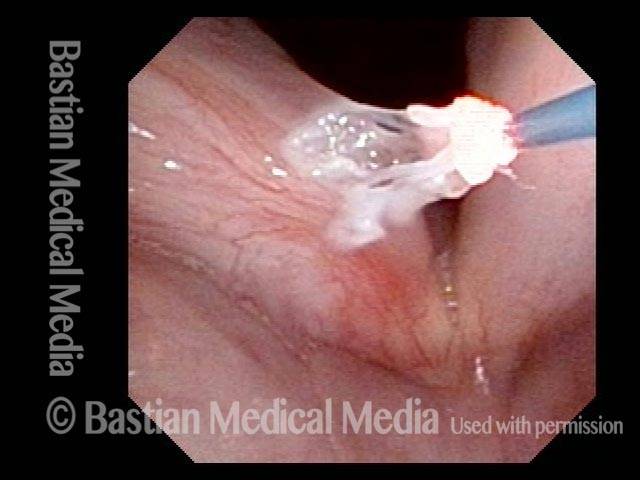
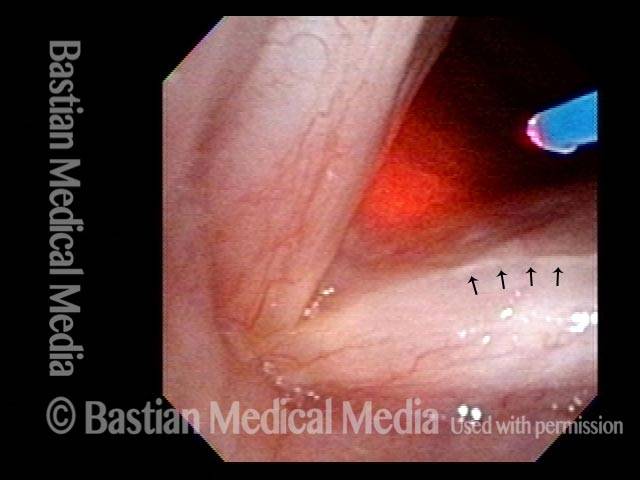
Intervento chirurgico con laser a tulio, con iniezione di anestetico locale, per il trattamento della leucoplachia
Leukoplakia, about to be treated with laser (1 of 4)

Injection of local anesthetic (2 of 4)
Injection of local anesthetic (3 of 4)
Right after thulium laser treatment (4 of 4)

Biopsia della leucoplachia
HIV Testing (1 of 2)

Biopsy (2 of 2)
