
Differential Re-Innervation after SLAD-R Surgery
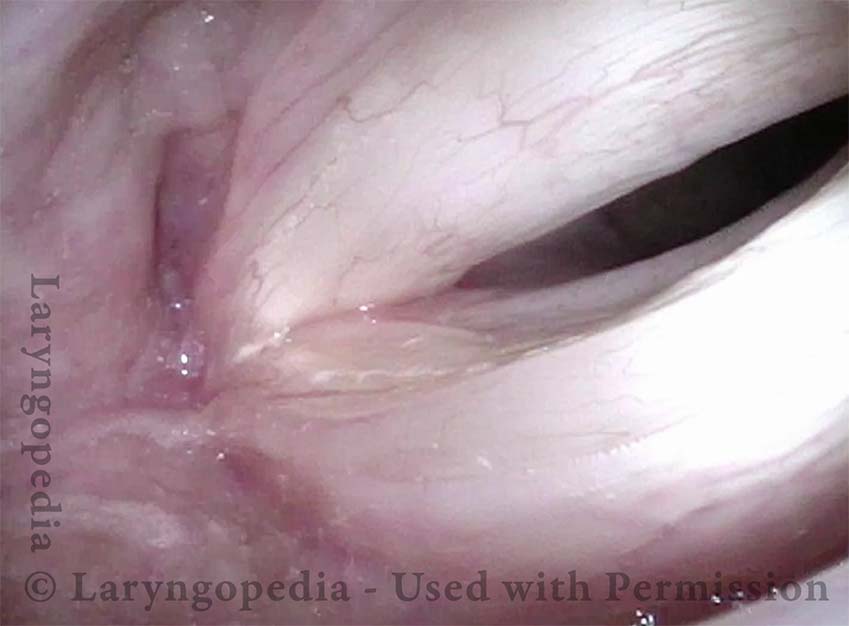
Six years post SLAD-R (1 of 4)
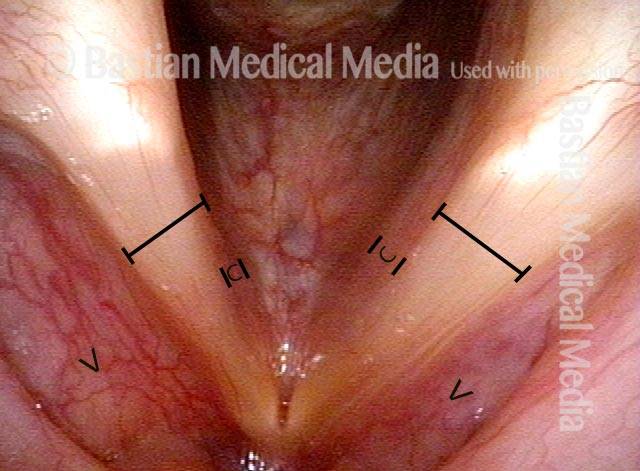
Six years after SLAD-R performed elsewhere. Note that re-innervation appears greater for left (right of photo) than right (left of photo) thyroarytenoid (TA) muscle. Signs of continuing atrophy of the TA muscle within the right cord (left of photo) include capacious ventricle (‘V’); absence of “conus” (‘C’) bulk below the free margin (see contrast between /–/ on both sides); slight concavity or bowing of the free margin; and narrower band of the vocal cord itself that we sometimes refer to as the “spaghetti-linguini” larynx.
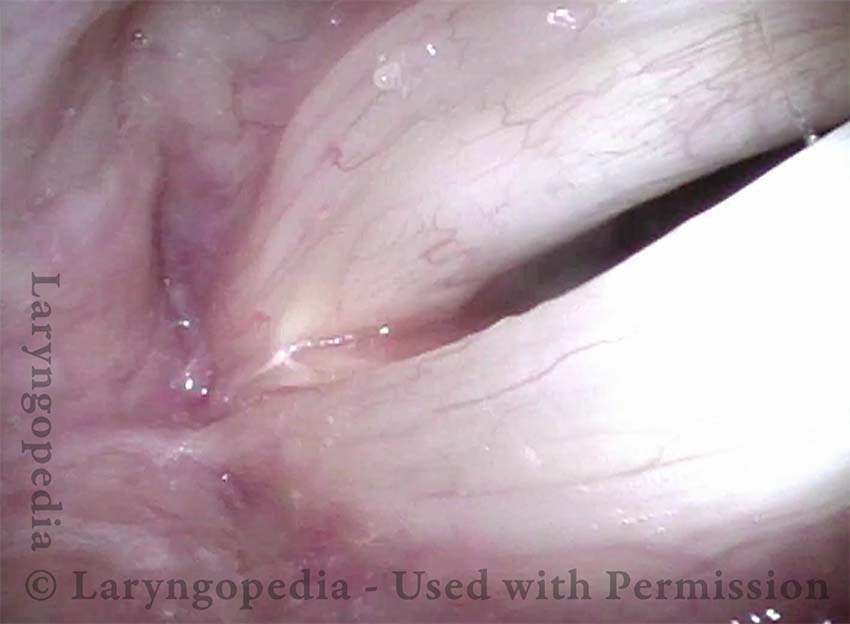
TA + LCA muscles (2 of 4)
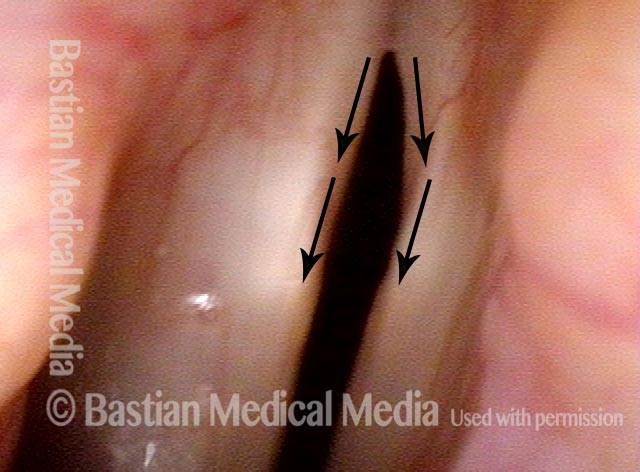
While TA is more recovered on the left (right of photo) as seen in photo 1, here we see that the lateral cricoarytenoid (LCA) muscle has recovered more on the right (left of photo). At the prephonatory instant, the failure of the left (right of photo) vocal process to turn to the midline indicates continuing weakness of the LCA muscle.
Greater amplitude of right cord (3 of 4)
Under strobe illumination, open phase of vibration shows greater amplitude of right cord (left of photo), consistent with the atrophy of the permanently somewhat weak TA muscle seen in photo 1.

Patient has returned to Botox (4 of 4)
Closed phase of vibration. A few years after SLAD-R, this man’s spasms recurred sufficiently that he has resumed Botox injections.

SLAD-R Findings in Spasmodic Dysphonia
This man has had longstanding laryngeal dystonia causing adductory spasmodic dysphonia. More than a year before these photos, he underwent SLAD-R on the left side (right of photo). The left cord moves normally, and one can see full recovery of the LCA (lateral cricoarytenoid) muscle, but the TA (thyroarytenoid) muscle is atrophic and flaccid.
Angle of Abduction (1 of 5)
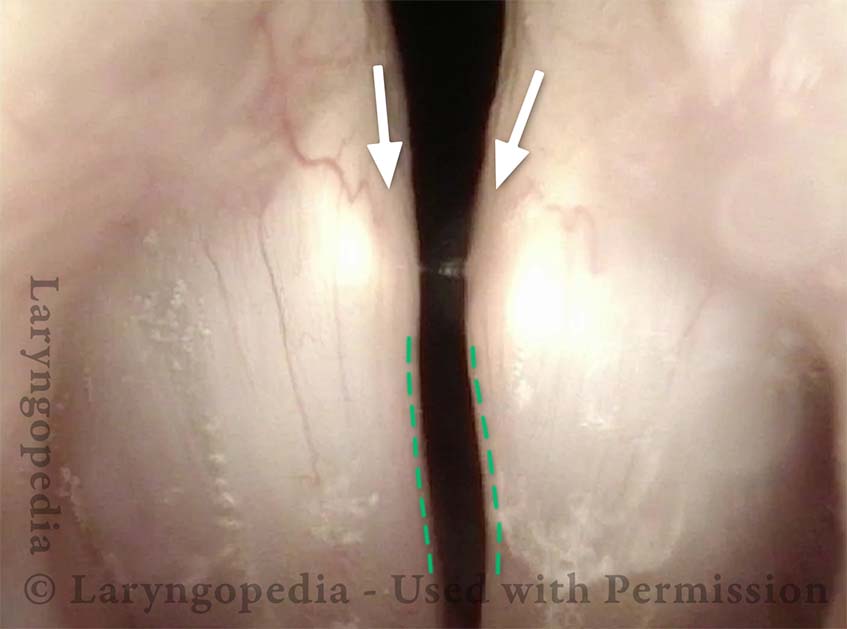
A year after SLAD-R, the angle of abduction (legs of the “V”) is the same bilaterally due to equal function of the PCA (posterior cricoarytenoid) muscle, not affected by the surgery. The margin of the folds (dotted lines) appear similar. But the bulk of the left thyroarytenoid muscle as manifested in the conus (bulge below the margin) appears to be less on the left (right of photo) than on the right (left of photo). The conus is also mildly flattened, as well. See the difference as marked by the bracketed lines.

Concave Margin (2 of 5)
As the cords approach approximation, the vocal processes are both beginning to point equally towards each other, suggesting that both LCA (lateral cricoarytenoid) muscles fully functional. However, the margin of the left cord appears to be subtly more concave than the right, suggesting mild TA (thyroarytenoid) muscle atrophy. (Compare dotted lines.)
Lateral buckling (3 of 5)
During phonation under standard light, the cord margins are both blurred due to vibration, but the left side (right of photo) is buckling laterally, consistent with atrophy/flaccidity.
Mild bowing (4 of 5)
Under strobe light, at maximally closed phase of vibration. This view again suggests mild bowing of the left cord (right of photo).
Greater amplitude (5 of 5)
The open phase of vibration shows much greater amplitude (lateral excursion) of left cord oscillation (lower right of photo) than on the right vocal cord (upper left of photo). Furthermore, the vibratory wave of the left cord is much greater, also consistent with atrophy/flaccidity.

How Effective Is SLAD-R in Treating AD-SD?
SLAD-R compared to high quality botulinum toxin injections.
SLAD-R: A New Surgical Treatment for AD-SD [1]
Gerald S. Berke, MD et al.