Subglottic stenosis is narrowing just below the vocal cords, in the lowest part of the larynx and immediately above the first tracheal ring. Examples of causes include scarring from a breathing tube used during a long ICU stay, Wegener’s Granulomatosis (aka Granulomatosis with Polyangiitis [GPA]), and idiopathic subglottic stenosis (aka limited Wegener’s Granulomatosis).
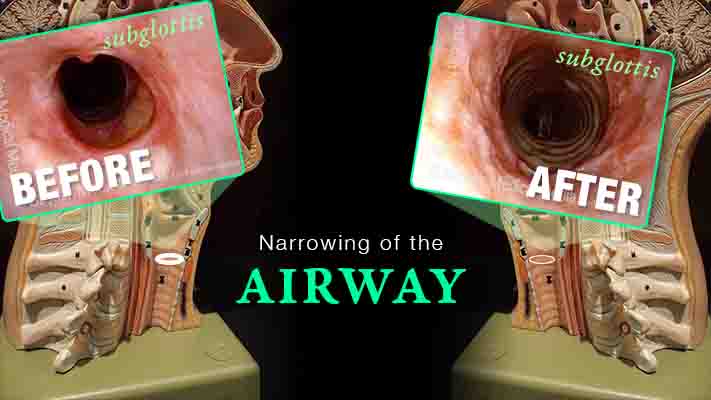
Subglottic Stenosis, after Treatment
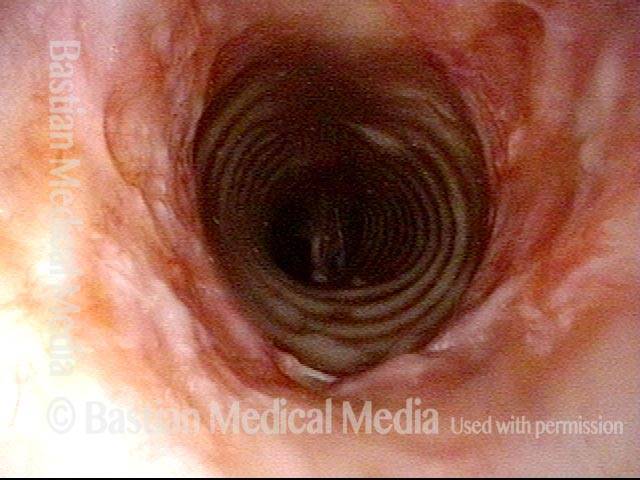
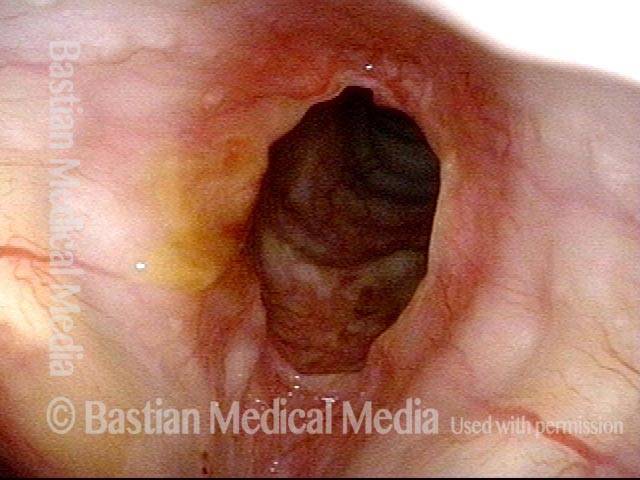
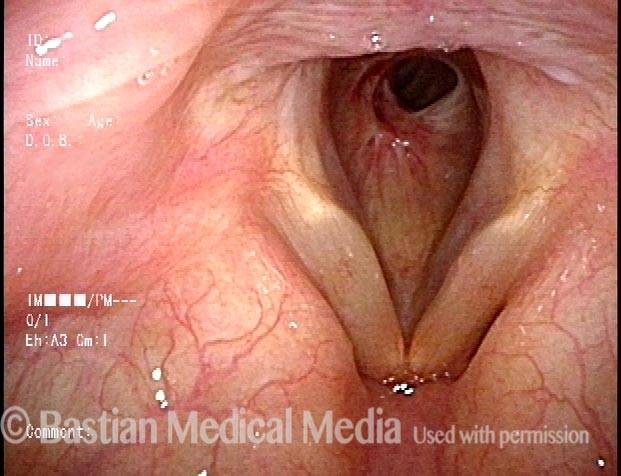
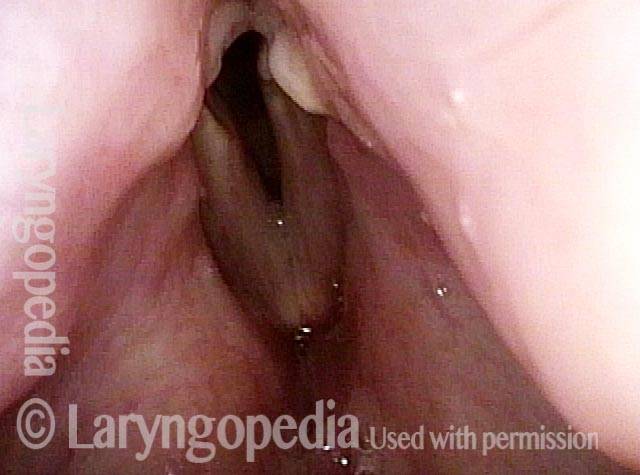
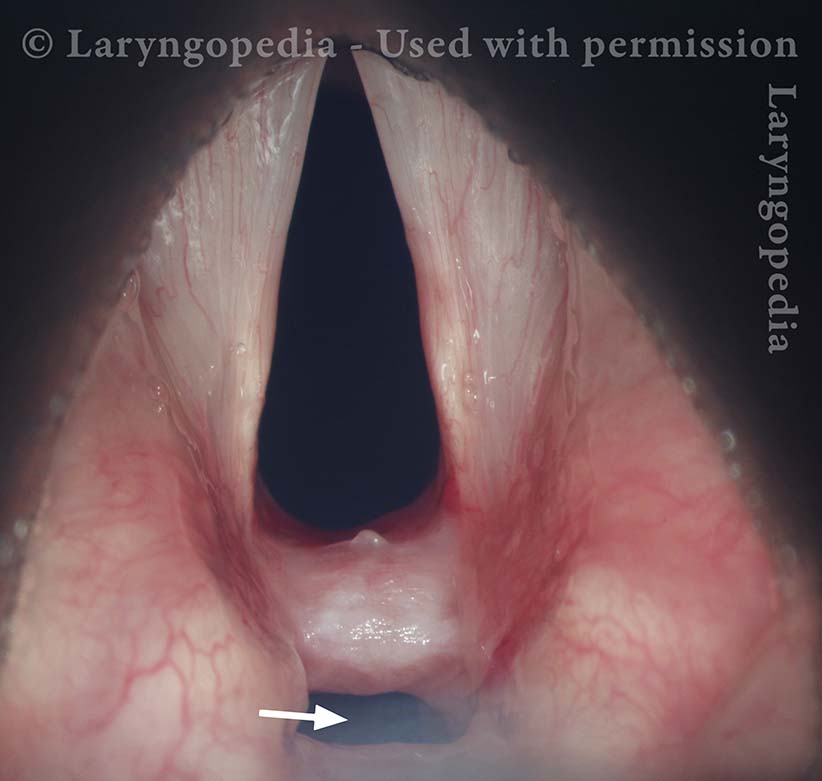
Subglottic stenosis, before treatment (1 of 2)
Subglottic and high tracheal stenosis, inflammatory, idiopathic (Lab).

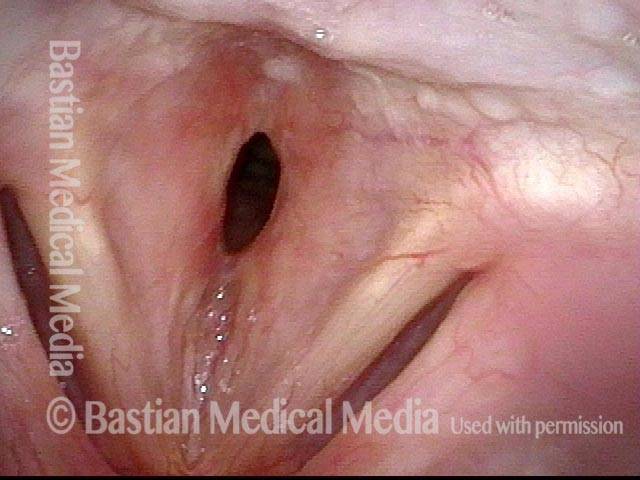
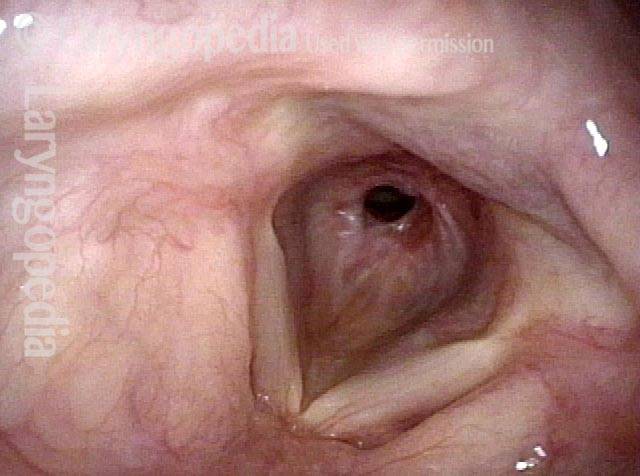
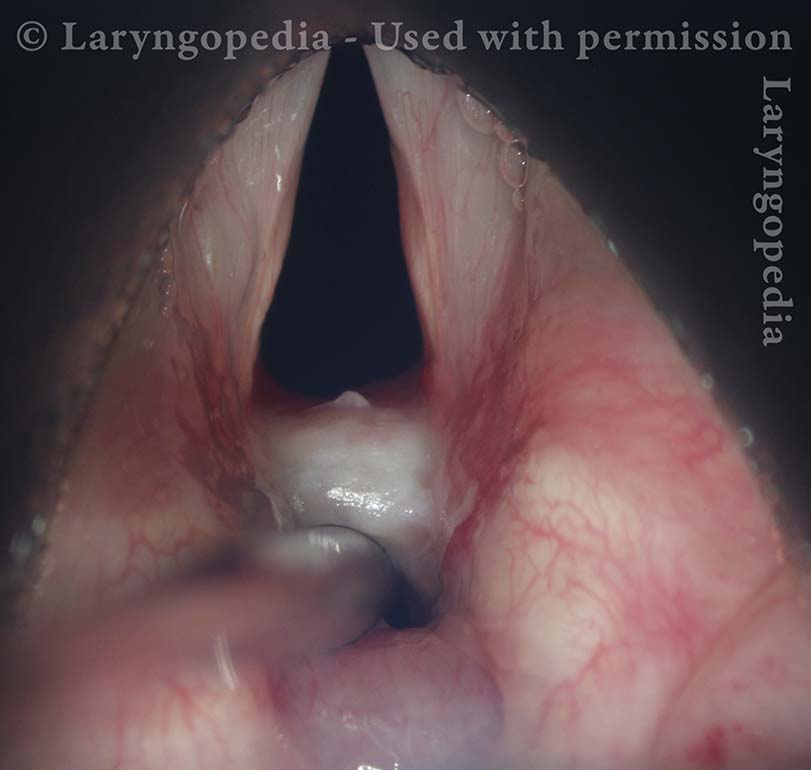
Subglottic stenosis, after treatment (2 of 2)
Same patient, a few days after dilation and steroid injection (Lab).

Subglottic Stenosis, before and after Dilation
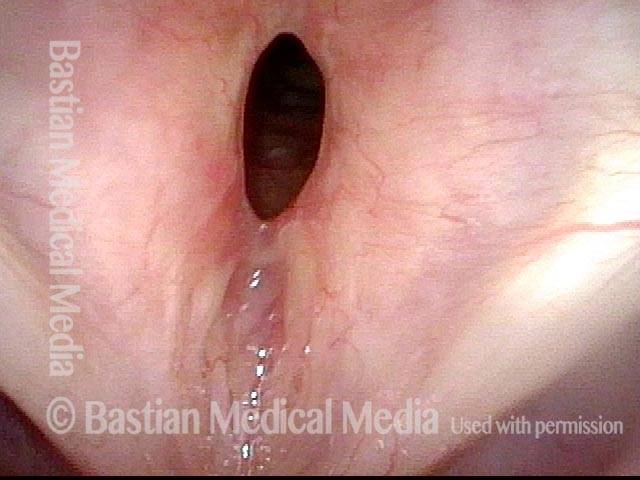
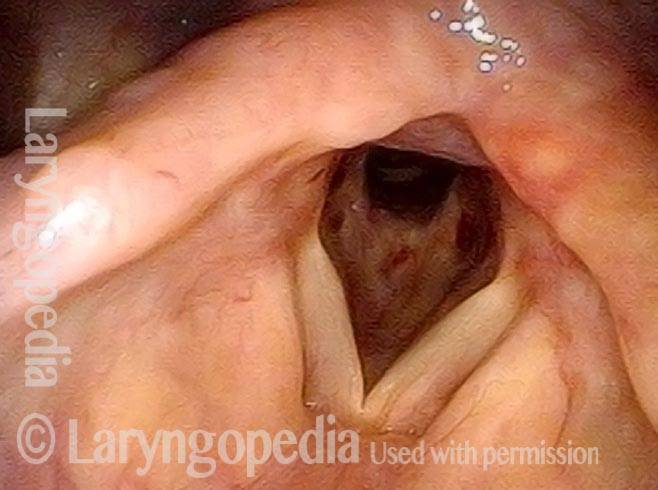
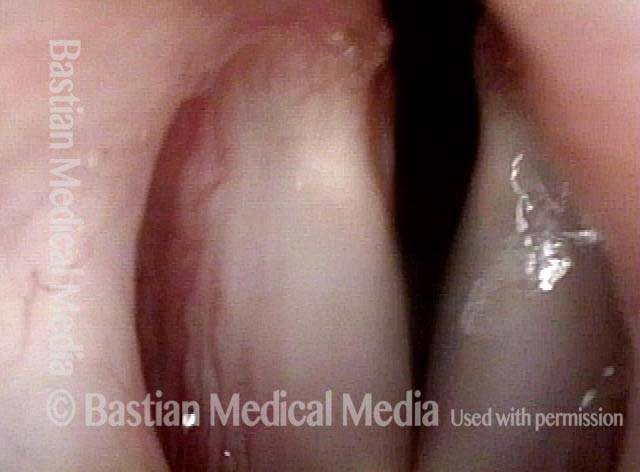
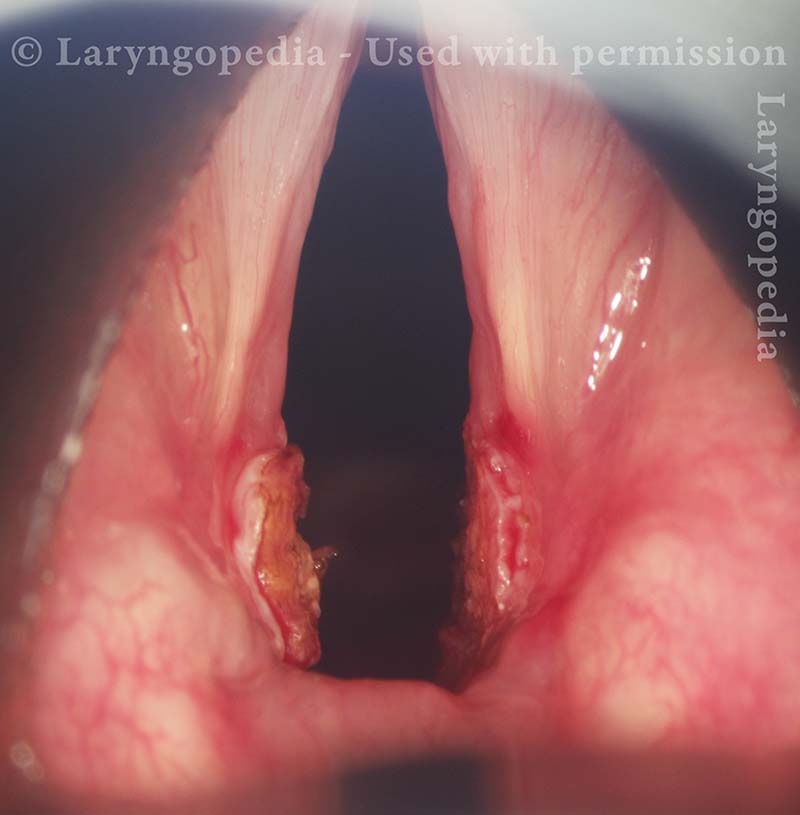
Subglottic stenosis, before dilation (1 of 2)
This individual has undergone at least a dozen prior dilations, each of which provides dramatic relief from noisy breathing and exercise intolerance. Here the patient is halfway to needing re-dilation, due to the typical inflammatory stenosis that is seen. Compare with photo 2.
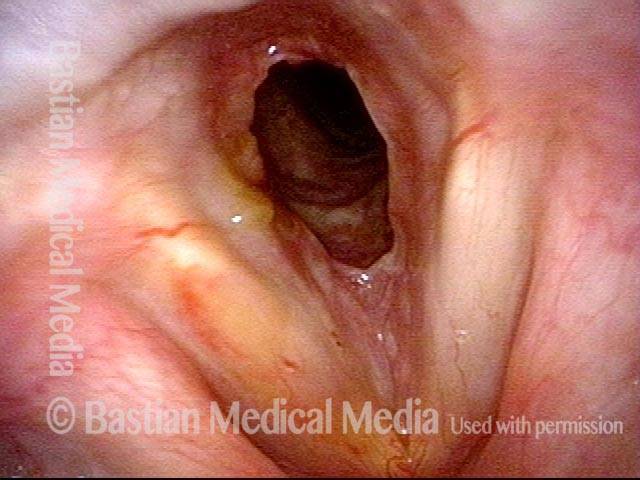
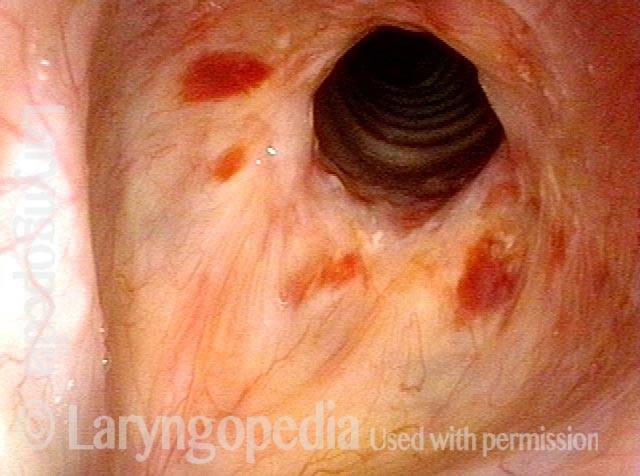
Subglottic stenosis, after dilation (2 of 2)
One week after one of this patient’s dilations (with Kenalog injection and topical Mitomycin C), showing a dramatic widening of her airway; compare with photo 1. After a number of years, inflammatory lesions such as this sometimes “burn out,” and the interval between dilations increases.
Example 2
Subglottic stenosis (1 of 5)
Middle-aged woman with unexplained shortness of breath and noisy breathing, due to this idiopathic inflammatory and very high subglottic stenosis. The patient initially declined dilation due to her anxiety. She also had granularity of the nasal septum and a positive ANCA profile for Wegener’s granulomatosis.

Subglottic stenosis, worsened (2 of 5)
Five months later, the symptoms became intolerable, and the stenosis was noted to be slightly narrower and with a greater posterior component. The patient agreed to dilation.
Subglottic stenosis, worsened (3 of 5)
Same exam as photo 2; this close-up view shows more clearly the inflammatory nature of this stenosis.
Subglottic stenosis, after dilation (4 of 5)
Five days after outpatient dilation, triamcinolone injection, and topical mitomycin C application. The patient’s symptoms have vanished, the harsh inspiratory noise is no longer heard, and the size of the airway, though still not normal, is more than doubled. Compare with photo 2 of this series.
Subglottic stenosis, after dilation (5 of 5)
Same exam as photo 4, close-up view. Intensification of the inflammatory changes of this stenosis are expected so early after dilation. Compare size of the stenosis with photo 3 of this series.
Stenosis Before and After Dilation for Forme Fruste Wegener’s
Subglottic stenosis (1 of 5)
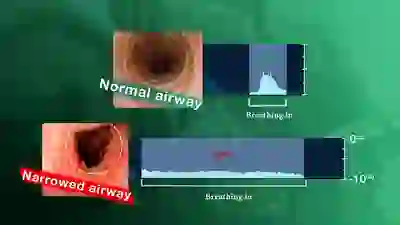
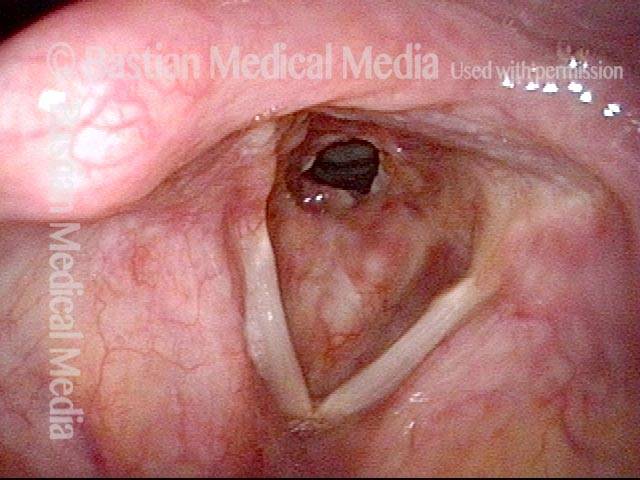
High-grade subglottic stenosis in a woman diagnosed syndromically with forme fruste Wegener’s granulomatosis-related subglottic stenosis. With a narrowing less than 50%, she is very symptomatic. Her breathing is noisy, and her forced inspiration time is about 3 seconds. Compare with photo 4.
Inflammation (2 of 5)
Closer visualization reveals the inflammatory nature of the stenosis.

Flexible scope (3 of 5)
Here the distal chip flexible scope has passed through the narrowing not only to see into distal trachea, but also as a breathing test. The patient becomes very aware of reduced space and this indicates a marginal airway.

Post-dilation (4 of 5)
A week after dilation, triamcinolone injection and mitomycin C application, the patient says breathing is now normal, and forced inspiration time is only a second in duration–normal. Compare with photo 1.
Post-operative bruising (5 of 5)
Closer visualization with early postoperative bruising. The trachea is now easily visible through the larger opening. Compare with photo 2.
Subglottic / Tracheal Stenosis
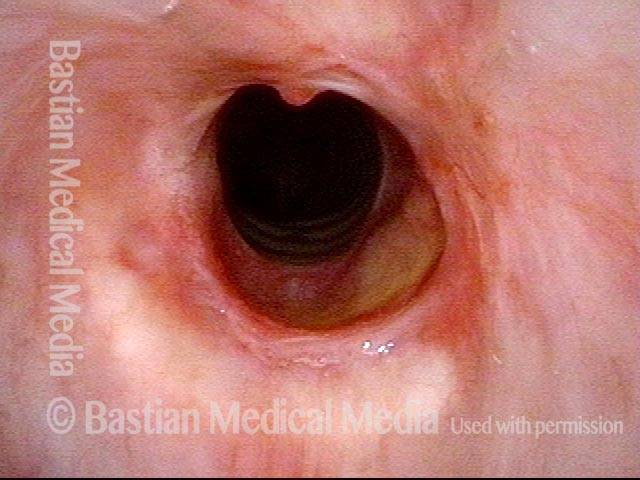
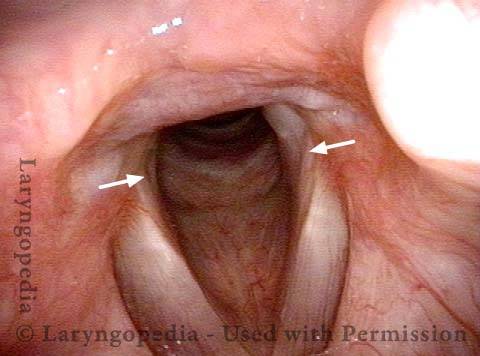
Wegener’s granulomatosis (1 of 4)
Inflammatory subglottic/tracheal stenosis, thought to be the result of an incomplete expression of Wegener’s granulomatosis (no history of trauma).
Subglottic / Tracheal stenosis (2 of 4)
Close view, from vocal cord level.

Subglottic / Tracheal stenosis (3 of 4)
Close view, from just above vocal cords.

Inflammed Stenosis (4 of 4)
Close view, showing the inflammatory nature of the stenosis.

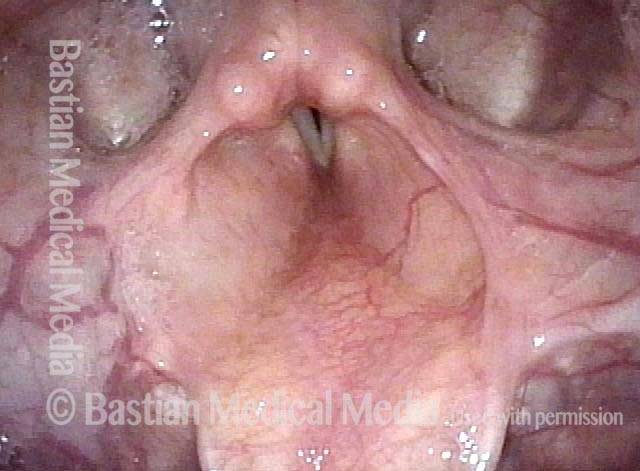
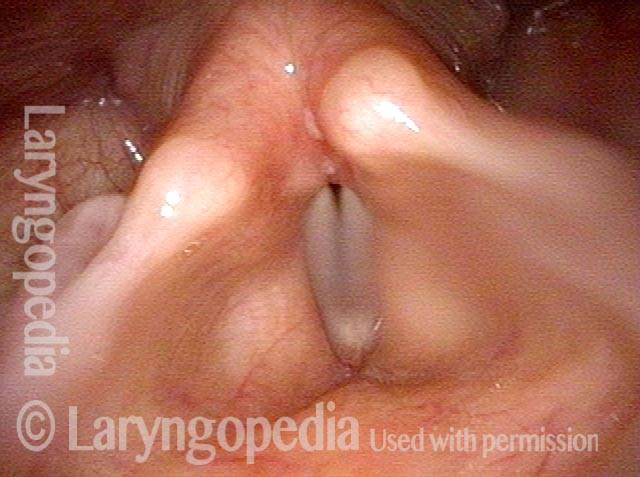
Subglottic Stenosis, Due to Wegener’s Granulomatosis
Subglottic stenosis, due to Wegener’s (1 of 2)
This person has Wegener’s granulomatosis, confirmed by anti-neutrophil cytoplasmic antibodies (ANCA) testing. Here, looking from above the vocal cords, one can see an estimated 50% narrowing of the subglottic and high tracheal passageway.
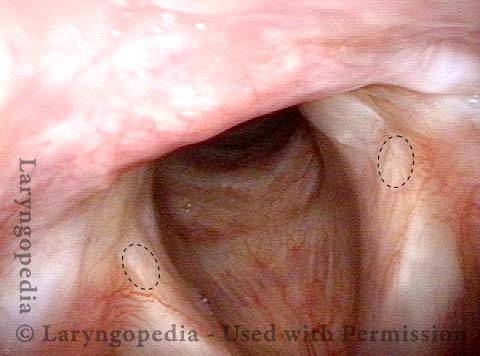
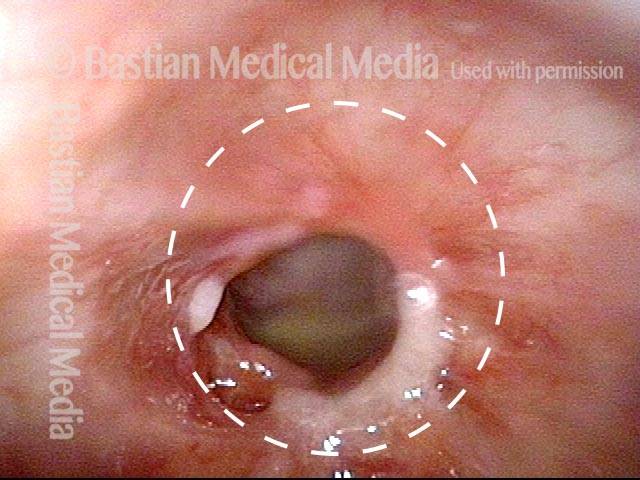
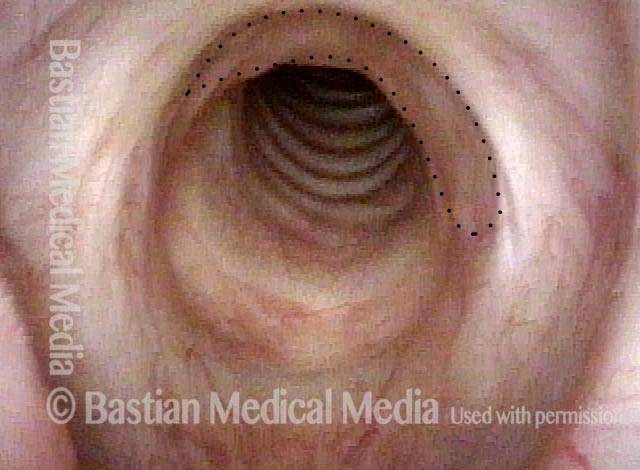
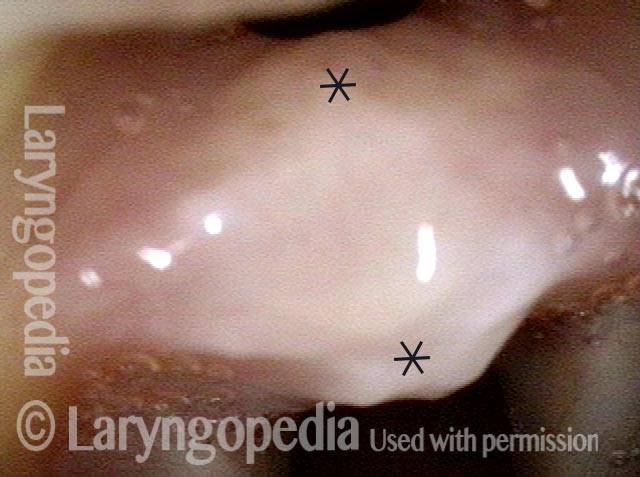
Subglottic stenosis, due to Wegener’s (2 of 2)
Viewed from within the subglottis, one can see more clearly the inflammatory nature of this stenosis. A dotted oval estimates what the normal caliber or width of this airway would be. This patient has been managed with systemic medication, but also occasional dilation, steroid injection, and Mitomycin C application.
Supraglottic, Glottic, and Subglottic Endotracheal Tube Injury
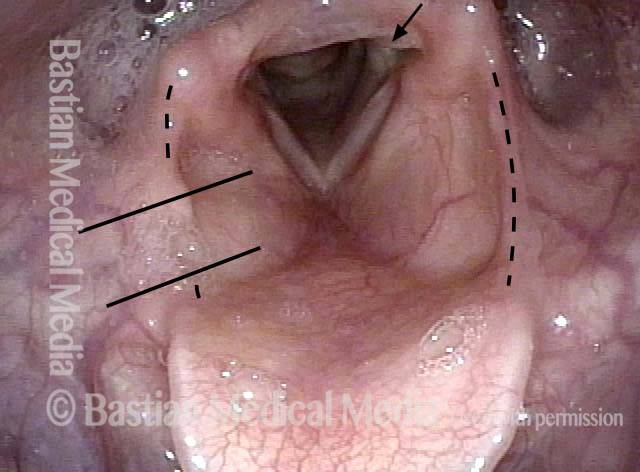
Breathing tube injury (1 of 4)
This 20-something individual was premature at birth and intubated for several weeks. Decades later, the evidence of breathing tube injury can be seen. Here, parallel lines outline likely trajectory of tube, taped at right corner of mouth. This fits as well with the left medial arytenoid divot at arrow. Dotted lines indicate aryepiglottic cord margins. Note deficit on right (left of photo) suggesting pressure necrosis from the endotracheal tube.
Aryepiglottic cord defect (2 of 4)
Aryepiglottic cord defect is better seen during phonation. The details of posterior commissure injury are obscured at this distance.
Phonation (3 of 4)
During phonation, low voice, note that the posterior vocal cords cannot come together, (even with cough or breath-holding) due to joint capsule injury from the endotracheal tube. Voice is intractably breathy.
Posterior subglottic thickening (4 of 4)
Posterior subglottic thickening surrounded by dotted lines, indicating a third level of old injury, here with no functional consequence.
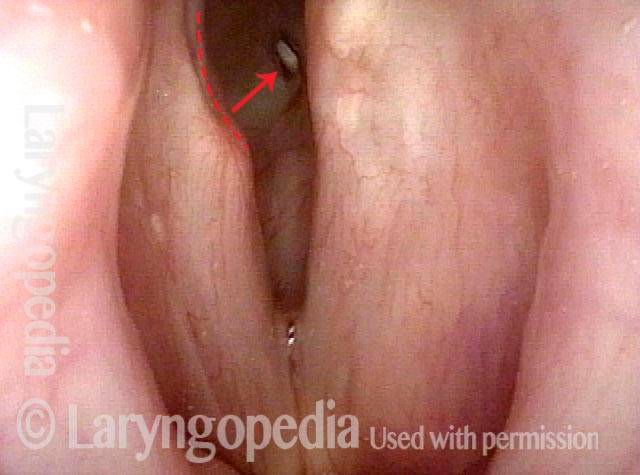
Pinhole Opening in Near-Complete Subglottic Stenosis
Narrowed space for breathing (1 of 4)
This man was gravely ill and intubated for several weeks. He is now well, but tracheotomy-dependent. The vocal cords do not abduct fully due to scarring of the cricoarytenoid joints. However, the narrowed space for breathing between the posterior vocal cords is not the main reason he is tracheotomy-dependent, as seen in the next photos.
Looking between the vocal cords (2 of 4)
At closer range, a deep erosion “divot” of the right posterior vocal cord (left of photo at dotted line) is the result of pressure necrosis of the endotracheal tube. Looking between the vocal cords into the subglottic airway, a small white oval is seen (arrow). This is the upper surface of the white plastic tracheotomy tube.
Closer view (3 of 4)
A closer view, again through the vocal cords.

Space between subglottis and trachea (4 of 4)
At yet closer range. The size of this pinhole between subglottis and trachea below cannot measure more than 3 mm. Crico-tracheal resection and re-anastomosis (planned for soon after this examination) is the best option to work towards decannulation.

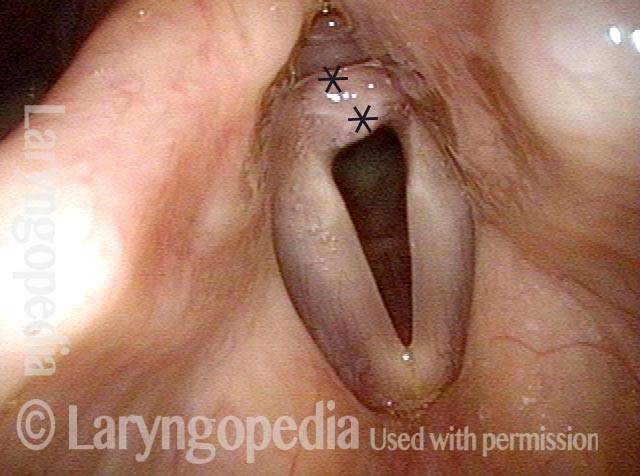
Difficulty Breathing after a 3-day Intubation
Noisy, restricted breathing following intubation (1 of 10)
This teenager was intubated for 3 days due to tongue swelling. Breathing became noisy and restricted approximately 6 weeks later. Note that the vocal cords do not abduct fully and there is what appears to be granulation tissue at the posterior commissure (anterior asterisk).
Normal voice (2 of 10)
The vocal cords can come into contact as shown here, consistent with her normal-sounding voice.
At close range (3 of 10)
At very close range within the posterior commissure, a small tract is seen posterior to the “granulation” which is now seen more clearly to be a broad-based synechiae with asterisks marking anterior and posterior limits.
Mucosalized tract (4 of 10)
Intraoperatively, the synchia appears mature. There is a mucosalized tract posteriorly (arrow). This makes joint injury less likely.
Suction Cannula (5 of 10)
A 4mm suction cannula is passed through the mucosalized tract posteriorly and lifted anteriorly, demonstrating its firmness.
CO2 Laser during Microlaryngoscopy (6 of 10)
The carbon dioxide laser has begin transecting the synechia.

Separation complete (7 of 10)
One can already see better abduction of the cords, suggesting that the cricoarytenoid joints are indeed undamaged.

Core removal complete (8 of 10)
The “core” of the synechia has been excavated, leaving the overlying mucosa intact (and retracted).
Complete abduction post-surgery (9 of 10)
Several months later, abduction of the cords is complete, proving that there is no injury to the cricoarytenoid joints. Arrows point to the subtle remnant of the base of the synechia.
Complete healing (10 of 10)
Faint dotted lines encircle the only remaining evidence of the synechia.