We refer to vocal cord dysfunction as nonorganic breathing disorder, laryngeal (see that entry for a fuller definition), which should be distinguished from nonorganic breathing disorder, tracheal.
Nonorganic Breathing Disorder, Laryngeal
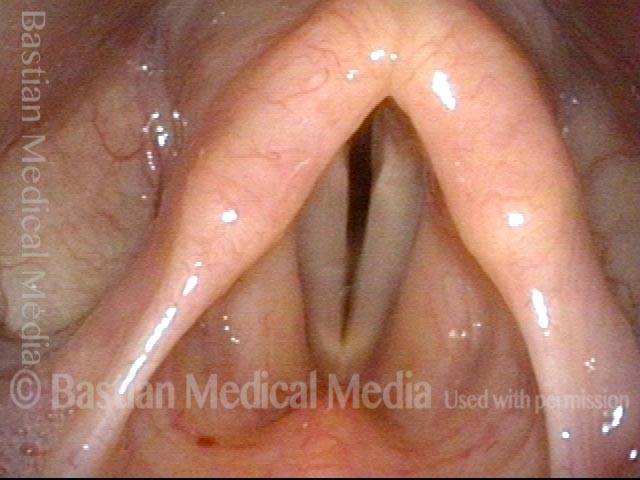
Nonorganic breathing disorder, laryngeal (1 of 4)
Normal quiet breathing with vocal cords widely abducted.

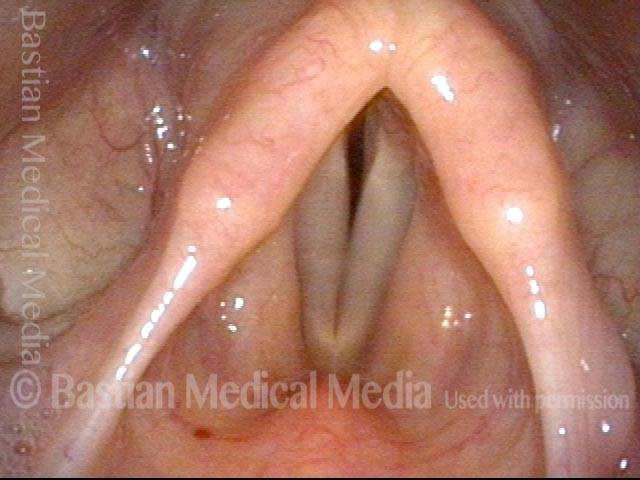
Nonorganic breathing disorder, laryngeal (2 of 4)
Typical posture of vocal cord dysfunction, with vocal cords only slightly abducted.
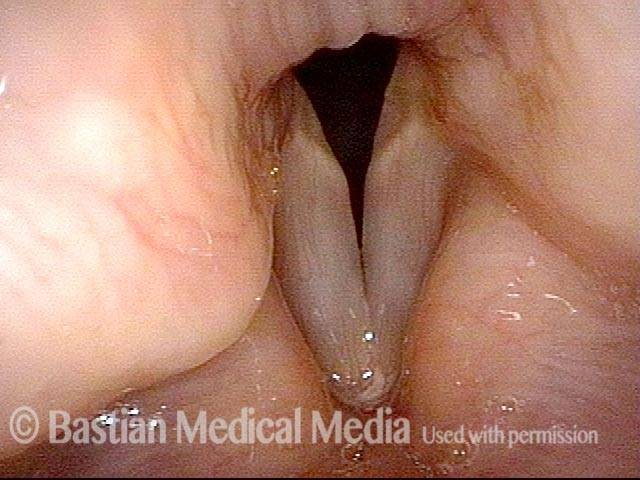
Breathing (3 of 4)
If air is drawn into the lungs in this posture, the vocal cords are brought into vibration and make inspiratory phonation (see blurring of the margins).
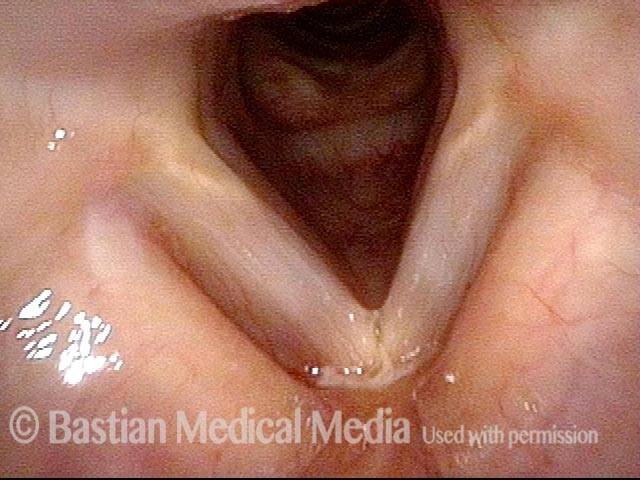
Nonorganic breathing disorder, laryngeal (4 of 4)
For comparison, same patient, normal (expiratory) phonation.

Example 2
Nonorganic breathing disorder, laryngeal (1 of 3)
Nonorganic breathing disorder in a patient who makes loud inspiratory noise with athletic exertion. Images shows functional partial closure during inspiration as a nonorganic phenomenon.
Nonorganic breathing disorder, laryngeal (2 of 3)
Normal abduction of vocal cords with elicited sniffing.
Nonorganic breathing disorder, laryngeal (3 of 3)
Note the convexity and vibratory blurring of the free margins, correlating with inspiratory phonation.
