A cord of tissue separated from the true vocal cord by the laryngeal ventricle. The false vocal cord serves as a secondary sphincter to help close the larynx when swallowing. While not “intended” for voicing, the false cords can be brought into vibration, but create a deep, rough voice quality.
False Cord Phonation
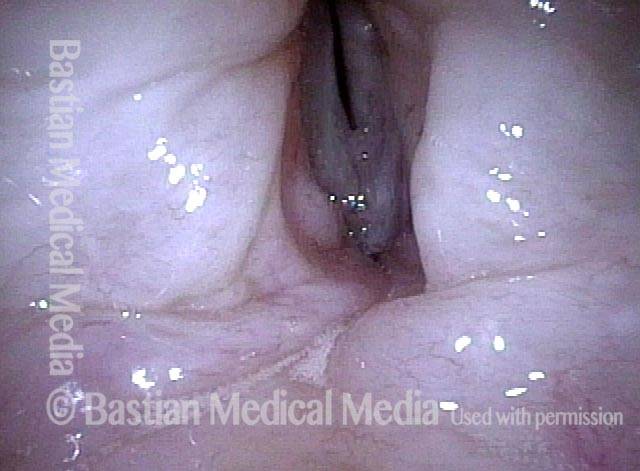
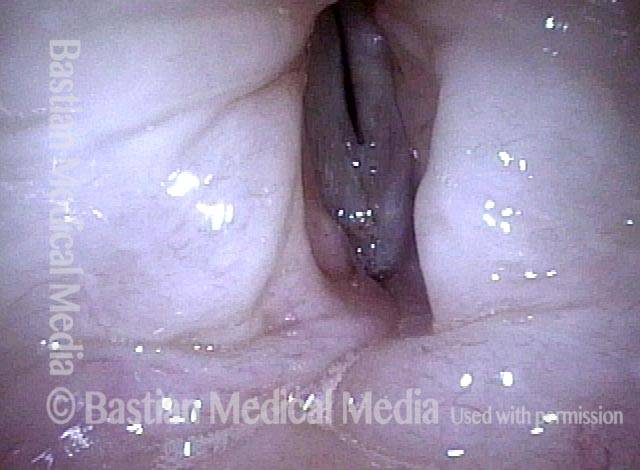
False cord phonation due to flaccid true cords (1 of 5): before false cords begin to vibrate
An elderly man, quiet by nature who uses the voice little, complains of weak, gravelly voice quality. This view of phonation, standard light, shows a slightly wider dark line of phonatory blurring. Also, the false vocal cords are overly approximated, but not yet participating in vibration (for that, see images 4 and 5).
False cord phonation due to flaccid true cords (2 of 5): before false cords begin to vibrate
Strobe light reveals an unusually wide amplitude of vibration, denoting flaccidity of the true vocal cords.

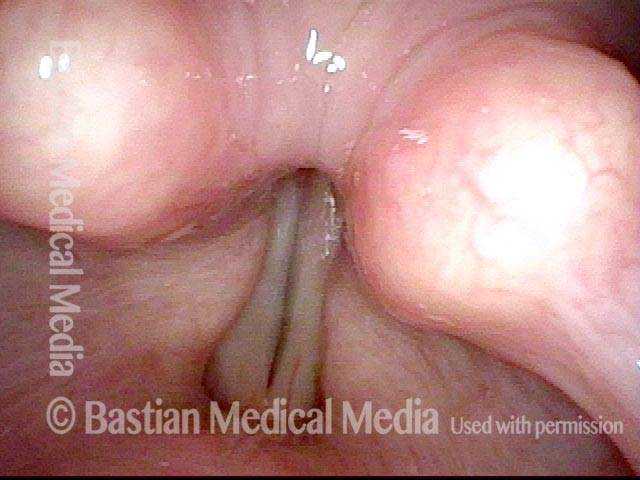
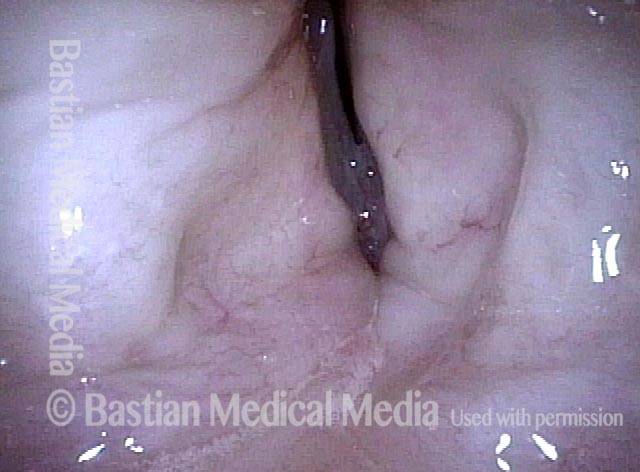
False cord phonation due to flaccid true cords (3 of 5): before false cords begin to vibrate
Maximum closed phase shows the telltale residual opening at the anterior commissure (from this perspective, the lowermost end of the true cords), also a potent indicator of flaccidity.
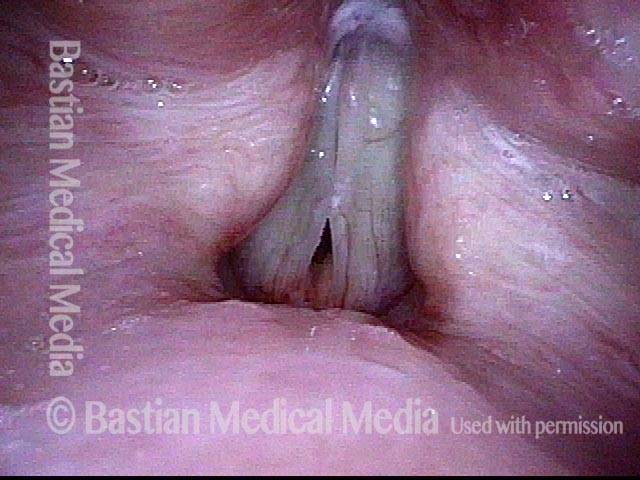
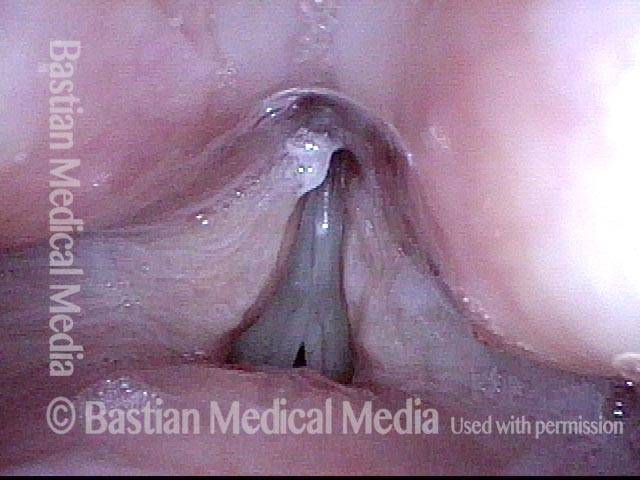
False cord phonation due to flaccid true cords (4 of 5): after false cords begin to vibrate
When asked to produce louder voice, the false cords begin to participate in vibration, and a rough, gravelly superimposed “ godfather” quality arrives. Notice that the true cords are in at least partial open phase of vibration.
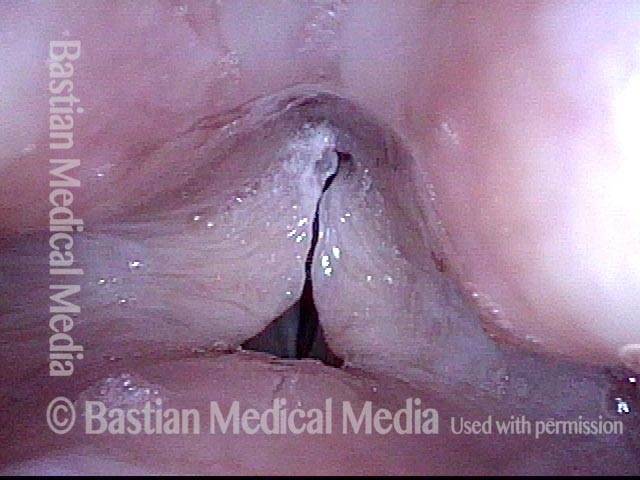
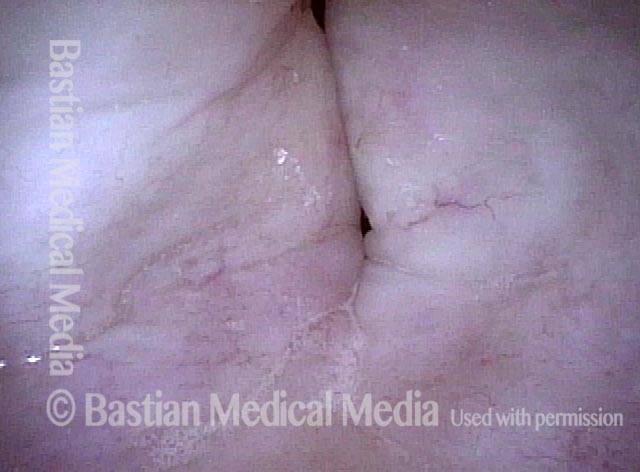
False cord phonation due to flaccid true cords (5 of 5): after false cords begin to vibrate
Now the false cords are in open phase of vibration, and the true cords are in maximum closed phase of vibration, with the same residual opening anteriorly seen in photo 3. False cord phonation is not to be seen most accurately as primary here, but as a secondary result of effort necessitated by flaccid true cords.
Adductory Spasmodic Dysphonia
AD-SD (1 of 2)
Sustained, clear phonation, standard light. Note vibratory blur of the vocal cord margins. The false vocal cords (lines) are in normal relation to the true vocal cords.

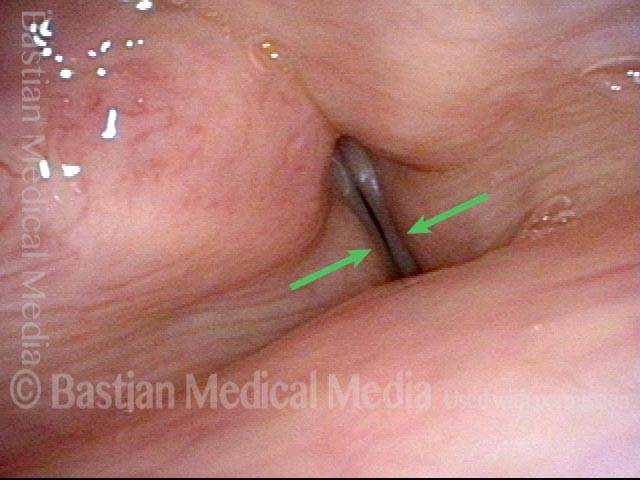
AD-SD (2 of 2)
Involuntary adductory spasm. Note that the false vocal cords suddenly over-close (arrows) as a result of the adductory spasm, and voice momentarily stops (along with vibratory blur).
Laryngeal Papillomas Rarely Can be Found by…Accident
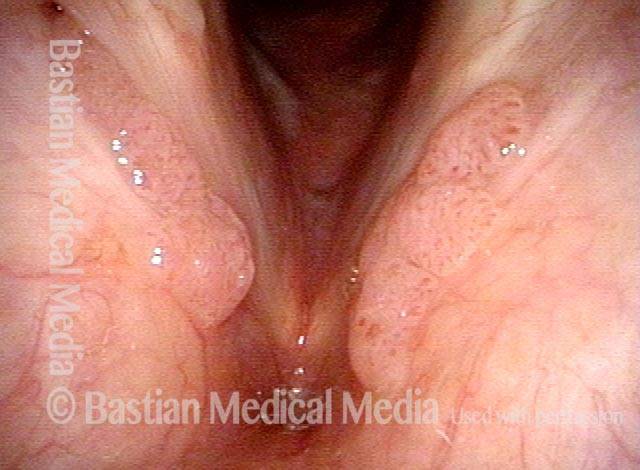
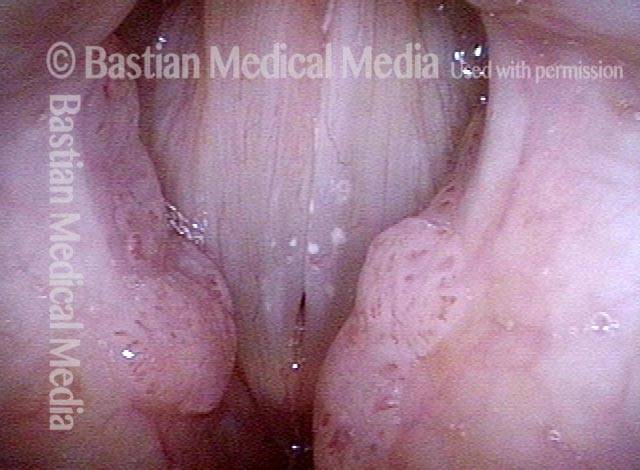
Papilloma finding (1 of 4)
This young man had a tonsil problem and normal voice but during the initial head and neck examination was found to have a papilloma in his larynx. Rapid recurrence and spread triggered referral. Note stippled vascularity on masses along the edges of the false vocal cords.
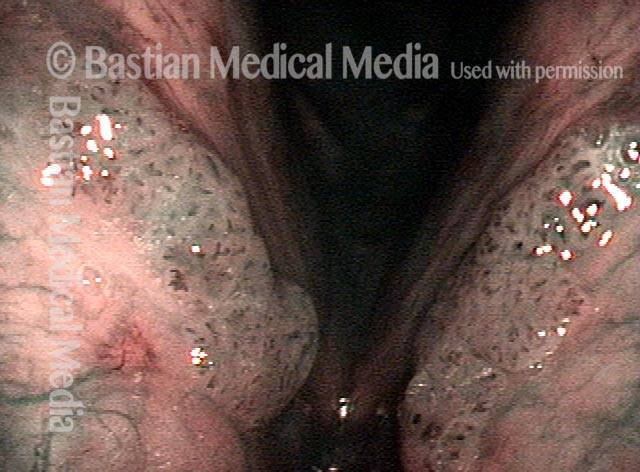
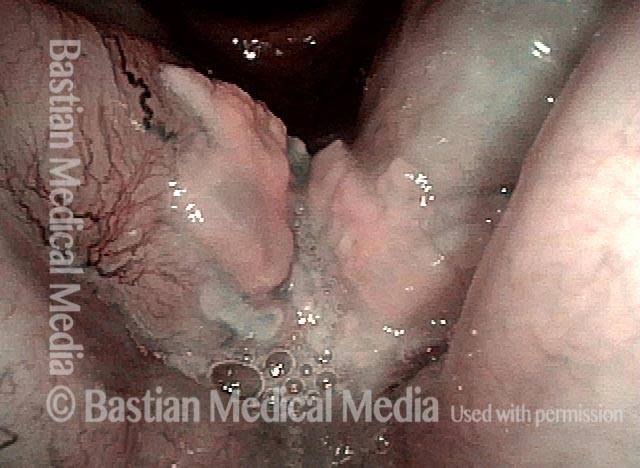
Narrow band light (2 of 4)
Narrow band light makes the papillomas much more evident.
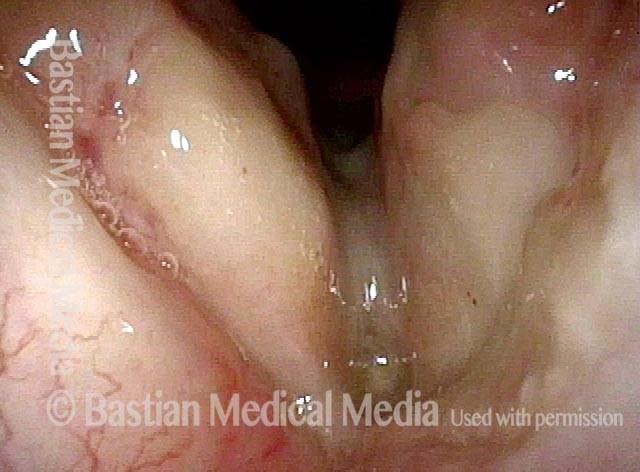
Closed phase (3 of 4)
Under strobe light, closed phase of vibration, the true cords are seen to be uninvolved, and this explains his normal voice.
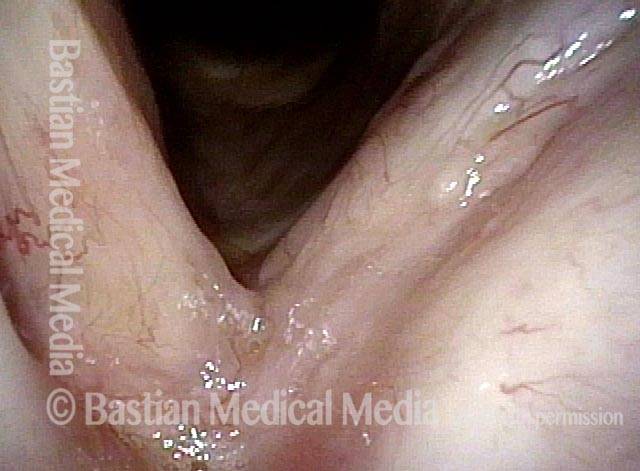
Open phase (4 of 4)
Open phase of vibration, strobe light. The plan is definitive removal and HPV subtyping.

Papillomas, HPV
Papillomas: HPV Subtype? (1 of 2)
Papillomas involving both the true and false vocal cords.

Papillomas: HPV Subtype (2 of 2)
At higher magnification, the stippled vascular markings become more evident.

Breaking the Rules in Larynx Cancer
Recurrent cancer (1 of 8)
Cancer, recurrent after radiotherapy. Cancer treatment 'rules' dictate a radical anterior commissure resection or more likely, total laryngectomy.

Closer view (2 of 8)
Closer view. The rules just invoked came about because cancer that crosses the anterior commissure is not to be trusted and especially after radiotherapy; cartilage involvement is far more likely; furthermore, laser resection might trigger radionecrosis. With careful patient involvement, an exception to these 'rules' was made here due to concomitant Stage 4 lung cancer of highly uncertain prognosis.
One week post laser resection (3 of 8)
A week after radical laser resection, including to the inner perichondrium of the thyroid cartilage. Wound healing/radionecrosis is a concern, as is the risk of recurrence when rules are bent.
One year postop (4 of 8)
A year post-op. There is no sign of recurrence. As expected, the vocal cords are scarred and will not vibrate. The patient has developed highly functional false vocal cord voice. (See the next four photos.)
True cord phonation (5 of 8)
Making voice, the true cords approximate but do not vibrate.
False vocal cords (6 of 8)
The false cords travel toward each other...
False vocal cord closure (7 of 8)
Here, they have come into full vibratory approximation.
True cords (8 of 8)
False cords separate, again revealing the non-vibrating true cords.