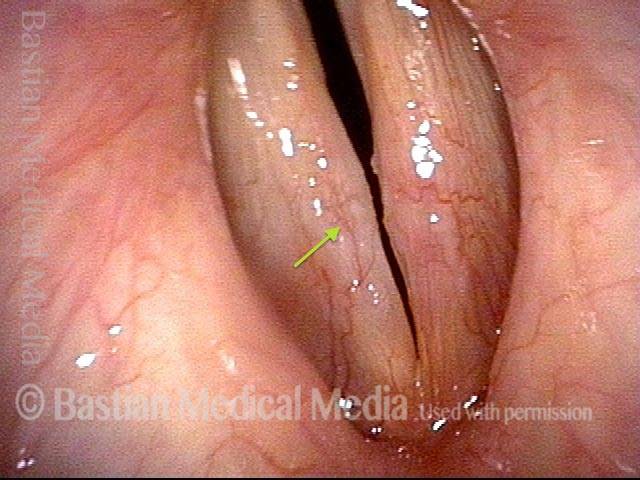
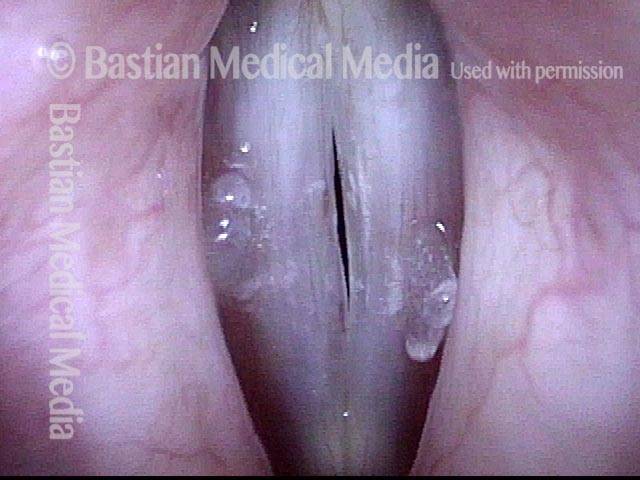
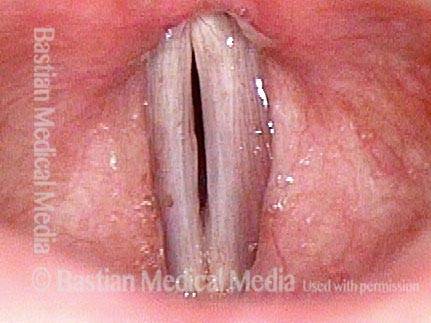
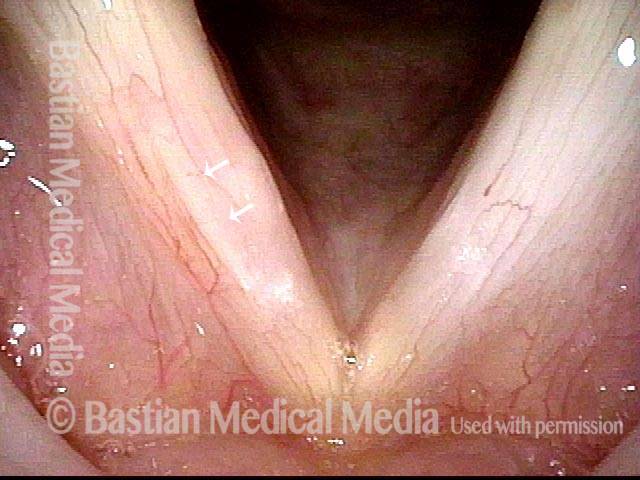
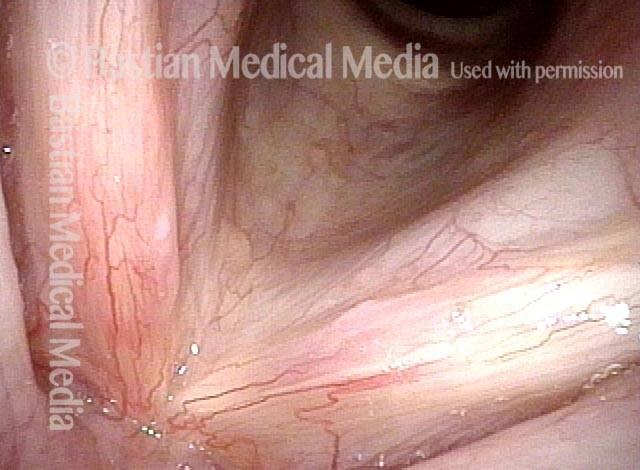
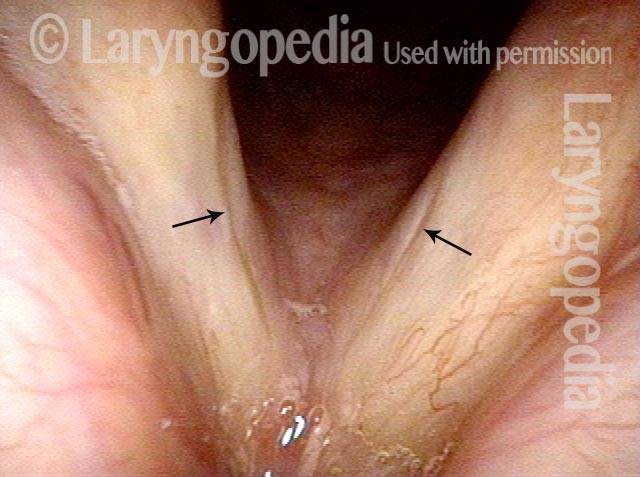
Glottic sulcus is a degenerative lesion consisting of the empty “pocket” of what was formerly a cyst under the mucosa of the vocal cord. The lips of a glottic sulcus may be seen faintly during laryngeal stroboscopy. Or, vibratory characteristics may suggest this lesion.
A glottic sulcus may be overlooked unless one is familiar with this entity. To paraphrase eminent French laryngeal microsurgeon Dr. Marc Bouchayer, these lesions are diagnosed much more frequently once you know about them than before. At present, aside from having the patient coexist peacefully with this problem via voice therapy and other measures, surgery is the primary treatment modality.
Glottic Sulcus, before and after surgery
Glottic sulcus, before surgery (1 of 3)

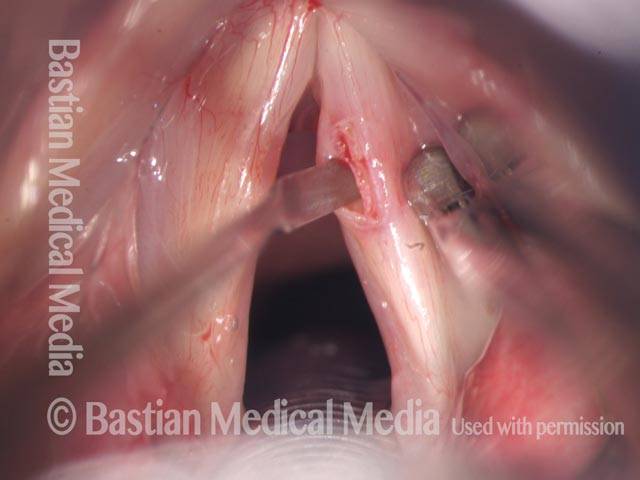
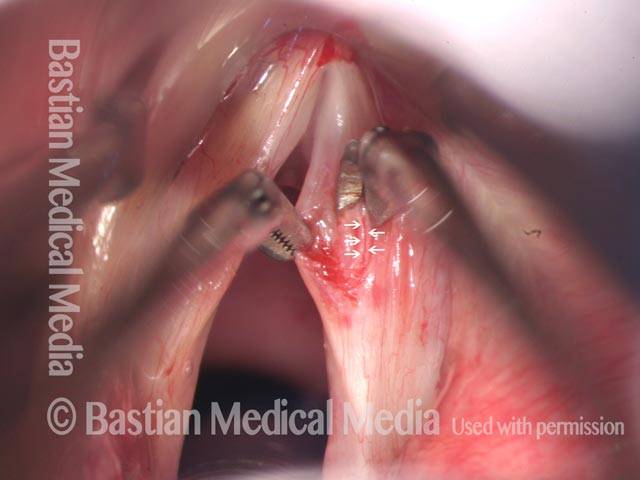
Glottic sulcus, before surgery (2 of 3)

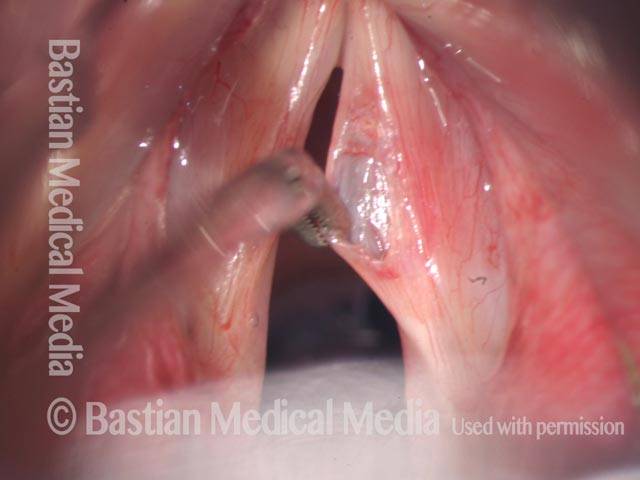
Glottic sulcus, after surgery (3 of 3)
Congenital glottic sulcus and bowing, before and after injection
Glottic sulcus (1 of 10)

Glottic sulcus (2 of 10)

Glottic sulcus (3 of 10)
Glottic sulcus (4 of 10)
Sulcus with bowing, just prior to injection (5 of 10)
Sulcus with bowing, just prior to injection (6 of 10)

Voice gel injection (7 of 10)
Voice gel injection (8 of 10)
After the injection (9 of 10)
After the injection (10 of 10)

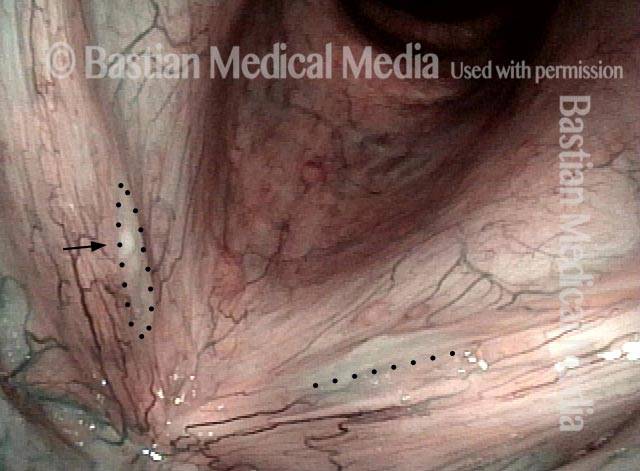
Glottic Sulcus
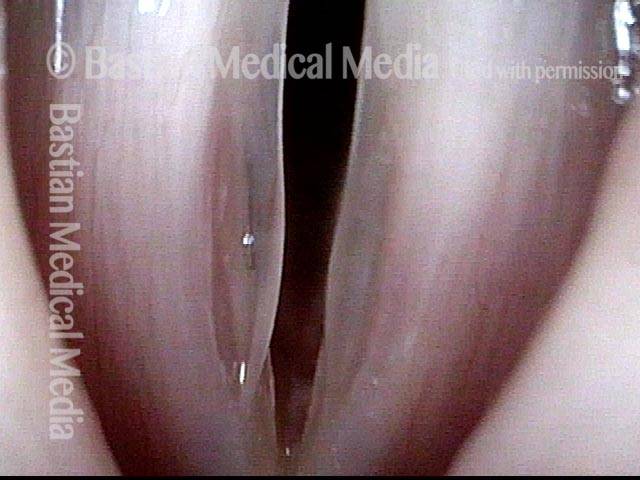
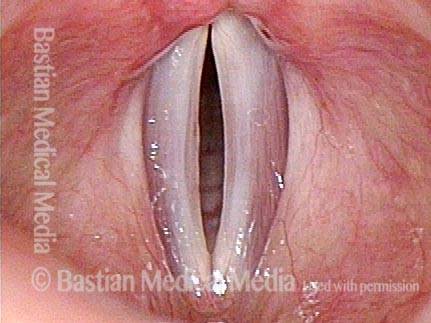
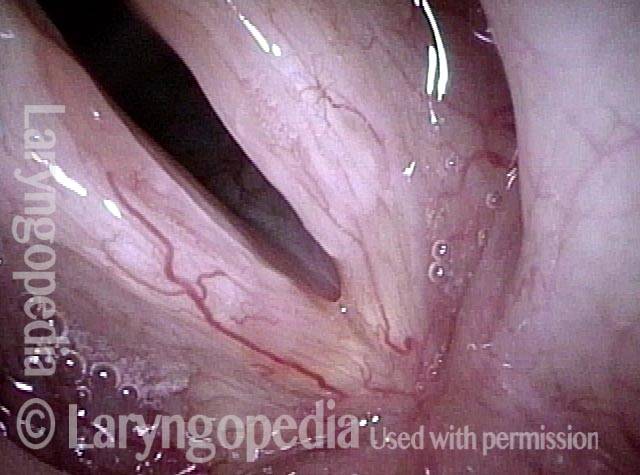
Glottic sulcus, open (1 of 2)

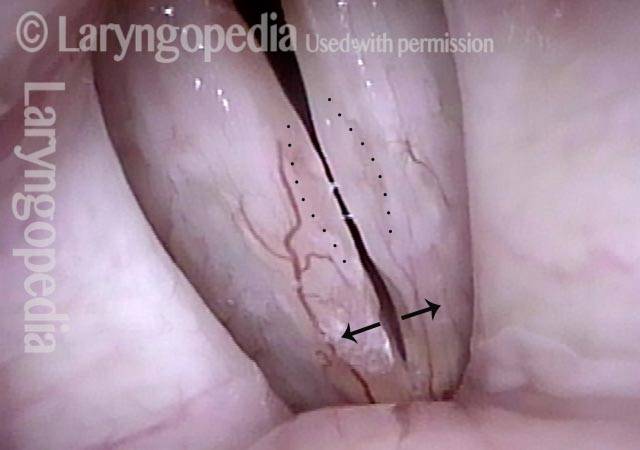
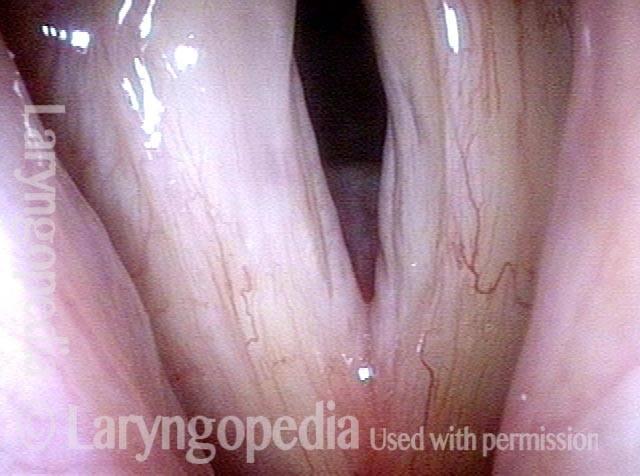
Glottic sulcus, closed (2 of 2)

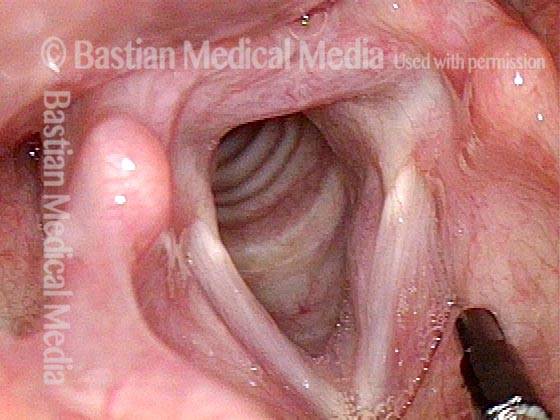
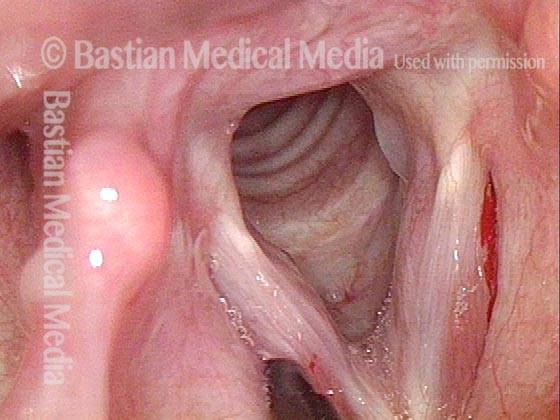
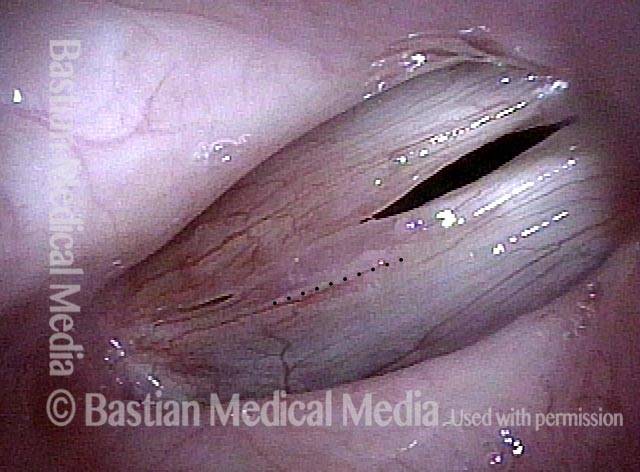
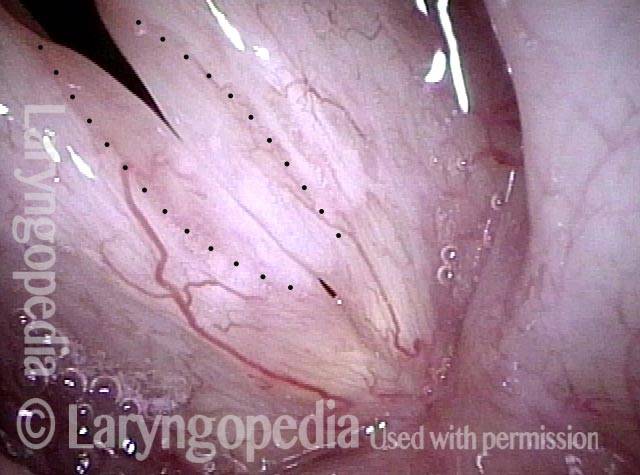
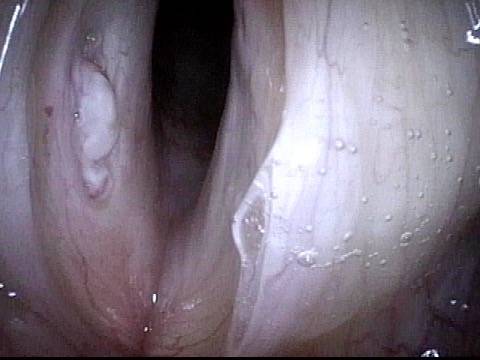
Example 2
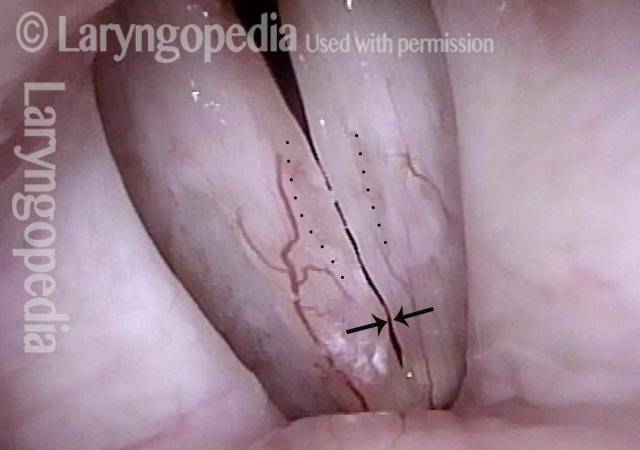
Glottic sulcus (1 of 2)
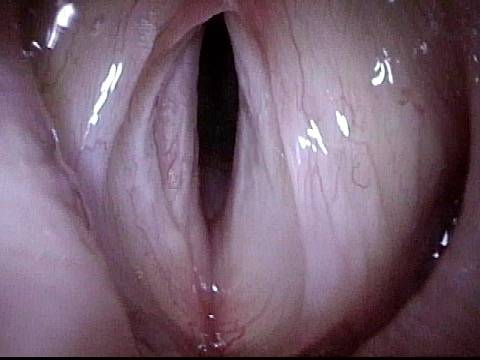
Glottic sulcus (2 of 2)

Example 3
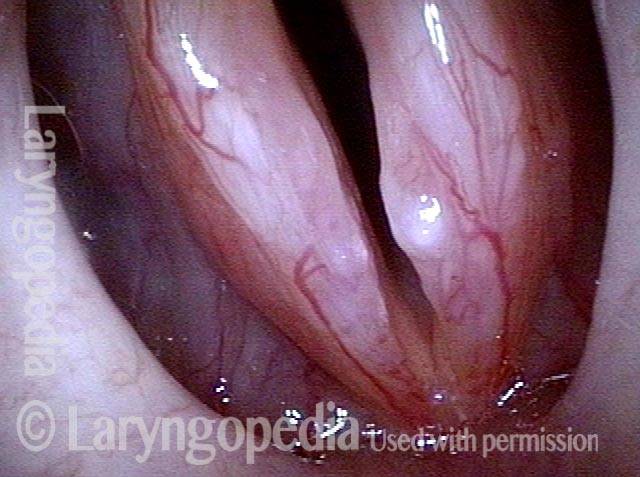
Glottic sulcus (1 of 2)
Glottic sulcus (2 of 2)
Example 4
Glottic sulcus (2 of 2)
Glottic sulcus (2 of 2)
Example 5
Glottic sulcus (1 of 1)

Glottic Sulcus and Glottic Furrow
Glottic sulcus and glottic furrow (1 of 4)
Glottic sulcus and glottic furrow (2 of 4)

Glottic sulcus and glottic furrow (3 of 4)

Glottic sulcus and glottic furrow (4 of 4)
Glottic Sulcus Operation
Glottic sulcus operation (1 of 7)
Glottic sulcus operation (2 of 7)

Glottic sulcus operation (3 of 7)

Glottic sulcus operation (4 of 7)

Glottic sulcus operation (5 of 7)

Glottic sulcus operation (6 of 7)

Glottic sulcus operation (7 of 7)

Surgical Removal of Glottic Sulcus
Surgical removal of glottic sulcus (1 of 4)

Surgical removal of glottic sulcus (2 of 4)
Surgical removal of glottic sulcus (3 of 4)
Surgical removal of glottic sulcus (4 of 4)
Open Cyst or Sulcus?
Hoarse voice (1 of 4)
Open Cyst Definition (2 of 4)
Closed phase (3 of 4)
Open phase (4 of 4)

Sulcus and Segmental Vibration
Glottic sulci (1 of 4)
Open phase (2 of 4)
Closed phase (3 of 4)
Segmental vibration (4 of 4)
Open Cyst and Sulcus; Normal and Segmental Vibration
Margin swelling (1 of 6)

Narrow band light (2 of 6)

Open phase, strobe light (3 of 6)
Closed phase, same pitch (4 of 6)

Segmental vibration (5 of 6)

Closed phase (6 of 6)

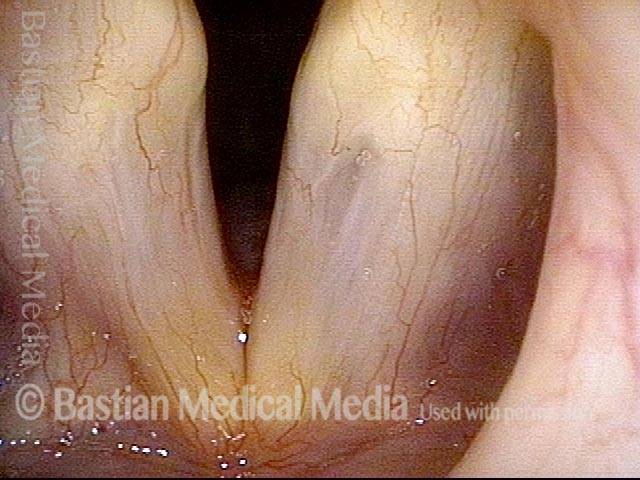
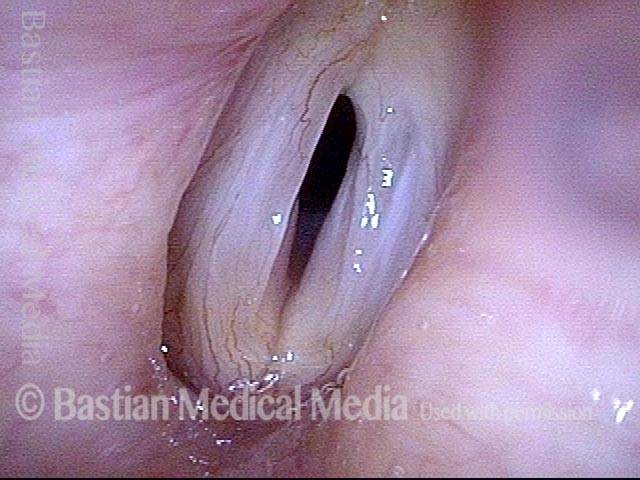
Glottic Furrow—Not Just Bowing and Not Glottic Sulcus
Bowing vocal cords with furrows (1 of 4)
Closed phase (2 of 4)

Open phase (3 of 4)
Lower pitch reveals furrow (4 of 4)

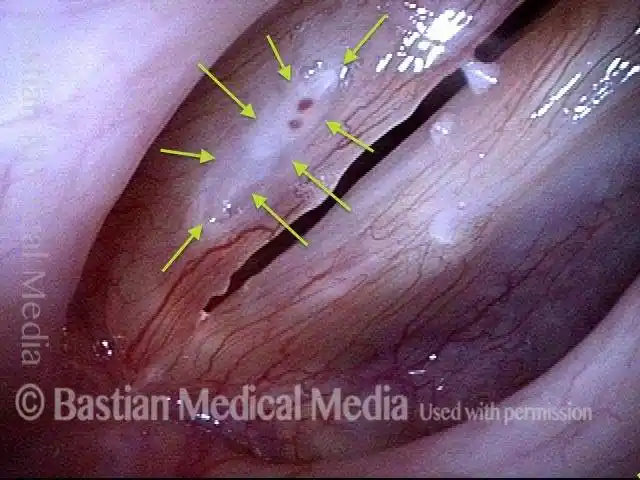
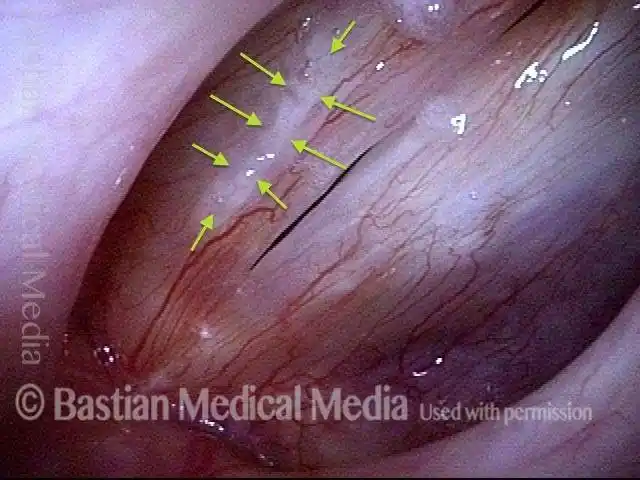
Mottled Vocal Cord Mucosa May Hide Glottic Sulci
Vocal cord swelling and mucosa (1 of 4)

Same view under strobe light (2 of 4)

Closed phase (3 of 4)

Glottic sulcus is visible (4 of 4)

A Case That Clearly Shows the Relationship Between Cyst & Sulcus
White Lesion on Right Vocal Cord (1 of 6)

White Lesion Under Strobe Light (2 of 6)
White Lesion Under Strobe Light (3 of 6)

White Lesion Removed (4 of 6)

Vocal Cords (5 of 6)
Vocal Cords without Lesion (6 of 6)
Nuances of Endotracheal Tube Injury
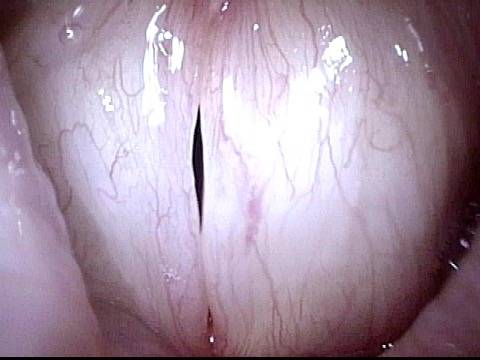
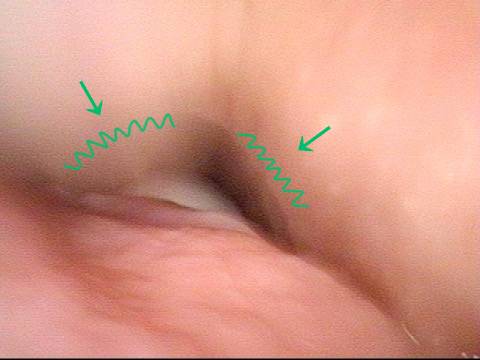
This woman with high-risk comorbidities of diabetes and obesity, was in ventilated in ICU more than a month for pulmonary complications of Covid-19 infection. She had an orotracheal tube in place for 3.5 weeks, and then a tracheotomy tube was placed. Now at her first visit a year later, she remains tracheotomy-dependent, and is told she has bilateral vocal cord paralysis (disproven in the following photo series).
Maximum glottic opening (1 of 8)

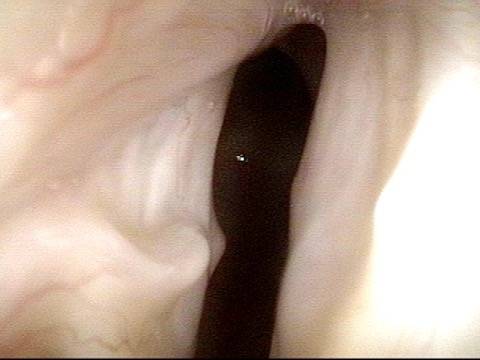
Undersurface mucosa indraws (2 of 8)

Phonation (3 of 8)

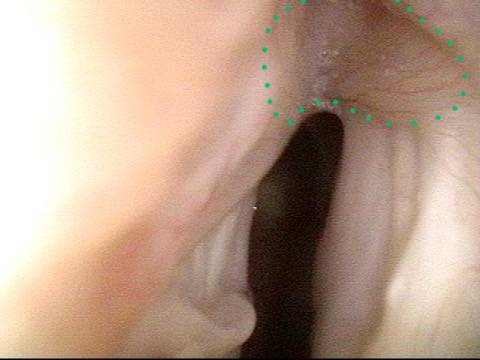
Posterior commissure divot (4 of 8)
Further evidence of scarring (5 of 8)
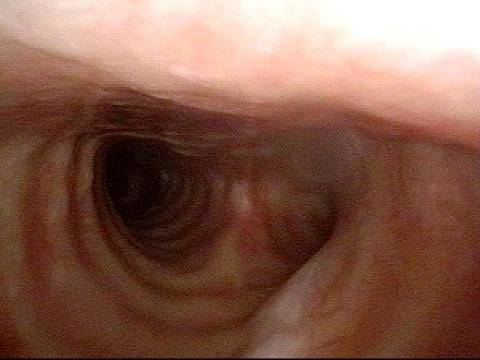
View into trachea (6 of 8)
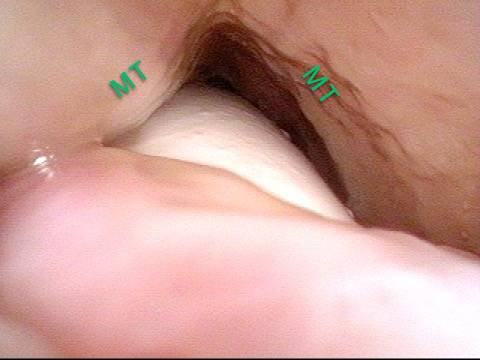
Vibration of trachea (7 of 8)
Open trachea beyond the tube (8 of 8)
The plan here is posterior commissuroplasty, followed by placement of a smaller trach tube and a trial of plugging. If plugging is tolerated during the day, she will need a sleep study with it plugged at night, given the tracheomalacia and her obesity.