La miotomia cricofaringea (CPM) è una procedura in cui il muscolo cricofaringeo, che forma un “anello” attorno all’esofago superiore, viene diviso o tagliato per rilassarlo. Questo viene fatto nei casi in cui questo muscolo cricofaringeo (cioè lo sfintere esofageo superiore) non riesce a rilassarsi quando si deglutisce (disfunzione cricofaringea anterograda [A-CPD]), con conseguente ostruzione funzionale. Il CPM lascia il muscolo sempre aperto e consente alla persona di riprendere la deglutizione in modo relativamente normale.
In una percentuale di soggetti con mancato rilassamento del muscolo cricofaringeo, le continue alte pressioni della deglutizione possono eventualmente causare una “ernia” nel passaggio della deglutizione chiamata diverticolo di Zenker.
Procedura CPM
La miotomia cricofaringea viene eseguita in anestesia generale, in due modi: la metodologia preferita e più recente viene eseguita per via endoscopica. Utilizzando questo metodo, un “tubo” cavo e illuminato, chiamato esofagoscopio, viene inserito nella gola e nella parte superiore dell’esofago per esaminare l’area e pianificare il passaggio successivo. Quindi, uno speciale cannocchiale laser viene posizionato nell’esofago superiore. Un microscopio consente una visione ingrandita e ben illuminata dell’anello muscolare incriminato.
If a clear view cannot be achieved during esophagoscopy due to difficult patient anatomy (e.g., jaws won’t open well, small lower jaw, short neck, large upper teeth), then we return to a more traditional approach through an incision on the lower left neck. In this case, the muscle is divided from outside in. Depending on a number of issues, an associated Zenker’s diverticulum may or may not be removed at the same time.
Il laser viene utilizzato per dividere il muscolo e spezzarne la “presa”. Se la sacca di Zenker è evidente, è “marsupializzata”, il che significa che la sua apertura è allargata per essere sicuri che la sacca non trattenga il cibo, ma svuoti invece il suo contenuto direttamente nell’esofago.
A seconda del paziente e dei problemi chirurgici, un drenaggio di aspirazione può essere posizionato all’interno dell’esofago superiore e fatto uscire attraverso il naso. Un secondo tubicino per l’alimentazione può essere inserito attraverso il naso e giù nello stomaco. Una volta posizionate, entrambe le tube vengono rimosse la mattina successiva all’intervento.
Se durante l’esofagoscopia non è possibile ottenere una visione chiara a causa delle difficoltà anatomiche del paziente (ad esempio, le mascelle non si aprono bene, la mascella inferiore è piccola, il collo corto, i denti superiori grandi), si ritorna a un approccio più tradizionale attraverso un’incisione sulla parte inferiore collo sinistro. In questo caso, il muscolo viene diviso dall’esterno verso l’interno. A seconda di una serie di problemi, un diverticolo di Zenker associato può o meno essere rimosso contemporaneamente.
Cricopharyngeal myotomy (1 of 7)
Cricopharyngeal myotomy (2 of 7)
Cricopharyngeal myotomy (3 of 7)
Cricopharyngeal myotomy (4 of 7)
Cricopharyngeal myotomy (5 of 7)

Cricopharyngeal myotomy (6 of 7)
Cricopharyngeal myotomy (7 of 7)

Tasso di successo del CPM
Il tasso di successo può variare a seconda del grado in cui la persona è un candidato ideale per questo intervento chirurgico. Quando la disfagia da cibo solido è il sintomo principale e quando gli studi a raggi X mostrano il mancato rilassamento del muscolo, la procedura può ripristinare drasticamente la capacità di deglutire dell’individuo.
La soddisfazione dei pazienti per i risultati è solitamente molto elevata. “Posso mangiare di nuovo tutto ciò che voglio”, si sente spesso dopo l’intervento chirurgico. Di tanto in tanto un individuo ha più di un deficit di deglutizione, di cui il CPMD è solo uno. In questo caso, la deglutizione potrebbe essere migliore, ma non ancora perfetta dopo il CPM.
Rischi del CPM
A meno che tu non abbia problemi di salute significativi, i rischi sommati insieme sono molto piccoli. I rischi possono includere:
- Una reazione al farmaco, un problema cardiaco, ecc., durante l’anestesia generale.
- Trauma dentale: ad esempio, dente scheggiato, graffiato, rotto o spostato.
- Se l’intervento viene eseguito all’interno dell’esofago esiste un piccolo rischio di un’infezione speciale, potenzialmente grave, chiamata mediastinite. (Non abbiamo riscontrato questo problema con un totale BVI di circa 120 interventi CPM).
- Se l’intervento viene eseguito attraverso un’incisione sul collo, esiste un piccolo rischio aggiuntivo di paralisi temporanea – o raramente permanente – di una corda vocale, che viene gestita in modo relativamente semplice.
- Il “rischio” o il risultato finale è che il medico non può garantire il grado preciso di miglioramento, ovvero se il risultato sarà “buono”, “molto buono” o “spettacolare”. Ciò dipende in larga misura dalle componenti precise del problema originale; poiché il medico tende a conoscerli prima dell’intervento chirurgico, di solito può fare una stima ragionevolmente affidabile del miglioramento atteso.
Cosa aspettarsi dopo il CPM
Dopo l’intervento, i pazienti tornano a casa più tardi il giorno dell’intervento o la mattina dopo, con rare eccezioni. Naturalmente, la guida deve essere affidata ad un familiare o ad un amico. La maggior parte delle persone ha effetti collaterali minimi dell’anestesia. La nausea, ad esempio, è diventata relativamente rara.
Gli antidolorifici sono costituiti da Tylenol o Tylenol con codeina, salvo allergie o sensibilità. L’acqua può essere ingerita immediatamente dopo l’intervento chirurgico.
I primi cinque giorni la dieta dovrebbe consistere di liquidi e cibi molto morbidi. L’acqua è sempre l’ultima cosa ingerita dopo ogni “pasto”, per “risciacquare” l’area dell’intervento. Alcuni ritengono che cibi/liquidi salati o acidi brucino l’area dell’intervento.
Occasionalmente i denti sembrano un po’ doloranti e allentati, soprattutto gli incisivi centrali superiori.
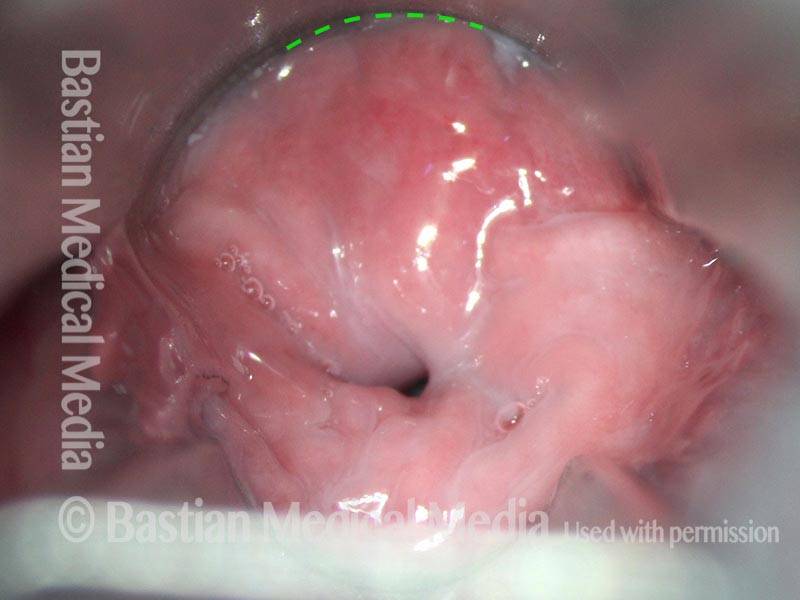
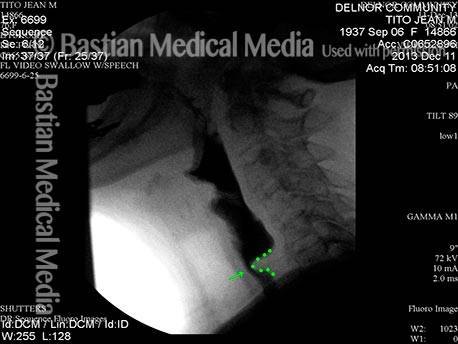
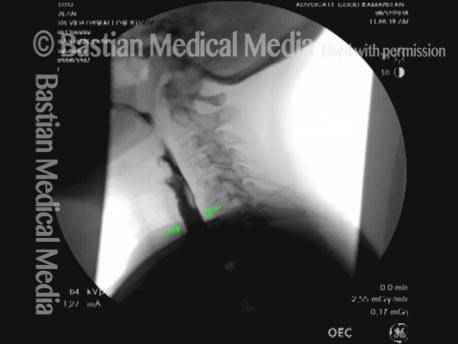
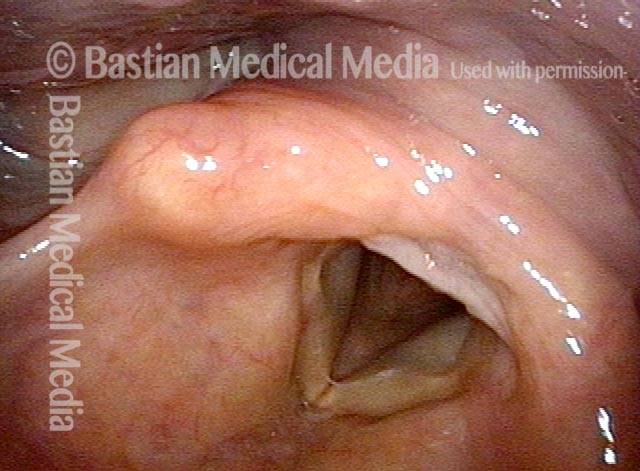
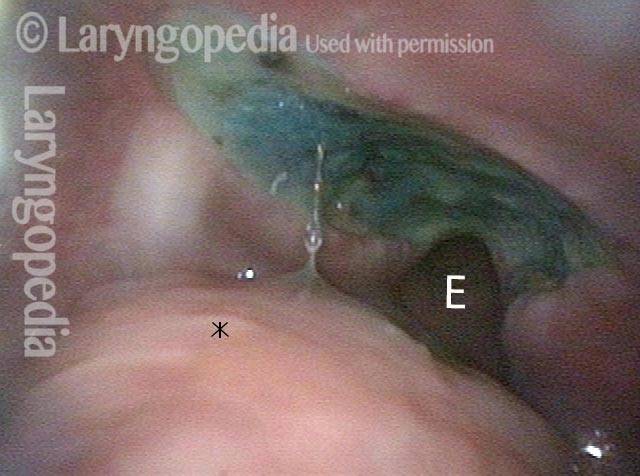
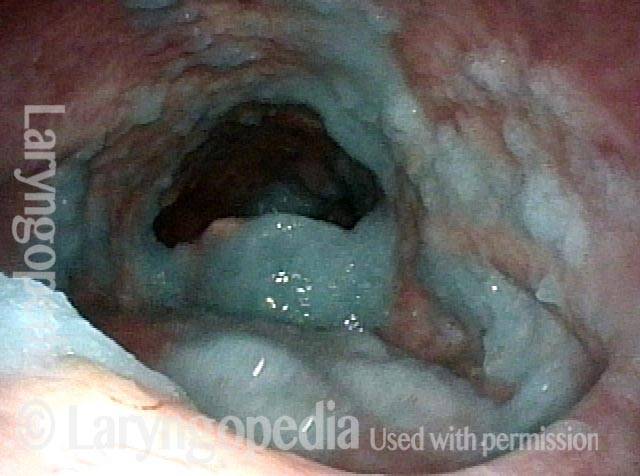
Disfunzione cricofaringea, prima e dopo la miotomia
Cricopharyngeal dysfunction: before myotomy (1 of 2)

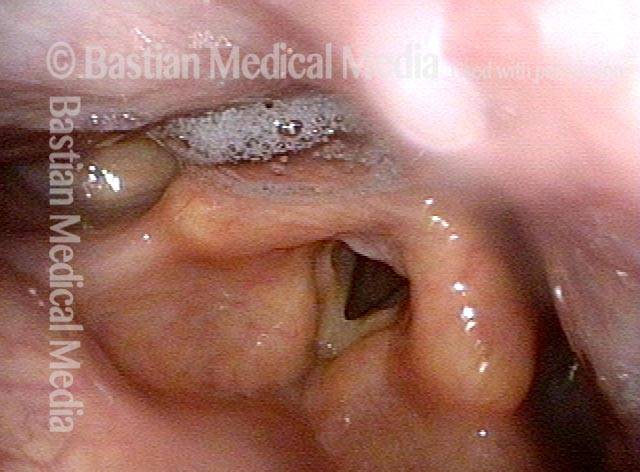
Cricopharyngeal dysfunction: after myotomy, resolved (2 of 2)

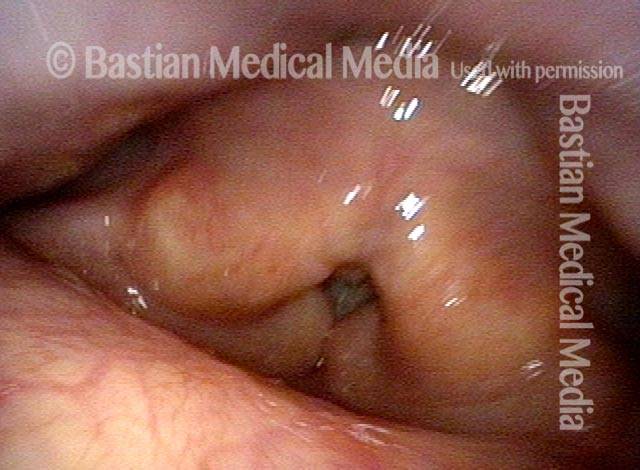
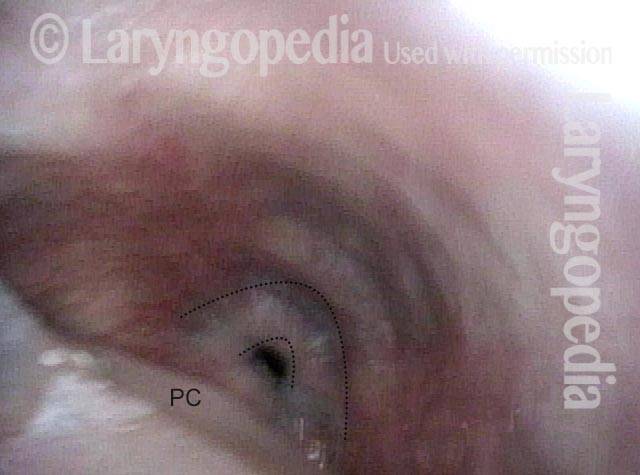
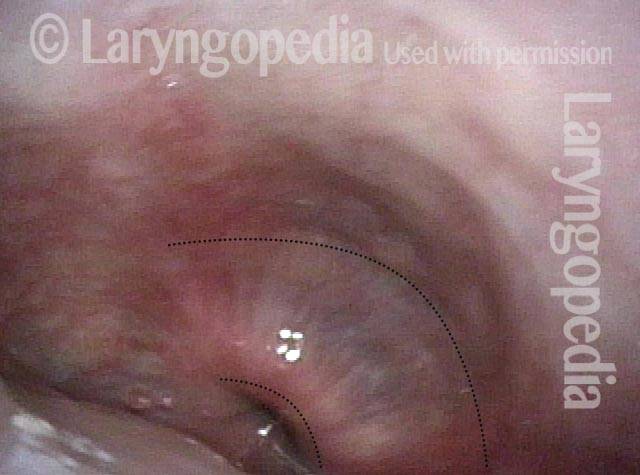
Esempio 2
Cricopharyngeal dysfunction: before myotomy (1 of 2)

Cricopharyngeal dysfunction: after myotomy, resolved (1 of 2)

Esempio 3
Cricopharyngeal dysfunction: before myotomy (1 of 2)
Cricopharyngeal dysfunction: after myotomy (2 of 2)
Miotomia cricofaringea per l’alimentazione ricreativa e la gestione della saliva
Panormaic view, post CPM (1 of 4)

Trumpet maneuver (2 of 4)
Closer view (3 of 4)
Well-managed saliva (4 of 4)

98 anni, prima e dopo la miotomia
Immediately after swallowing (1 of 10)
Zenker’s (2 of 10)
Dysphagia (3 of 10)
Residue from Zenker’s (4 of 10)

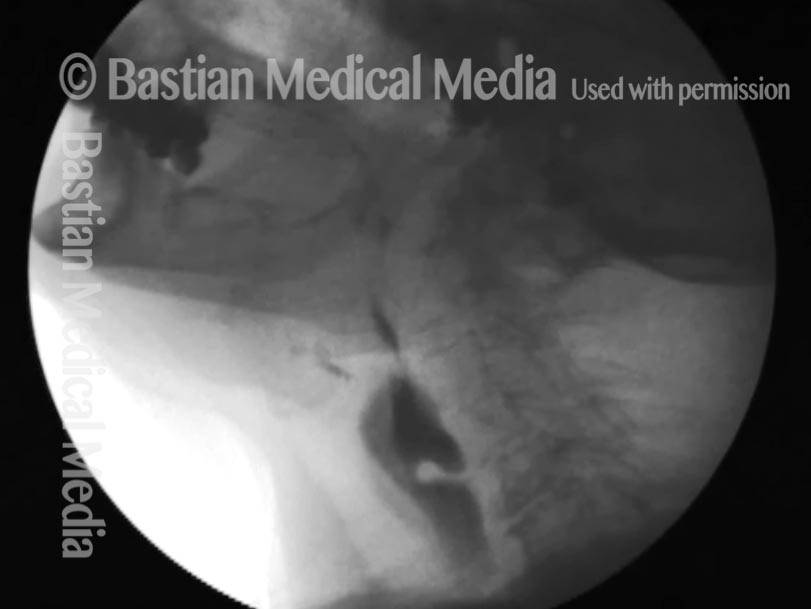
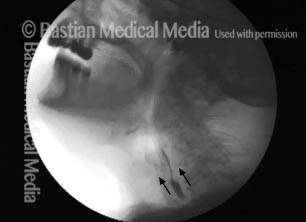
X-ray showing Zenker’s (5 of 10)
Moments later (6 of 10)
After myotomy (7 of 10)
No residue (8 of 10)

Zenker’s gone (9 of 10)

No barium in hypopharynx (10 of 10)

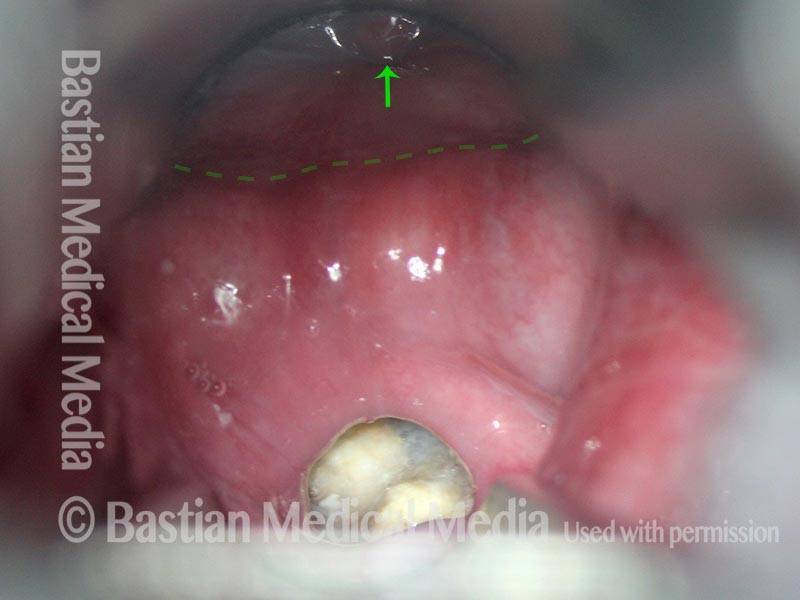
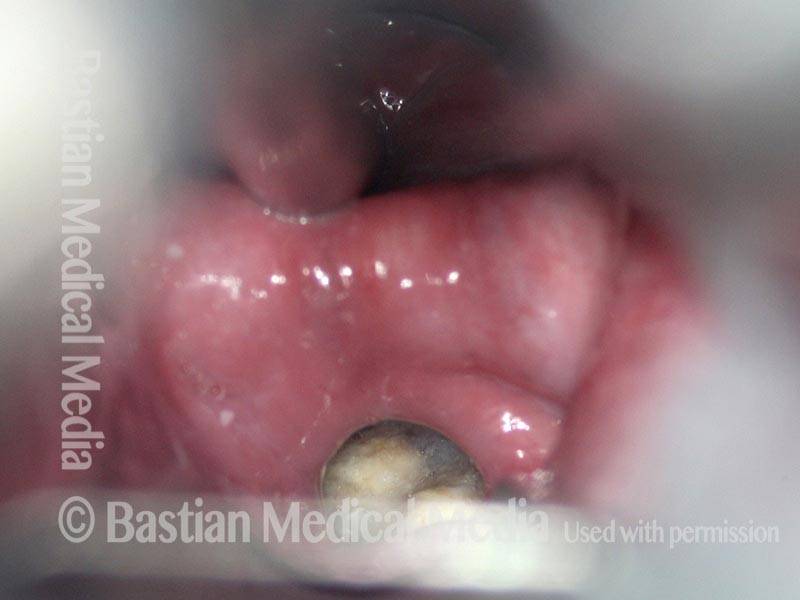
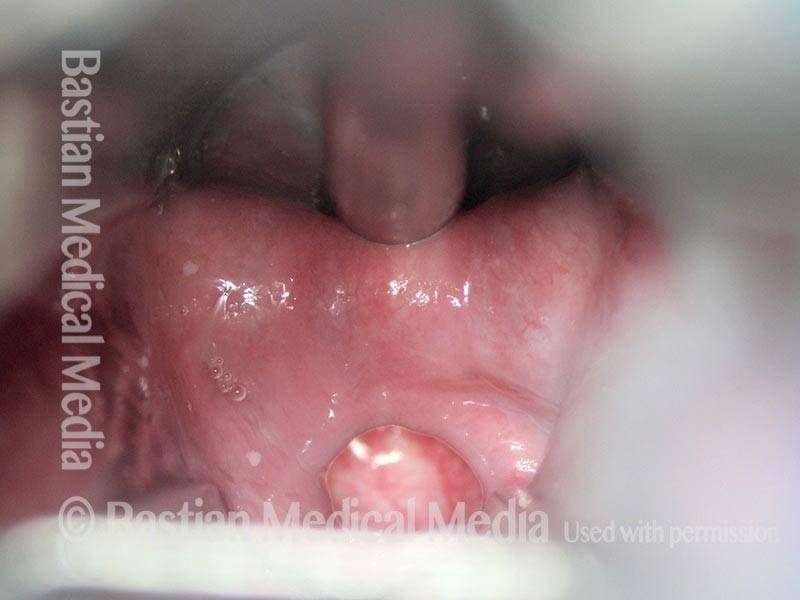
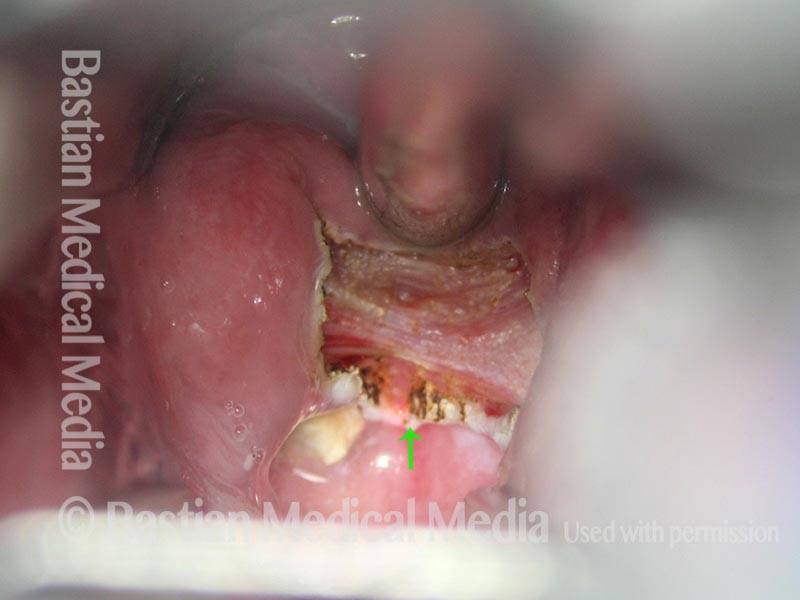
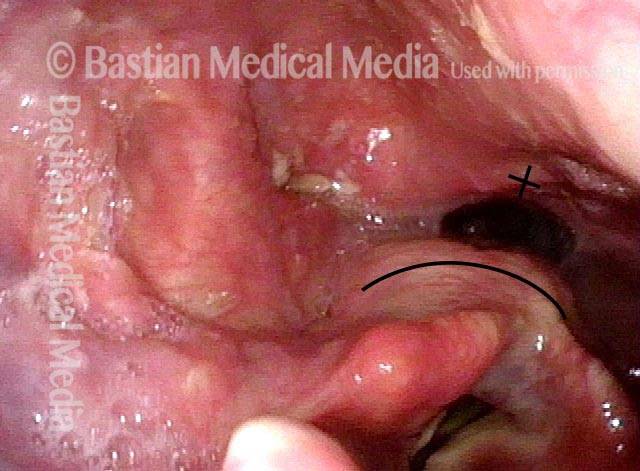
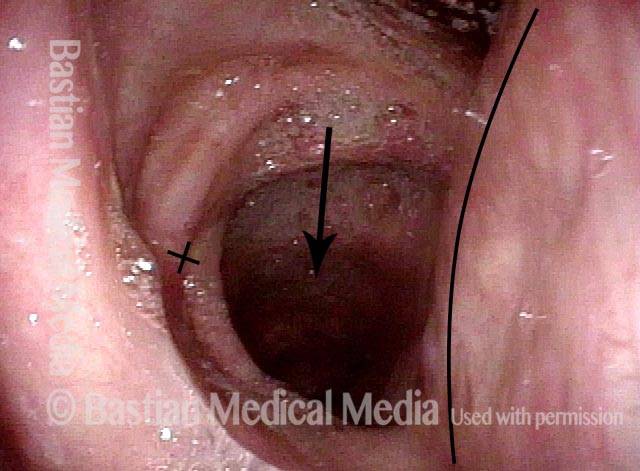
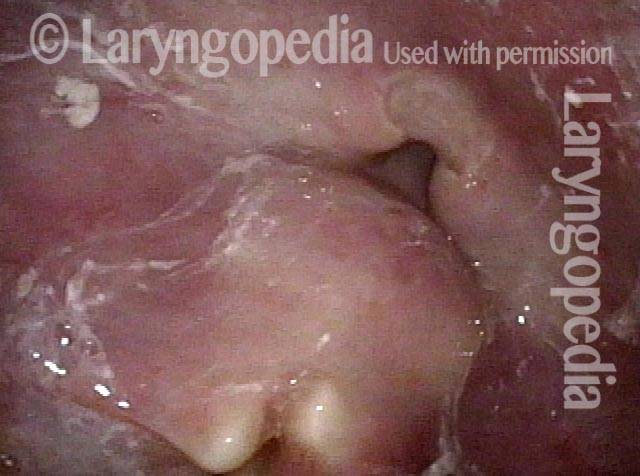
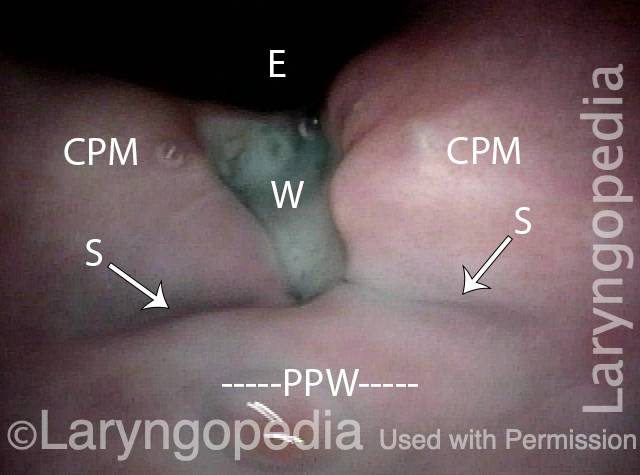
Ottima vista della ferita chirurgica della miotomia cricofaringea fresca
CPM dysfunction (1 of 4)
VFSS six years later (2 of 4)

Five days post-op (3 of 4)
Cervical esopagus (4 of 4)
Bolus Stream prima e dopo la miotomia cricofaringea
Pre-myotomy (1 of 2)

Post-myotomy (2 of 2)

Risultati VESS dopo la radioterapia
Narrowed pharyngeal wall (1 of 7)

Swallowing applesauce (2 of 7)
After sipping water (3 of 7)

Gravity aiding in swallowing (4 of 7)

Lifting larynx (5 of 7)
A closer look (6 of 7)
Gravity aiding again in swallowing (7 of 7)
L’evoluzione di una ferita da miotomia cricofaringea
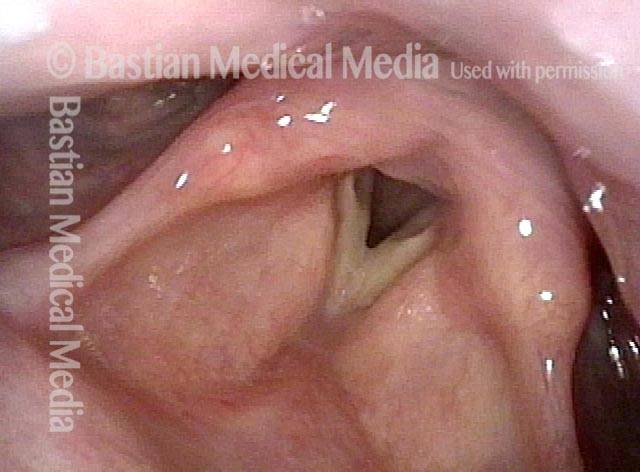
Difficulty swallowing solid foods (1 of 8)
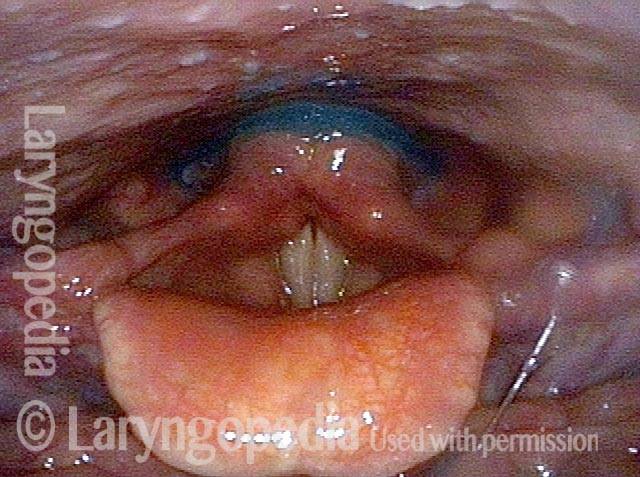
Pooled saliva (2 of 8)

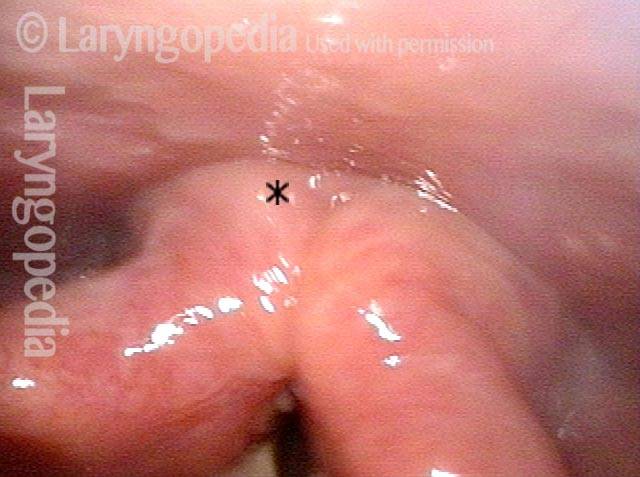
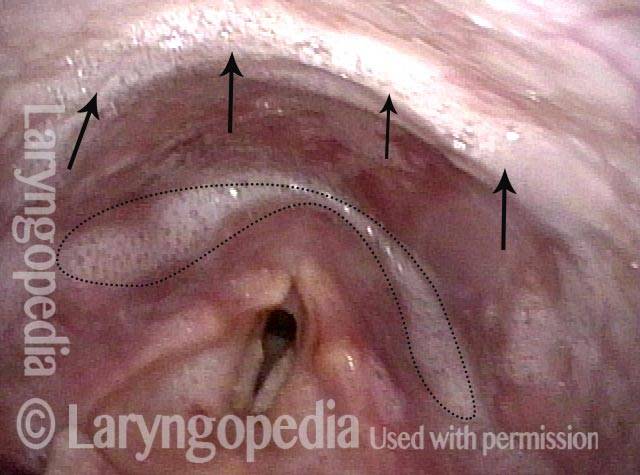
Muscle bulge (3 of 8)
Residue in swallow crescent (4 of 8)

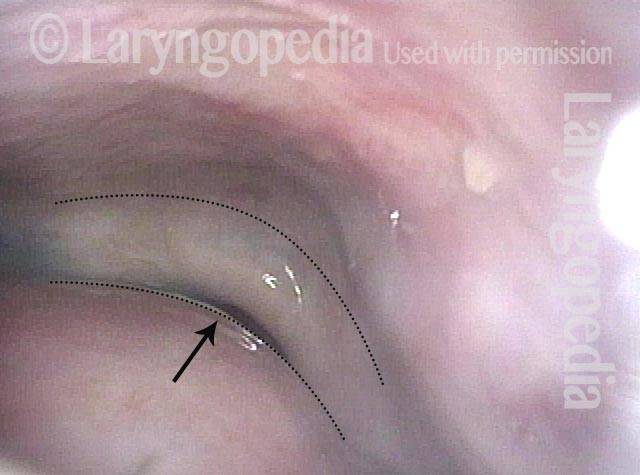
Three weeks later (5 of 8)
Residual “wound” (6 of 8)

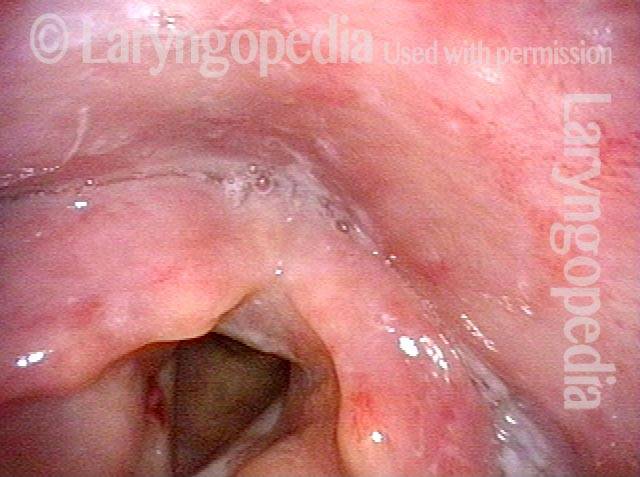
Three months post-op (7 of 8)
At close range (8 of 8)

Diverticolo di Zenker una settimana dopo la miotomia del cricofaringeo
Zenker’s Sac (1 of 3)
Zenker’s Sac (2 of 3)

Zenker’s Sac (3 of 3)