Q: What is Endoscopy?
A: Endoscopy means to “look within,” in our case either the larynx (voice box), windpipe, esophagus, and throat. This might be done for many different reasons:
- Just to see and feel something
- Take a biopsy
- Try to widen the airway
- To remove something
Some common kinds of endoscopy include microlaryngoscopy and esophagoscopy.
Q: How is the procedure accomplished?
A: This is typically performed in an operating room during general anesthesia. After you are completely asleep, a hollow, lighted “tube”—a laryngoscope for example —is placed on the back of the tongue and against the sidewall of the throat, where it rests during the procedure. There is also unavoidably considerable pressure on your teeth, despite the use of a tooth guard. In order to see clearly, a microscope may be used, and the area in question magnified and brightly illuminated. Many different tools might be used, including a laser. Sometimes medications are injected into the area or painted on it. Time required for the procedure is usually short—10 to 45 minutes of operating time, but can be longer.
Q: What are the risks of the procedure?
A: Unless you have significant health issues, risks added together are very small. The main ones are:
- A very small possibility of drug reaction, heart problem, etc., during general anesthesia
- A very small chance of dental trauma—e.g., chipped, scratched, broken, or dislodged tooth or crown. We have several instances per year of roughened enamel that doesn’t need a dentist’s attention, but only needs to be smoothed off in the O.R. Beyond this, about every couple of years something more significant happens, such as a broken or dislodged crown, bridge, or tooth. A little more often, certain teeth may feel loose in the early days after surgery but usually tighten up without further treatment.
- The third “risk” is that we cannot guarantee the precise degree of improvement. That depends primarily on the difficulty of the original problem that we have thoroughly discussed with you.
Q: The potential for harm to my teeth really bothers me.
A: Dental injury happens infrequently, but this possibility bothers us too! That’s why we use not only a tooth guard, but also all the care and gentleness we can while still getting the job done. Please keep in mind that you must NOT consent to surgery if you cannot personally accept the very small chance of a dental problem. BVI cannot assume this risk, because our reimbursement is so small in relation to the cost of dental work, and our practice has a much higher than average proportion of difficult cases. The only way for you to avoid this small risk, and its potential expense to you, is to not have the surgery.
Q: I’m also worried about my result. What is the chance I will be worse after surgery?
A: The point of surgery is to answer a question and /or to improve voice, swallowing, and breathing. Our expectations do vary a bit, however, according to what precisely we are trying to accomplish and your specific circumstance. This has been reviewed in detail with you, so that you know what to expect.
Q: Is there anything else I should know?
A: A family member or friend will have to drive you home. You may have after effects from the anesthesia medication. We typically give you a prescription for a pain medicine, often containing a narcotic such as codeine, if you are not allergic to it. The risk of nausea is reduced by having food in your stomach when you take it. Unless directed otherwise, you may eat whatever your appetite and throat discomfort allow, but eat cautiously the first time, to be sure your stomach is “settled.” Occasionally, salty or acidic food / liquids will burn the sore area caused by pressure from the laryngoscope. Most commonly, that pain will be on the left side. Occasionally the teeth feel a little sore and loose, especially your upper central incisors. In this case, we suggest that you refrain from wiggling them, or from biting into tough foods until they tighten back up on their own. Most often this takes a few days to a week or so. If you experience a lot of coughing, over-the-counter Robitussin DM suffices for most people. If that is not effective, you can call BVI for a stronger prescription.
Q: When do I see my doctor after surgery?
A: Typically, we will see you for the first postoperative visit at about a week after surgery.
Example of Microlaryngoscopy:
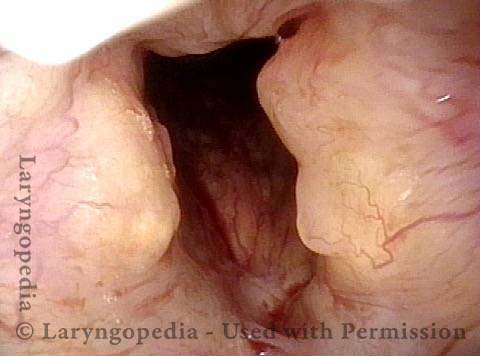
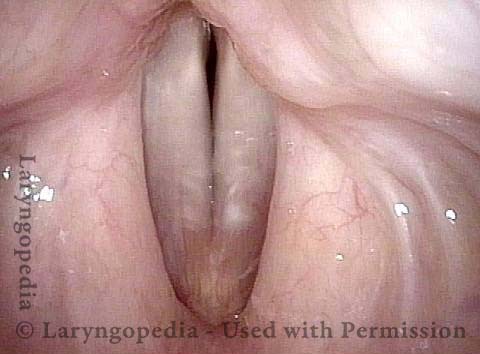
Amyloidosis of the Larynx as Seen over Time, with Treatment
Primary laryngeal amyloidosis (1 of 7)
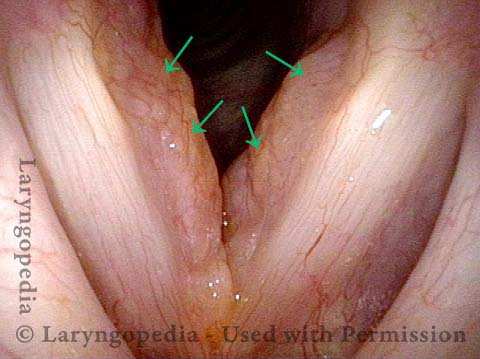
Bulky swelling (2 of 7)

Amyloidosis (3 of 7)

Amyloid deposits (4 of 7)
Vocal cords cannot close completely (5 of 7)

Amyloids Remain (6 of 7)

Voice remains clear (7 of 7)
Example of Esophagoscopy
Esophagoscopy (1 of 4)
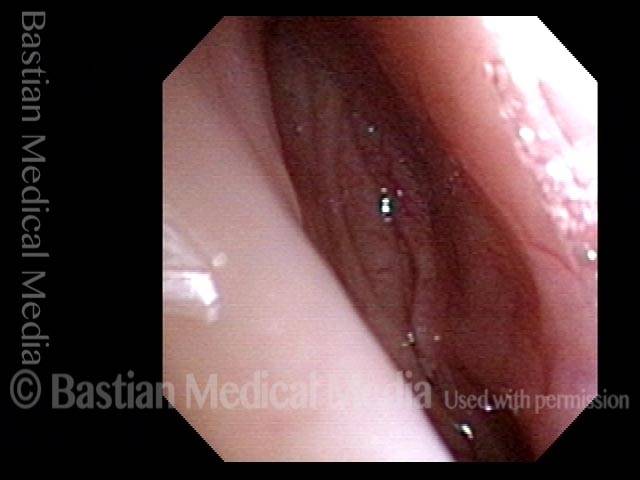
Esophagoscopy (2 of 4)

Esophagoscopy (3 of 4)

Esophagoscopy (4 of 4)
