A synthetic material, polytetrafluoroethylene, most popularly associated with non-stick cooking pans. Until 25 or so years ago, it was common to treat paralyzed vocal cords by injecting a paste of Teflon particles deep within the cords. It was an effective treatment for its time, but it occasionally caused granuloma formation and required late debulking.
Today, injected materials such as hyaluronic acid gel or hydroxyapatite particles suspended in hyaluronic acid are typically used instead for temporary or somewhat permanent rehabilitation. For permanent rehabilitation of permanent paralysis, surgically implanted silastic wedges are used most often, though other materials are also used optionally.
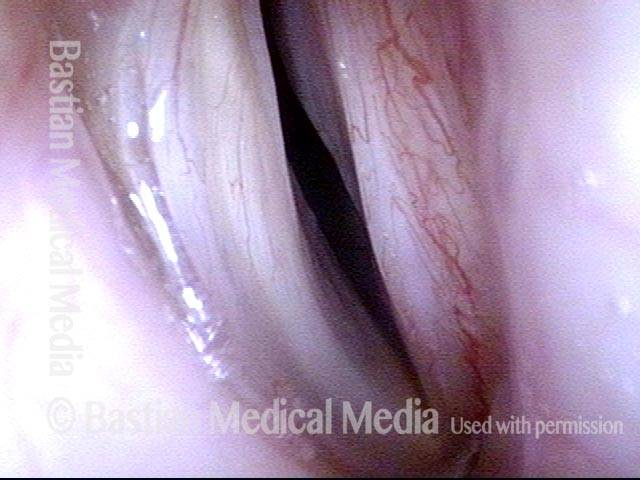
Teflon Bulge, before and after Removal
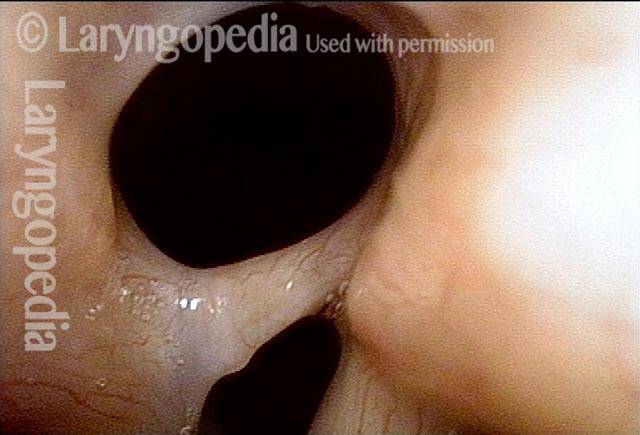
Teflon bulge (1 of 4)
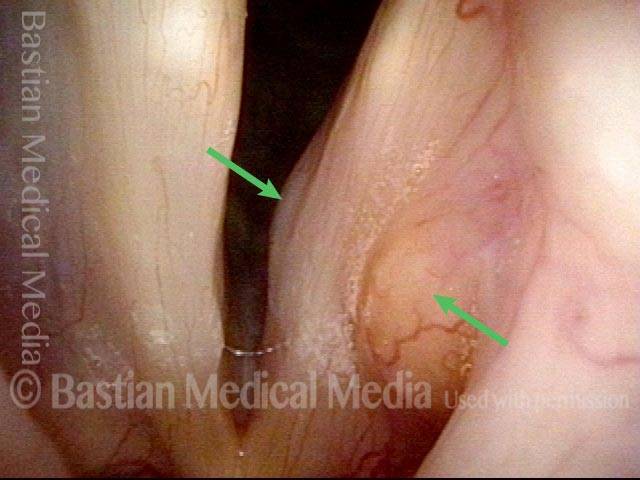
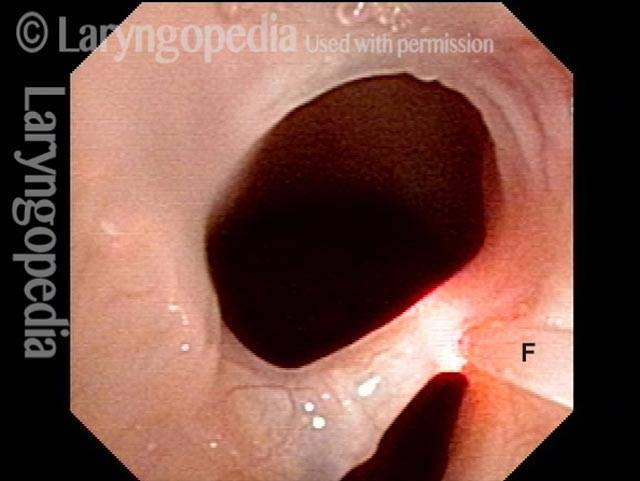
Teflon bulge (2 of 4)
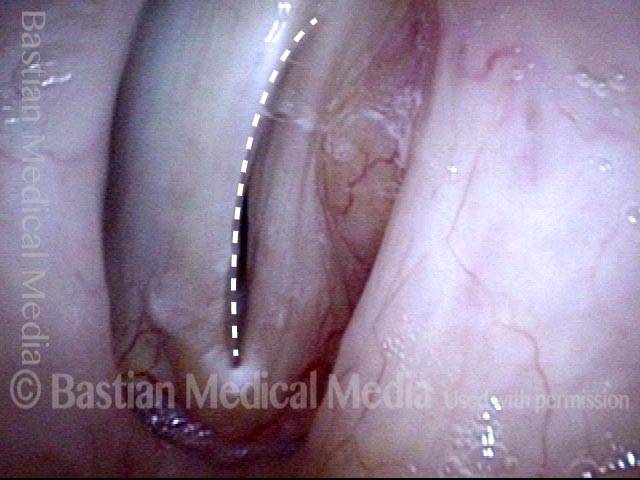
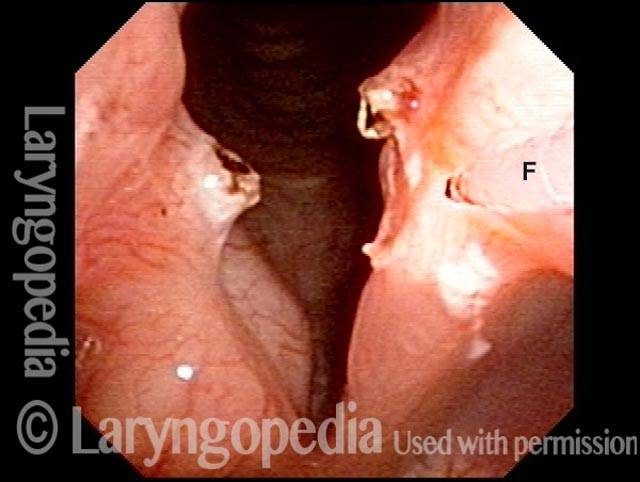
Teflon bulge: after removal (3 of 4)
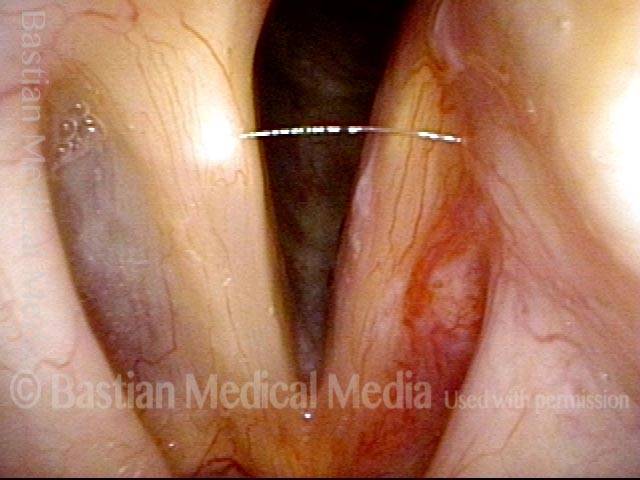
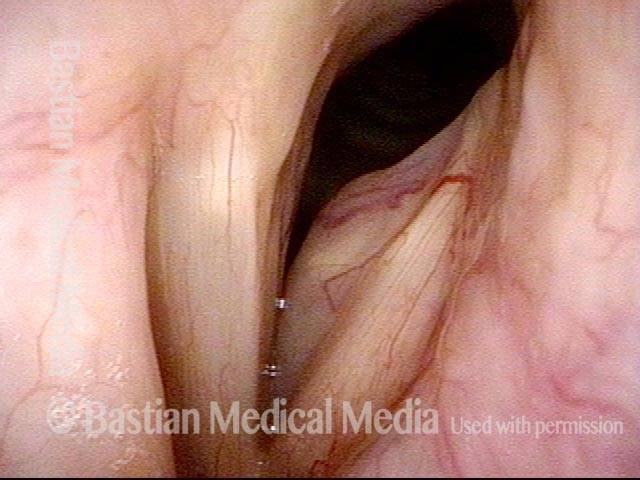
Teflon bulge: after removal (4 of 4)

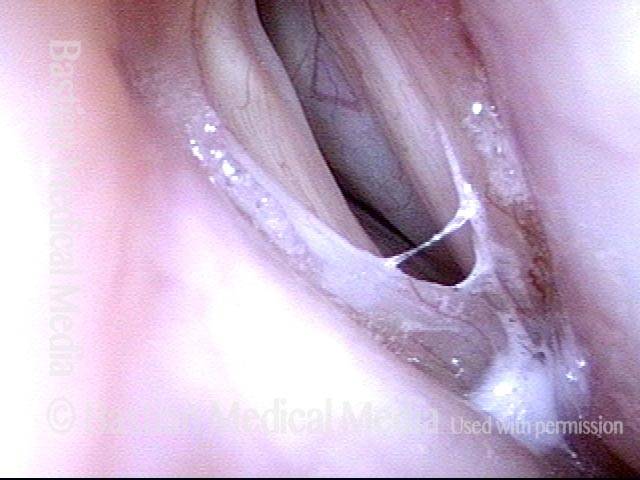
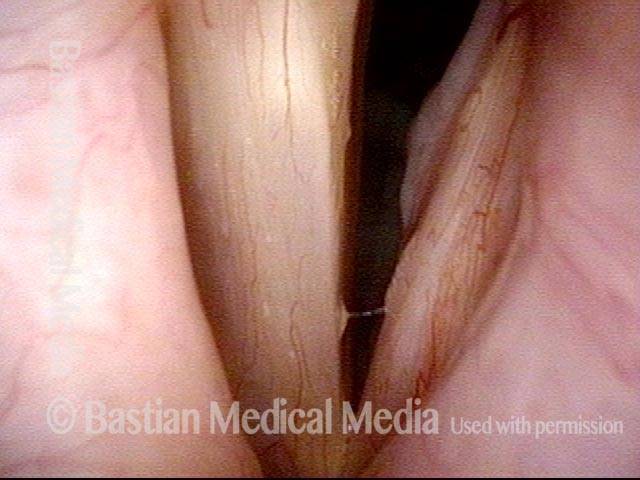
Posterior Commissure Synechiae
Tethered vocal cords (1 of 5)

Tethered vocal cords (2 of 5)
Before laser removal (3 of 5)
Immediately after laser (4 of 5)
One month post-op (5 of 5)

Audio with photos:
Interview:
The patient describes original problem with Teflon granuloma/ overinjection, and the improvement after debulking Teflon.
Teflon Bulge, before and after Treatment
Teflon bulge (1 of 5)
Teflon bulge (2 of 5)
Teflon bulge (3 of 5)

Teflon bulge: after treatment (4 of 5)
Teflon bulge: after treatment (5 of 5)