What to Expect After Botox Injection for R-CPD
Background of R-CPD
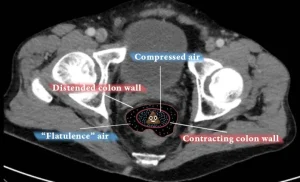
R-CPD causes 4 primary symptoms: inability to belch, gurgling noises, bloating, and flatulence. Less universal symptoms include painful hiccups, nausea after large meals, shortness of breath when very bloated, hypersalivation, and constipation. For more information, see links below.
Standard of care
This is an injection of botulinum toxin (“Botox”) into the upper esophageal sphincter through the mouth during brief general anesthesia—often a “once and done” treatment.
How Many Units of Botox Should My Doctor Should Inject for R-CPD?
Unsatisfyingly, the answer is “that depends,” for two main reasons. The first is placement. If the doctor’s is very accurate, the amount injected can be less than if inaccurate. (And any good ENT doctor should be able to aim accurately without difficulty.)
The second reason is the innate difference of individual sensitivity to Botox. It is known from other sites that one person may need a bigger dose than another to get the same result. And it doesn’t correlate with age, sex, weight, height, etc. and so there is no predicting…
In the larynx, where we inject botox for a rare neurological voice disorder, the dose varies by a factor of at least 20. Most lie in a middle range, of course, but there are “outliers” on both the “hypersensitive” and “insensitive” ends of the scale.
The muscle we are injecting is small, and that is why I initially thought that 50 units—the dose I used for my first 200 patients—was generous. That dose worked well for virtually everyone I injected. In fact, it was likely a higher dose than needed for some. But it was not enough for the very occasional patient. And so, to “capture” the rare patient who needs higher dose, I increased to 75 units for approximately the next 700 patients.
Again, a really good result followed for “almost” all 700. But for the next 150 or so, I used 100U for two reasons. One is that the patient has purchased the entire vial of 100, so I figure to just give the full amount. The second is that so many travel from such a distance (even internationally) that we want to make certain even if they are a bit insensitive to Botox, they still get a good result…
So many patients would do fine with 50 or even 75, but the above reasons explain my current dose of 100. To repeat, keep in mind it is not only dose but – critically – accurate placement that may determine the effectiveness of any given injection. Thankfully targeting is only occasionally difficult, so most people will do well with 50, 75 or 100. If we could know in advance each individual’s dose requirement, I am sure some would do well even with 25 units!
Is there any downside to using a higher dose than (in retrospect) would have been necessary? The only downside of higher dose would be a bit more of the initial “slow swallow” which everyone gets through…
Logistics of the Procedure under General Anesthesia
This will vary according to where you have the procedures done. Time required at most surgicenters will likely be 2 to 3 hours, while the procedure itself, from preop holding to O.R. to recovery room might be about 30 minutes. It is not likely strong pain medicine would be needed for most people. As for diet, most doctors will probably tell you to be guided by your throat and stomach. Key additional things to know:
There will be no relief of R-CPD symptoms for 1—5 days
Only when micro-burps begin do patients start to notice the beginning of symptom relief. So do not try carbonation for lunch on the day of the injection!
Initial Botox side effects can be “weird” for a few days to weeks
Most are joyful due to the ability to belch and relief of bloating, but just so that nobody is surprised:
- Burping can be excessive. Some say burps happen spontaneously if they yell, clear the throat, or laugh loudly—or even breathing out after having taken a deep breath. Most say it is funny or cause for celebration. Rarely, burps can include some regurgitation, too. If present, these are expected to subside within days to weeks.
- Swallowing is peculiar initially, especially for solid foods. The limp cricopharyngeus muscle (sphincter muscle) allows food to “hang” in the throat, causing an off-putting sensation of the food remaining in your throat. If this happens, the food is in the correct place; it is in a safe place. It is not “stuck.” To manage this, always have liquid in front of you while eating. If you feel that “hanging” sensation, take a sip of water to chase the food through until this side effect soon subsides.
- Very occasionally, swallowing is more than peculiar, and the person views it as problematic. This is for maybe 1% of persons who undergo the procedure. They may consume mostly liquids and smoothies for the first few weeks to avoid the “hanging” feeling, or because food seems to push back up into the throat after swallowing. This does not mean anything bad.
- A heavy or swollen sensation in the mid-to-low neck coming from “limp muscle.” If present in initial days to weeks, some R-CPD patients feel like there is a phantom wad of phlegm or swelling in the throat. Repeated swallowing or throat clearing will not help. Instead, sip water or even try to ignore this sensation.
- Amplified or unmasked acid reflux symptoms. Where reflux symptoms increase early post-injection, the Botox injection did not cause this but rather unmasked it. Years of constant upward pressure on the lower esophageal sphincter as your body tries unsuccessfully to burp eventually damages / stretches the muscular valve at the bottom of the esophagus. This has been concealed to some degree because the acid travel upwards has been limited by trapped air and the malfunctioning / non-relaxing upper sphincter. Once burping can happen, acid can travel farther up the esophagus, accentuating heartburn, or a sour burp can now reach the mouth. This can be managed with an acid reducer medication like Prilosec OTC (omeprazole) until it subsides in a few weeks.
- Voice change: This rarely happens with O.R. injections and occasionally happens after EMG guided injection in an office setting. The explanation would be minor diffusion into laryngeal muscles.
- Noisy breathing during exertion or at night while sleeping. Again, this should be truly rare for O.R. injections.
- Laryngospasm (rare). This is extremely unlikely but can occur.
Are there potential complications from the Botox Injection?
The risk is extremely small. Watch Complications Compared to Expected Early Botox Effects in Treatment of R-CPD in the side bar explaining the few complications—at Bastian Voice Institute—in the first 1200 patients through January 2023.
How do I practice burping?
If you can manipulate your gurgles prior to Botox treatment, to make them softer or louder, use that technique to see if you can hurry burps along or make them bigger. Some tuck the chin, turn the head sharply to one side or the other, lower the larynx as if yawning. The trick seems to be to provide a little “help” for the burps without interfering with them. It is as though you are at the same time facilitating them and letting them happen, not “making them happen.”
Follow-up after the procedure
Each doctor will have his or her own schedule for this. An example of intervals might be 1 week, 6 weeks, 3 months, 6 months, and yearly. Things we want to know:
- Can you burp?
- Are you still gurgling?
- Is the bloating/abdominal distention gone?
- Is the flatulence diminished?
- What about hiccups, shortness of breath, hypersalivation, constipation (if you had these)?
- On a 7-point scale, what is the level of the residual problem? (Most have said it was a 6 or 7 pre-treatment.)
- Would you rate the improvement subtle, small, medium, or large?
- Anything else you want to say or ask.

How to Keep the Ability to Burp After Botox Treatment for R-CPD
R-CPD can thankfully be treated successfully with a simple outpatient injection of Botox into a muscle in the upper esophagus. Since the Botox effect on the muscle serves as “training wheels” for burping, about 4 out of 5 people are “cured” by a single treatment. That’s why we aim for “once and done” treatment.
Dr. Bastian describes here how to maximize the likelihood that the ability to burp will continue after Botox has worn off.

Can’t Burp? This May Explain Why
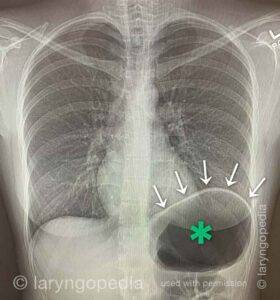
You may have R-CPD or retrograde cricopharyngeus dysfunction. In this condition, the upper esophageal sphincter (cricopharyngeus muscle) works normally from above to permit swallowing, but it refuses to relax from below to let air be belched out.
In-Office Injection of Botox for R-CPD | EMG-Guidance Compared to O.R. Esophagoscopy
There are two main approaches in treating R-CPD: one performed under brief general anesthesia through the mouth in an operating room, and another done in a clinic setting by injecting through the front or side of the lower neck using EMG (electromyographic) guidance with partial local anesthesia.
In this video, Dr. Bastian explains both techniques, with a special focus on the EMG-guided office procedure.
Complications Compared to Expected Early Botox Effects in Treatment of R-CPD
In this video, Dr. Bastian distinguishes the difference between early EFFECTS that are expected, and COMPLICATIONS patients have experienced in a caseload of approximately 870 people. This informal discussion will likely reassure persons considering this treatment for the severe daily misery caused by R-CPD.
Teleconversation with Dr Bastian
Still have questions? Schedule a call with Dr. Bastian via Zoom.Share this article
Read Additional Entries