Photo Essays of Zenkers Diverticulum
Zenker’s diverticulum (1 of 4)
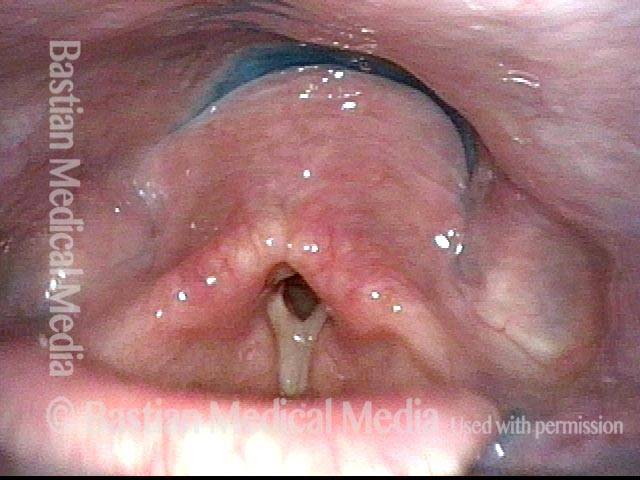
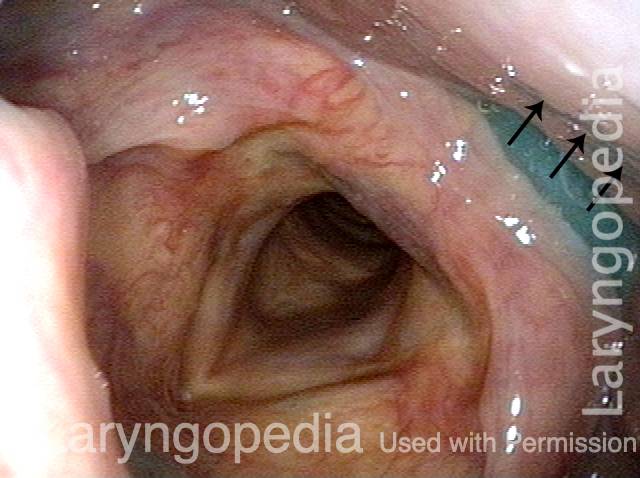
This middle-aged woman has had a known Zenker’s diverticulum for several years. She has now reached a point of frustration that has motivated her to proceed with cricopharyngeus myotomy. The series that follows explains some of the reason for her frustration. In this view, the patient has just completed a swallow of her saliva.

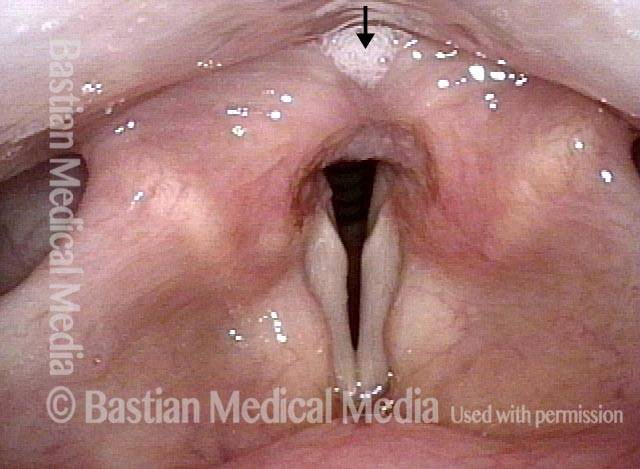
Saliva from Zenker’s sac (2 of 4)
A few seconds later, saliva begins to return upwards into the post-arytenoid area (at arrow) from the Zenker’s sac.
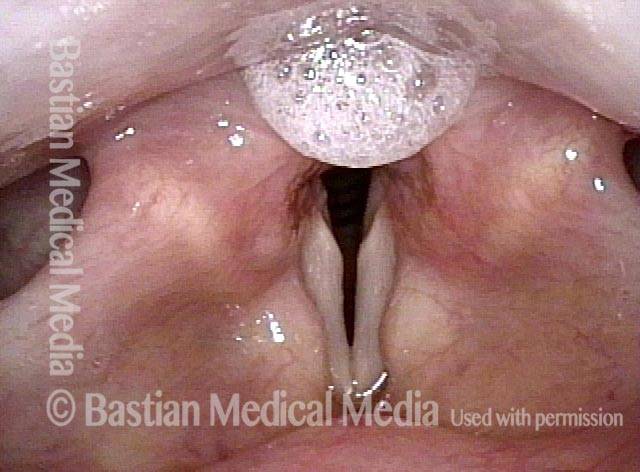
More saliva (3 of 4)
Less than a second later, more saliva comes upward from the Zenker’s sac.
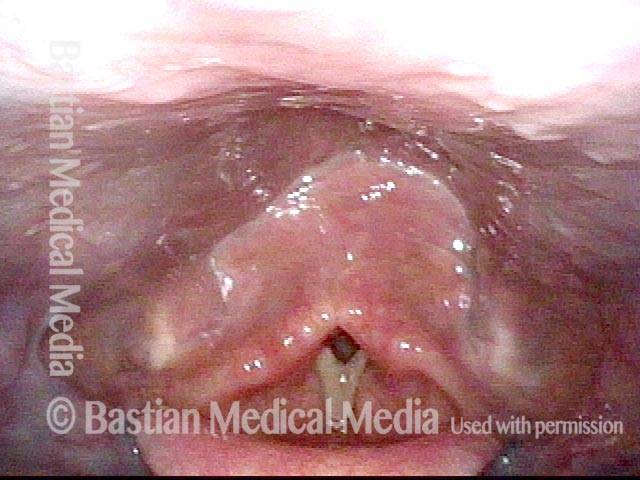
Forced to re-swallow (4 of 4)
A few seconds later, sufficient saliva has welled up from the sac that the patient is forced to re-swallow, taking her back to the appearance of the first photo in this series, only to begin the same cycle depicted in these four photos again and again.

Example 2
Zenker’s diverticulum (1 of 3)
This view is a moment after a completed swallow of blue-stained applesauce.

Postcricoid area (2 of 3)
Same view, a second later, as blue-stained applesauce emerges from the Zenker’s diverticulum upward (toward the camera) into the postcricoid area.

Hypopharynx (3 of 3)
Another second later, applesauce continues to re-emerge into the hypopharynx.

Post-swallow Return of Saliva into the Hypopharynx
This man began to experience solid food lodgment a few years earlier, along with gurgling noises every time he swallows. Even on an initial examination, Zenker’s diverticulum can be strongly suspected based on the findings of the videoendoscopic swallow study (VESS). Upon review of a videofluoroscopic swallow study (VFSS), a Zenker’s diverticulum is indeed the explanation for the findings below, which went away completely (return of saliva, gurgling noises, and food lodgment) after myotomy.
Pooling of saliva (1 of 4)
Upon first visualization of the hypopharynx and larynx, organized pooling of saliva is seen in the post-arytenoid area.

Saliva disappears after swallow (2 of 2)
Right after swallowing, all of the saliva disappears. The following 2 photos can be harvested within one second of completion of the swallow.

Saliva begins to return (3 of 3)
Here, the saliva begins to return from a presumed Zenker’s diverticulum.

Saliva is ejected upwards from Zenker’s sac (4 of 4)
Either spontaneously, or by gentle pressure on the low neck, much more saliva is ejected upwards from the presumed Zenker’s sac. This is seen commonly when there is a Zenker’s diverticulum, which, again, was subsequently diagnosed here. All of his symptoms and these findings vanished after myotomy.

Reflux Into Hypopharynx, Characteristic of Cricopharyngeal Dysfunction
Reflux into hypopharynx (1 of 3)
The patient has swallowing problems typical of cricopharyngeal dysfunction. This swallow study reinforces that impression as well as the likely presence of a Zenker’s diverticulum. In this photo, blue-stained water has just been swallowed, and the vocal cords are beginning to open. At this point, the hypopharynx contains no residue.
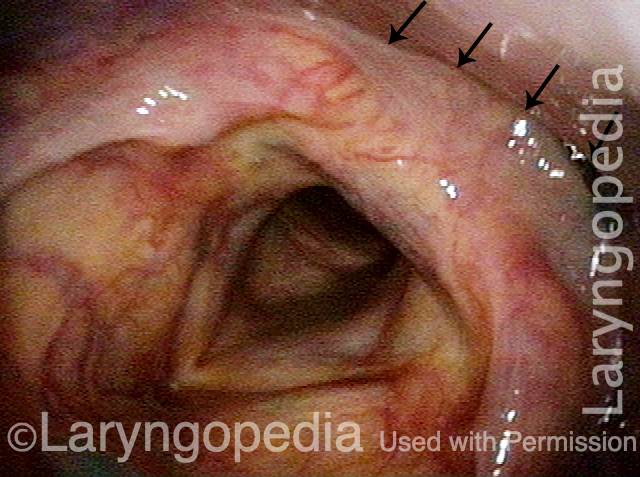
Water flows into the swallowing crescent (2 of 3)
One second later, the blue-stained water begins to emerge from just above the cricopharyngeus muscle into the “swallowing crescent”.
Larynx opens up (3 of 3)
Another two seconds later, the larynx has fully opened post-swallow. The post-swallow hypopharyngeal re-emergence of the blue-stained water is apparent.

Videoendoscopic View of Zenker’s Sac Opening and Cricopharyngeus Bar
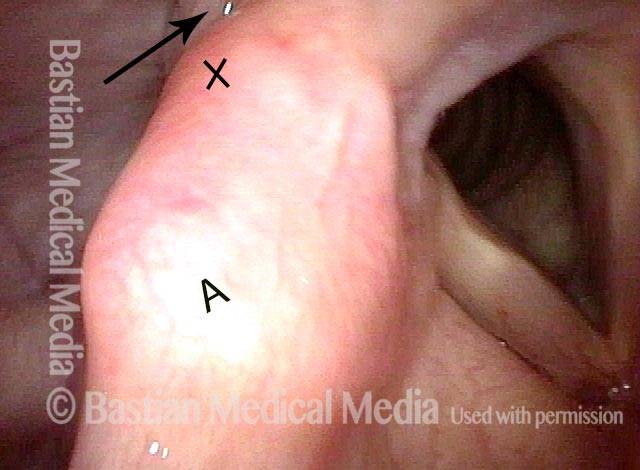
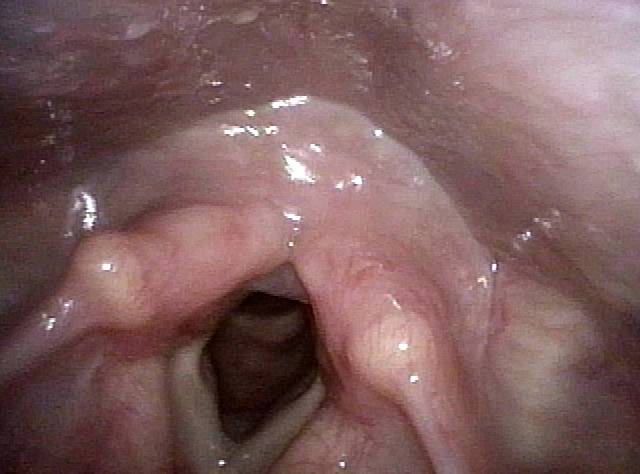
Orientation (1 of 4)
The ‘X’ is for orientation with next photo; ‘A’ is for right arytenoid eminence (left of photo). The arrow points to the area of focus of the next photo.
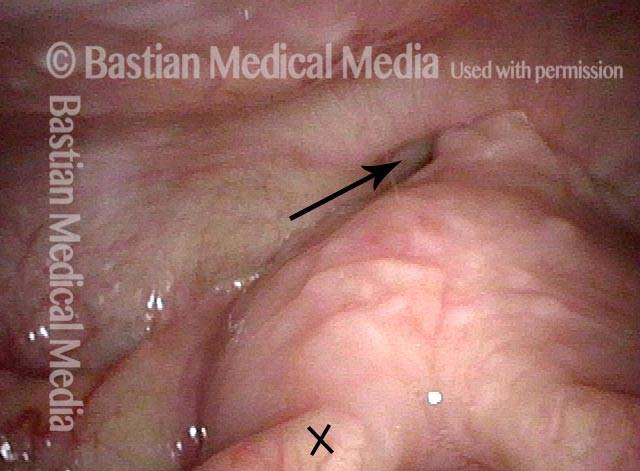
View into post-arytenoid and post-cricoid area (2 of 4)
View into post-arytenoid and post-cricoid area. The ‘X’ orients to the same place in photo 1. The esophageal entrance is just beginning to appear at the arrow.
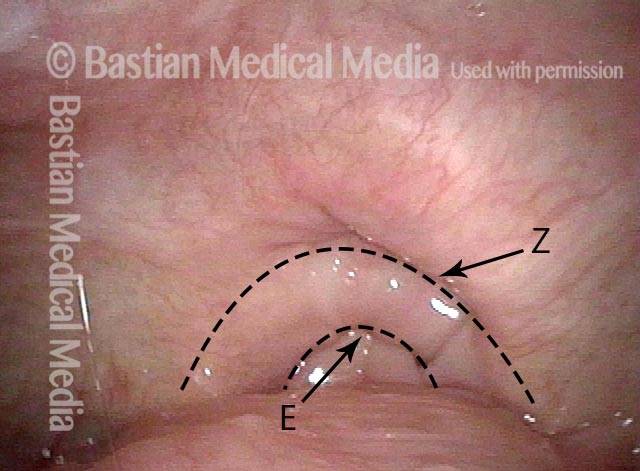
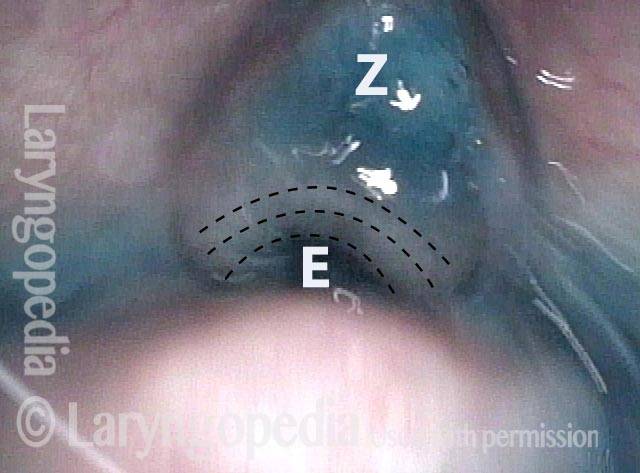
Esophageal and Zenker sac openings (3 of 4)
Descending further, we see two potential openings. ‘E’ designates actual esophageal opening and ‘Z’ the opening to the Zenker’s sac. Between the dotted lines is the cricopharyngeus muscle bar.
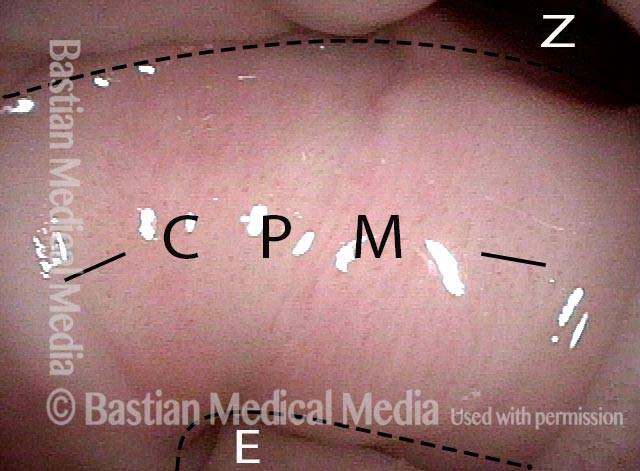
Cricopharyngeus muscle bar (4 of 4)
At very close range. Esophageal entrance is indicated at ‘E’ and the Zenker’s sac opening at ‘Z’ with the cricopharyngeus muscle bar (CPM) separating the two.
Cricopharyngeus Non-Relaxation and Zenker’s Sac Seen During VESS
Immediately after swallow (1 of 4)
During VESS, after administration of several boluses of blue-stained applesauce. Trace applesauce on pharyngeal walls, immediately after a completed swallow. The postcricoid area is “clean” in this view, at *.

One second later (2 of 4
Approximately a half second later, applesauce appears at the *, having been ejected upwards from a presumed Zenker’s diverticulum.

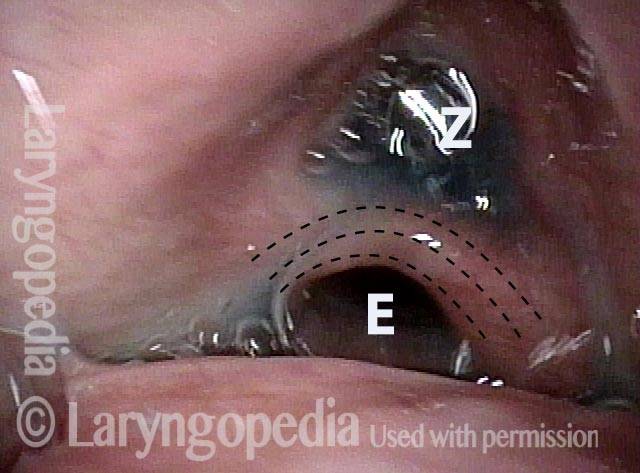
Un-relaxed cricopharyngeus muscle (3 of 4)
During water administration, a glimpse of the un-relaxed cricopharyngeus muscle is seen (concentric dotted lines). Esophageal entrance at ‘E’ and Zenker’s pouch, still containing some previously-administered blue applesauce, at ‘Z’.
More water (4 of 4)
After several more boluses of blue-stained water, the applesauce has mostly washed away, and the same findings of photo 3 are seen more clearly.
Zenker’s Diverticulum Returns Its Contents Upwards to the Throat After Each Swallow
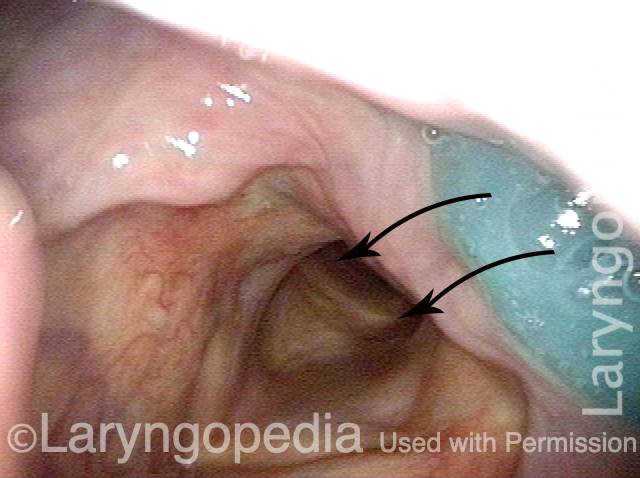
VESS (1 of 3)
During Videoendoscopic swallow study (VESS), this patient has just swallowed blue applesauce. It has disappeared downwards (arrows) into the upper esophagus but part of it is retained in a Zenker’s diverticulum (out of view).
Swallowing Crescent (2 of 3)
Exactly one second later blue applesauce appears in the swallowing crescent as the sac empties a part of its contents upwards.
Applesauce spills into airway (3 of 3)
One second later, even more blue applesauce has emerged. If it were more liquid, it would spill forward to enter the airway. This explains the constant throat clearing and re-swallowing of persons with Zenker’s diverticula (caused by antegrade cricopharyngeus dysfunction).
Post-swallow Hypopharyngeal Reflux (Zenker’s Diverticulum): VESS vs. VFSS
VESS (1 of 7)
In a patient with a known Zenker’s Diverticulum, who has just finished swallowing blue-stained applesauce during VESS.

Reflux (2 of 7)
Less than a second later, the applesauce and some saliva bubbles reflux upwards from the Zenker’s sac into the postarytenoid area.

Post-swallow (3 of 7)
Here, the patient has just swallowed a cheese cracker.
Reflux of cracker (4 of 7)
About a second and a half later, this material, mixed with saliva, returns from the sac.

VFSS (5 of 7)
Just after the patient has swallowed a bolus of barium.

X-Ray (6 of 7)
A second later, barium is “squishing” upwards from the sac.

Continued reflux (7 of 7)
Additional barium has come upwards into the postarytenoid area (compare with Photos 2 and 4).